Strengths Against Psychopathology in Adolescents: Ratifying the Robust Buffer Role of Trait Emotional Intelligence

 ,
, 
 ,
, 
Abstract
1. Introduction
1.1. Mental Health in Adolescence
1.2. Trait Emotional Intelligence and Mental Health
1.3. Mindfulness and Psychopathology
1.4. Irrational Beliefs: Catastrophizing
1.5. Relationships between Emotional Intelligence, Mindfulness, and Catastrophizing
1.6. Cross-Cultural Differences on Studies Variables
2. Materials and Methods
2.1. Participants
2.2. Variables and Instruments
2.3. Procedure
2.4. Data Analyses
3. Results
3.1. Mean Scores, Internal Consistencies, and Bivariate Correlations
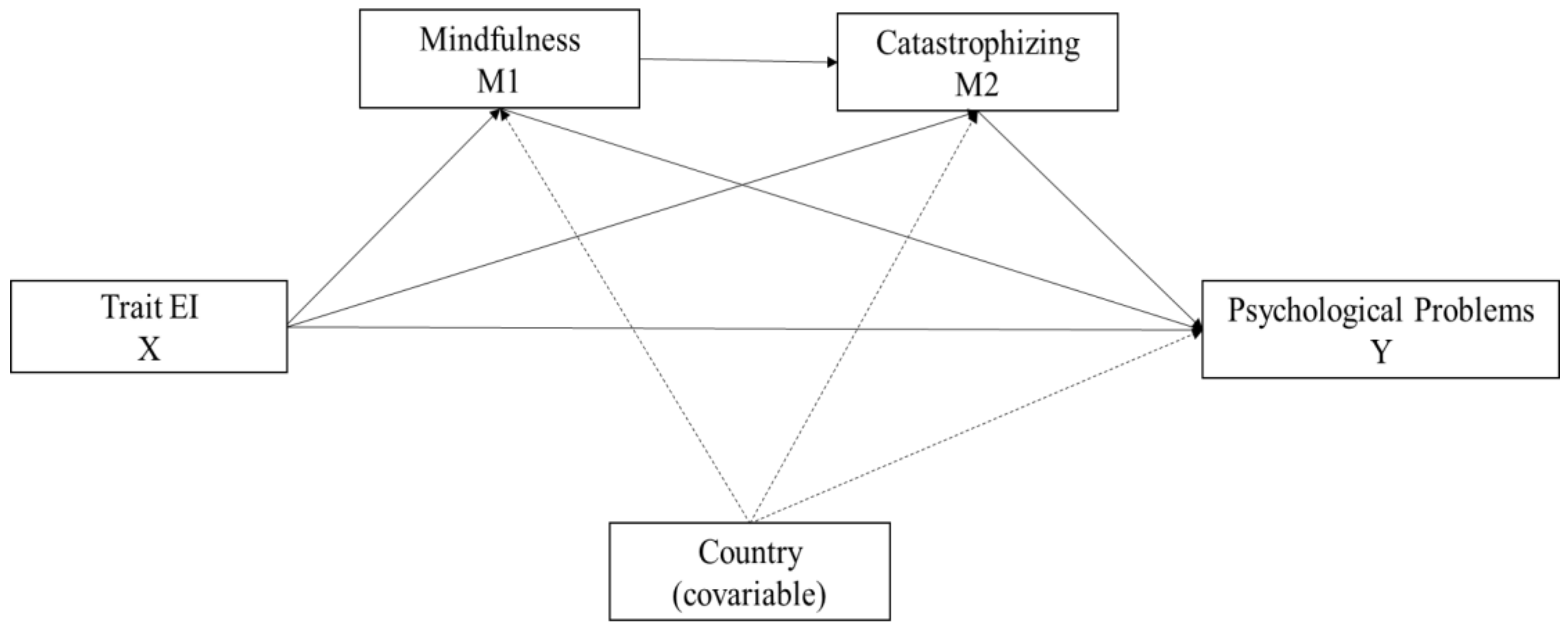
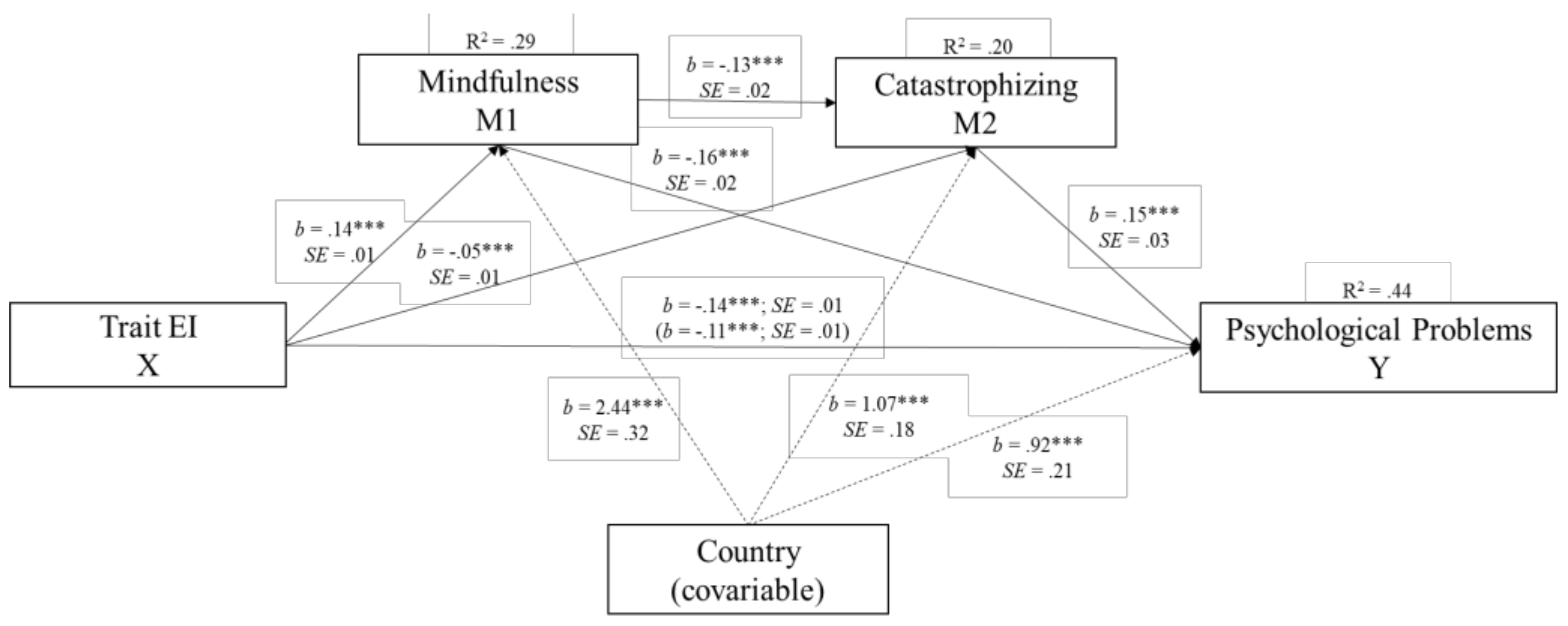
3.2. Mediation Anaylisis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Becker, A.; Döpfner, M.; Heiervang, E.; Roessner, V.; Steinhausen, H.C.; Rothenberger, A. Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: Research findings, applications, and future directions. J. Child Psychol. Psychiatry 2008, 49, 251–275. [Google Scholar] [CrossRef]
- Ortuño-Sierra, J.; Fonseca-Pedrero, E.; Paíno, M.; Aritio-Solana, R. Prevalence of emotional and behavioral symptomatology in Spanish adolescents. Rev. Psiquiatr. Salud. 2014, 7, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Ortuño-Sierra, J.; Fonseca-Pedrero, E.; Sastre i Riba, S.; Muñiz, J. Patterns of Behavioural and Emotional Difficulties through Adolescence: The Influence of Prosocial Skills. An. Psicol-Spain 2017, 33, 48–56. [Google Scholar] [CrossRef]
- Kessler, R.C.; McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; Aguilar-Gaxiola, S.; Obaid, A.; Alonso, J.; Angermever, M.; et al. Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Brit. J. Psychiat. 2010, 197, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Mayer, J.D. Emotional intelligence. Imagin. Cogn. Pers. 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Petrides, K.V.; Furnham, A. Trait emotional intelligence: Psychometric investigation with reference to established trait taxonomies. Eur. J. Personality 2001, 15, 425–448. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between emotional intelligence and health. Pers. Indiv. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Davis, S. Emotional intelligence in adolescence and early adulthood. In An Introduction to Emotional Intelligence; Dacree Pool, L., Qualter, P., Eds.; Wiley: Chichester, West Sussex, UK, 2018; pp. 105–122. [Google Scholar]
- Petrides, K.V.; Gómez, M.G.; Pérez-González, J.C. Pathways into psychopathology: Modeling the effects of trait emotional intelligence, mindfulness, and irrational beliefs in a clinical sample. Clin. Psychol. Psychother. 2017, 24, 1130–1141. [Google Scholar] [CrossRef]
- Keefer, K.V.; Saklofske, D.; Parker, J.D.A. Emotional Intelligence, 729 Stress and Health: When the Going Gets Tough, the Tough Turn to Emotions. In An Introduction to Emotional Intelligence; Dacree Pool, L., Qualter, P., Eds.; Wiley: Chichester, West Sussex, UK, 2018; pp. 161–731. [Google Scholar]
- Petrides, K.V.; Mikolajczak, M.; Mavroveli, S.; Sanchez-Ruiz, M.J.M.J.; Furnham, A.; Pérez-González, J.C. Developments in trait emotional intelligence research. Emot. Rev. 2016, 8, 335–341. [Google Scholar] [CrossRef]
- Kotsou, I.; Nelis, D.; Gregoire, J.; Mikolajczak, M. Emotional plasticity: Conditions and effects of improving emotional competence in adulthood. J. Appl. Psychol. 2011, 96, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczak, M.; Avalosse, H.; Vancorenland, S.; Verniest, R.; Callens, M.; Van Broeck, N.; Fantini-Hauwel, C; Mierop, A. A nationally representative study of emotional competence and health. Emotion 2015, 15, 653. [Google Scholar] [CrossRef] [PubMed]
- Pérez-González, J.C.; Sanchez-Ruiz, M.J. Trait emotional intelligence anchored within the big five, big two and big one frameworks. Pers. Indiv. Differ. 2014, 65, 53–58. [Google Scholar] [CrossRef]
- Lea, R.G.; Qualter, P.; Davis, S.K.; Pérez-González, J.C.; Bangee, M. Trait emotional intelligence and attentional bias for positive emotion: An eye tracking study. Pers. Indiv. Differ. 2018, 128, 88–93. [Google Scholar] [CrossRef]
- Resurrección, D.M.; Salguero, J.M.; Ruiz-Aranda, D. Emotional intelligence and psychological maladjustment in adolescence: A systematic review. J. Adolesc. 2014, 37, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Poulou, M.S. How are trait emotional intelligence and social skills related to emotional and behavioural difficulties in adolescents? Educ. Psychol-UK. 2014, 34, 354–366. [Google Scholar] [CrossRef]
- Stamatopoulou, M.; Galanis, P.; Tzavella, F.; Petrides, K.V.; Prezerakos, P. Trait Emotional Intelligence Questionnaire–Adolescent Short Form: A Psychometric Investigation in Greek Context. J. Psychoeduc. Assess. 2017, 36, 436–445. [Google Scholar] [CrossRef]
- Shapiro, S.L.; Carlson, L.E. The Art and Science of Mindfulness: Integrating Mindfulness into Psychology and the Helping Professions, 2nd ed.; American Psychological Association: Washington, DC, USA, 2017. [Google Scholar]
- Brown, D.B.; Bravo, A.J.; Roos, C.R.; Pearson, M.R. Five facets of mindfulness and psychological health: Evaluating a psychological model of the mechanisms of mindfulness. Mindfulness 2014, 6, 1021–1032. [Google Scholar] [CrossRef]
- Pepping, C.A.; Duvenage, M.; Cronin, T.J.; Lyons, A. Adolescent mindfulness and psychopathology: The role of emotion regulation. Pers. Indiv. Differ. 2016, 99, 302–307. [Google Scholar] [CrossRef]
- Keye, M.D.; Pidgeon, A.M. Investigation of the relationship between resilience, mindfulness, and academic self-efficacy. Open J. Soc. Sci. 2013, 1, 1–4. [Google Scholar] [CrossRef]
- Beutel, M.E.; Tibubos, A.N.; Klein, E.M.; Schmutzer, G.; Reiner, I.; Kocalevent, R.D.; Brähler, E. Childhood adversities and distress-The role of resilience in a representative sample. PloS ONE 2017, 12, e0173826. [Google Scholar] [CrossRef] [PubMed]
- Bluth, K.; Blanton, P.W. Mindfulness and self-compassion: Exploring pathways to adolescent emotional well-being. J. Child Fam. Stud. 2014, 23, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Pallozzi, R.; Wertheim, E.; Paxton, S.; Ong, B. Trait mindfulness measures for use with adolescents: A systematic review. Mindfulness 2017, 8, 110–125. [Google Scholar] [CrossRef]
- Tan, L.B.; Martin, G. Mind full or mindful: A report on mindfulness and psychological health in healthy adolescents. Int. J. Adolesc. Youth 2016, 211, 64–74. [Google Scholar] [CrossRef]
- Ellis, A.; David, D.; Lynn, S.J. Rational and Irrational Beliefs: A Historical and Conceptual Perspective; Rational and irrational beliefs: Research, theory, and clinical practice; David, D., Lynn, S.J., Ellis, A., Eds.; Oxford University Press: New York, NY, USA, 2010; pp. 3–22. [Google Scholar]
- Ellis, A. Reason and Emotion in Psychotherapy; Lyle Stuart: Oxford, UK, 1962. [Google Scholar]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative life events cognitive emotion regulation and emotional problems. Pers. Indiv. Differ. 2001, 30, 1311–1327. [Google Scholar] [CrossRef]
- Salvador, M.D.C.; Oliveira, S.; Matos, A.P.; Arnarson, E.; Craighead, W.E. A silent pathway to depression: Social anxiety and emotion regulation as predictors of depressive symptoms. In GAI International Academic Conferences; Handle Inc.: Praga, Czech Republic, 2015; Available online: handle/10316/83576 (accessed on 20 January 2020).
- Vîslă, A.; Flückiger, C.; Grosse Holtforth, M.; David, D. Irrational beliefs and psychological distress: a meta-analysis. Psychother. Psychosom. 2016, 85, 8–15. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M. Emotional intelligence mediates the relationship between mindfulness and subjective well-being. Pers. Indiv. Differ. 2011, 50, 1116–1119. [Google Scholar] [CrossRef]
- Wang, Y.; Kong, F. The role of emotional intelligence in the impact of mindfulness on life satisfaction and mental distress. Soc. Indic. Res. 2014, 116, 843–852. [Google Scholar] [CrossRef]
- Miao, C.; Humphrey, R.H.; Qian, S. The relationship between emotional intelligence and trait mindfulness: A meta-analytic review. Pers. Indiv. Differ. 2018, 135, 101–107. [Google Scholar] [CrossRef]
- Ortuño-Sierra, J.; Fonseca-Pedrero, E.; Aritio-Solana, R.; Velasco, A.M.; De Luis, E.C.; Schumann, G.; Cattrell, A.; Flor, H.; Nees, F.; Banaschewski, T.; et al. New evidence of factor structure and measurement invariance of the SDQ across five European nations. Eur. Child Adolesc. Psychiatry 2015, 24, 1523–1534. [Google Scholar] [CrossRef]
- Gökçen, E.; Furnham, A.; Mavroveli, S.; Petrides, K.V. A cross-cultural investigation of trait emotional intelligence in Hong Kong and the UK. Pers. Indiv. Differ. 2014, 65, 30–35. [Google Scholar] [CrossRef]
- Nozaki, Y. Cross-cultural comparison of the association between trait emotional intelligence and emotion regulation in European-American and Japanese populations. Pers. Indiv. Differ. 2018, 130, 150–155. [Google Scholar] [CrossRef]
- Potthoff, S.; Garnefski, N.; Miklósi, M.; Ubbiali, A.; Domínguez-Sánchez, F.J.; Martins, E.C.; Witthöft, M.; Kraaij, V. Cognitive emotion regulation and psychopathology across cultures: A comparison between six European countries. Pers. Indiv. Differ. 2016, 98, 218–224. [Google Scholar] [CrossRef]
- Christopher, M.S.; Charoensuk, S.; Gilbert, B.D.; Neary, T.J.; Pearce, K.L. Mindfulness in Thailand and the United States: A case of apples versus oranges? J. Clin. Psychol. 2009, 65, 590–612. [Google Scholar] [CrossRef]
- Johnson, C.J.; Wiebe, J.S.; Morera, O.F. The spanish version of the Mindful Attention Awareness Scale MAAS: Measurement invariance and psychometric properties. Mindfulness 2014, 5, 552–565. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Ortuño-Sierra, J.; Chocarro, E.; Fonseca-Pedrero, E.; Sastre i Riba, S.; Muñiz, J. The assessment of emotional and behavioural problems: Internal structure of the Strengths and Difficulties Questionnaire. Int. J. Clin. Health. Psychol. 2015, 15, 265–273. [Google Scholar] [CrossRef]
- Abreu-Lima, I.; Alarcão, M.; Almeida, A.; Brandão, T.; Cruz, O.; Gaspar, M.; Dos Santos, M.R. Avaliação de intervenções de educação parental: Relatório. 2010. Available online: http://www.cnpcjr.pt/preview_documentos.asp?r=3493m=PDF (accessed on 17 June 2019).
- Pechorro, P.; Poiares, C.; Vieira, R. Propriedades psicométricas do Questionário de Capacidades e de Dificuldades na versão portuguesa de auto-resposta. Revista de Psiquiatria Consiliar e de Ligação 2011, 16, 99–109. [Google Scholar]
- Petrides, K.V.; Sangareau, Y.; Furnham, A.; Frederickson, N. Trait emotional intelligence and children’s peer relations at school. Soc. Dev. 2006, 15, 537–547. [Google Scholar] [CrossRef]
- Ferrando, M.; Prieto, M.D.; Almeida, L.S.; Ferrándiz, C.; Bermejo, R.; López-Pina, J.A.; Hernández, D.; Sáinz, M.; Fernández, M.C. Trait emotional intelligence and academic performance: Controlling for the effects of IQ, personality, and self-concept. J. Psychoeduc. Assess. 2011, 29, 150–159. [Google Scholar] [CrossRef]
- Salvador, M.C.; Bandeira, A. O questionário de Inteligência Emocional Traço para Adolescentes—Versão Breve TEIQue-SF-A: estudo factorial e características psicométricas numa amostra de adolescentes Portugueeses. Submitted.
- Greco, L.; Baer, R.A.; Smith, G.T. Assessing mindfulness in children and adolescents: Development and validation of the child and adolescent mindfulness measure (CAMM). Psychol. Assess. 2011, 23, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Cunha, M.; Pinto-Gouveia, J.; Paiva, M.J. October. Mindfulness skills in Portuguese adolescents: Psychometric properties of the Children’s Acceptance and Mindfulness Measure CAMM. In The Meeting of the 40th Annual Congress of EABCT; European Association for Behavioral and Cognitive Therapies (EABCT): Milan, Italy, 2010. [Google Scholar]
- Cunha, M.; Paiva, M.J. Text anxiety in adolescents: The role of self-criticism and acceptance and mindfulness skills. Span. J. Psychol. 2012, 15, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Cunha, M.; Galhardo, A.; Pinto-Gouveia, J. Child and adolescent mindfulness measure CAMM: estudo das características psicométricas da versão portuguesa. Psicologia: Reflexão e Crítica 2013, 26, 459–468. [Google Scholar] [CrossRef]
- Viñas, F.; Malo, S.; González, M.; Navarro, D.; Casas, F. Assessing mindfulness on a sample of Catalan-speaking Spanish adolescents: Validation of the Catalan version of the child and adolescent mindfulness measure. Span. J. Psychol. 2015, 18, E46. [Google Scholar] [CrossRef]
- Turanzas-Romero, J. Adaptación transcultural de la escala CAMM Child and Adolescent Mindfulness Measure y estudio preliminar de sus características psicométricas. Master’s Thesis, Valencia International University, Valencia, Spain, 2013. [Google Scholar]
- Domínguez-Sánchez, F.J.; Lasa-Aristu, A.; Amor, P.J.; Holgado-Tello, F.P. Psychometric properties of the Spanish version of the Cognitive Emotion Regulation Questionnaire. Assessment 2013, 20, 253–261. [Google Scholar] [CrossRef]
- Serra, A. Regulação emocional e estilos parentais: Factores de risco ou de proteção no desenvolvimento da Perturbação Depressiva Major nos adolescentes. Master’s Thesis, Faculdade de Psicologia e de Ciências da Educação, Coimbra, Portugal, 2009. [Google Scholar]
- Mestre, J.M.; Núñez-Lozano, J.M.; Gómez-Molinero, R.; Zayas, A.; Guil, R. Emotion regulation ability and resilience in a sample of adolescents from a suburban area. Front. Psychol. 2017, 8, 1980. [Google Scholar] [CrossRef]
- Arnarson, E.Ö.; Matos, A.P.; Salvador, C.; Ribeiro, C.; De Sousa, B.; Craighead, W.E. Longitudinal study of life events, well-being, emotional regulation and depressive symptomatology. J. Psychopathol. Behav. 2016, 38, 159–171. [Google Scholar] [CrossRef]
- Duarte, A.C.; Matos, A.P.; Marques, C. Cognitive emotion regulation strategies and depressive symptoms: Gender’s moderating effect. Procd. Soc. Behv. 2015, 165, 275–283. [Google Scholar] [CrossRef]
- Diedenhofen, B.; Musch, J. Cocron: A web interface and R package for the statistical comparison of Cronbach’s alpha coefficients. Int. J. Internet Sci. 2016, 11, 51–60. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Barraca, J.; Fernández, A. Emotional Intelligence as predictor of pychosocial adaptation in the educational environment. Outcomes of an empirical research with students from the Community of Madrid. Anxiety Stress 2006, 12, 427–438. [Google Scholar]
- Piqueras, J.A.; Mateu, O.; Cejudo, J.; Perez-Gonzalez, J.C. Pathways into psychosocial adjustment in children: modeling the effects of trait emotional intelligence, social-emotional problems, and gender. Front. Psychol. 2019, 10, 507. [Google Scholar] [CrossRef] [PubMed]
- Mavroveli, S.; Petrides, K.V.; Shove, C.; Whitehead, A. Investigation of the construct of trait emotional intelligence in children. Eur. Child Adolesc. Psychiatry 2008, 17, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Eastabrook, J.M.; Flynn, J.J.; Hollenstein, T. Internalizing symptoms in female adolescents: Associations with emotional awareness and emotion regulation. J. Child Fami. Stud. 2014, 23, 487–496. [Google Scholar] [CrossRef]
- Lahaye, M.; Van Broeck, N.; Bodart, E.; Luminet, O. Predicting quality of life in pediatric asthma: the role of emotional competence and personality. Qual. Life Res. 2013, 22, 907–916. [Google Scholar] [CrossRef]
- Rowsell, H.C.; Ciarrochi, J.; Heaven, P.C.; Deane, F.P. The role of emotion identification skill in the formation of male and female friendships: A longitudinal study. J. Adolesc. 2014, 37, 103–111. [Google Scholar] [CrossRef]
- Goldner, L.; Scharf, M. Attachment security, personality, and adjustment of elementary school children. J. Genet. Psychol. 2013, 174, 473–493. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Spain | Portugal | Total Sample | Cronbach’s Alpha | Number of Items |
|---|---|---|---|---|---|
| SDQ | 0.67 | 0.63 | 0.64 | 0.16 | 25 |
| TeiQue-ASF | 0.85 | 0.85 | 0.86 | 0.56 | 30 |
| CAMM | 0.85 | 0.76 | 0.82 | 0.0001 | 10 |
| CERQ-Catastrophizing | 0.73 | 0.78 | 0.75 | 0.04 | 4 |
| Variable | Spain | Portugal | t (1368) | d |
|---|---|---|---|---|
| SDQ | 11.44 (5.20) | 12.15 (4.74) | −2.61 ** | −0.14 |
| TeiQue-ASF | 146.06 (22.65) | 136.42 (21.09) | 8.12 *** | 0.44 |
| CAMM | 25.69 (7.24) | 21.88 (5.77) | 10.85 *** | 0.59 |
| CERQ-Catastrophizing | 9.39 (3.71) | 9.28 (3.55) | 0.57 ns | - |
| Variables | Mean | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| (1) Trait EI | 140.58 | 22.29 | - | |||
| (2) Mindfulness skills | 23.52 | 6.72 | 0.51 ** | - | ||
| (3) Catastrophizing | 9.32 | 3.62 | −0.38 ** | −0.35 ** | - | |
| (4) Psychological problems | 11.84 | 4.96 | −0.62 ** | −0.48 ** | 0.38 ** | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piqueras, J.A.; Salvador, M.d.C.; Soto-Sanz, V.; Mira, F.; Pérez-González, J.-C. Strengths Against Psychopathology in Adolescents: Ratifying the Robust Buffer Role of Trait Emotional Intelligence. Int. J. Environ. Res. Public Health 2020, 17, 804. https://doi.org/10.3390/ijerph17030804
Piqueras JA, Salvador MdC, Soto-Sanz V, Mira F, Pérez-González J-C. Strengths Against Psychopathology in Adolescents: Ratifying the Robust Buffer Role of Trait Emotional Intelligence. International Journal of Environmental Research and Public Health. 2020; 17(3):804. https://doi.org/10.3390/ijerph17030804
Chicago/Turabian StylePiqueras, José A., Maria do Céu Salvador, Victoria Soto-Sanz, Francisco Mira, and Juan-Carlos Pérez-González. 2020. "Strengths Against Psychopathology in Adolescents: Ratifying the Robust Buffer Role of Trait Emotional Intelligence" International Journal of Environmental Research and Public Health 17, no. 3: 804. https://doi.org/10.3390/ijerph17030804
APA StylePiqueras, J. A., Salvador, M. d. C., Soto-Sanz, V., Mira, F., & Pérez-González, J.-C. (2020). Strengths Against Psychopathology in Adolescents: Ratifying the Robust Buffer Role of Trait Emotional Intelligence. International Journal of Environmental Research and Public Health, 17(3), 804. https://doi.org/10.3390/ijerph17030804