Maternal Exposure to Disinfection By-Products and Risk of Hypospadias in the National Birth Defects Prevention Study (2000–2005)


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
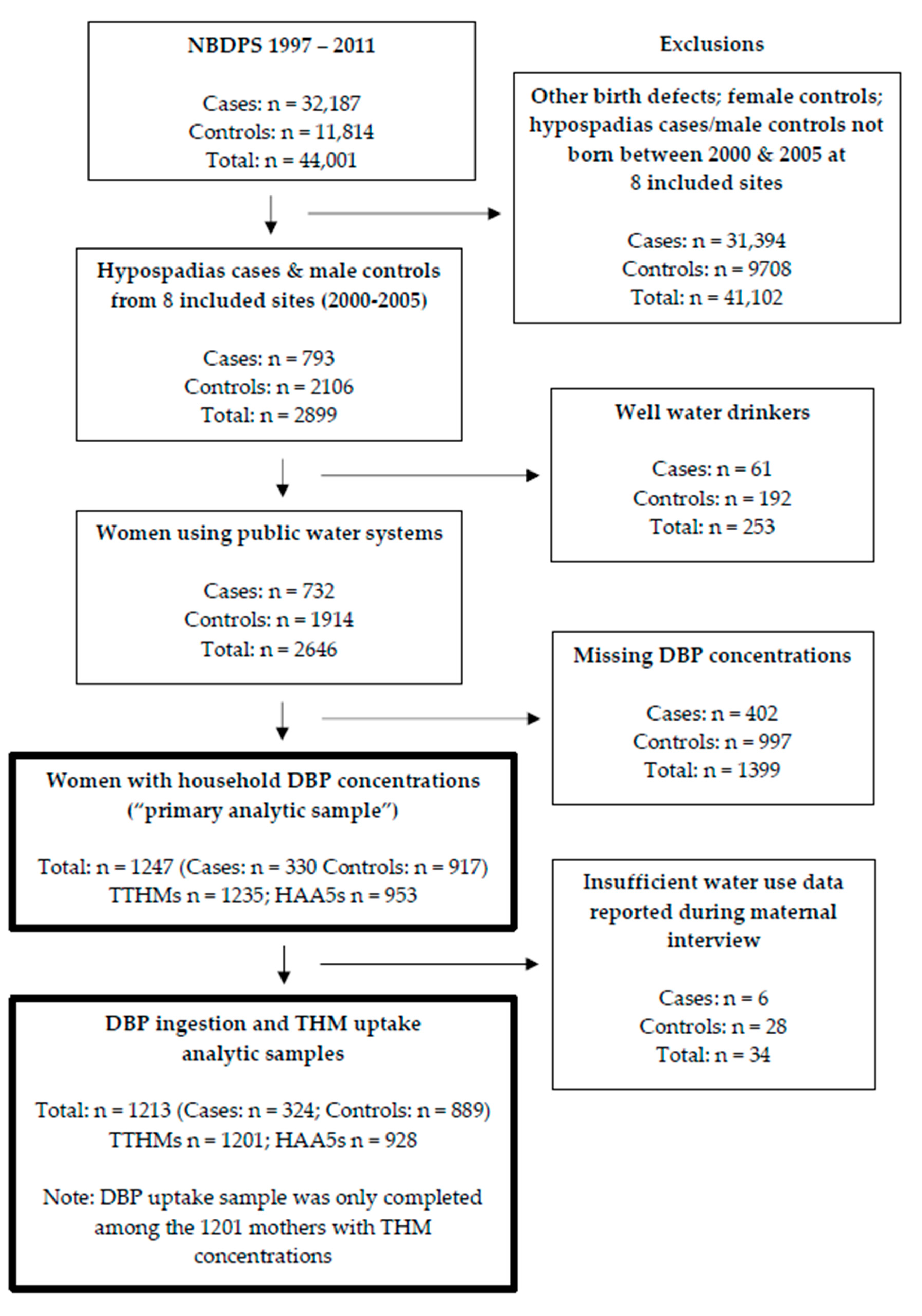
2.1. Study Design and Study Population
2.2. Outcome Classification
2.3. Exposure Classifications
2.3.1. Overview
2.3.2. DBP Concentrations in Household Tap Water
2.3.3. Water Consumption and DBP Ingestion
2.3.4. Uptake of THMs via Ingestion, Showering, and Bathing
2.4. Analysis
3. Results
3.1. Household Tap Water Concentrations and Hypospadias
3.2. DBP Ingestion and Hypospadias
3.3. Uptake of THMs via Ingestion, Showering, and Bathing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mai, C.T.; Isenburg, J.; Langlois, P.H.; Alverson, C.J.; Gilboa, S.M.; Rickard, R.; Canfield, M.A.; Anjohrin, S.B.; Lupo, P.J.; Jackson, D.R.; et al. Population-based birth defects data in the United States, 2008 to 2012: Presentation of state-specific data and descriptive brief on variability of prevalence. Birth Defects Res. A Clin. Mol. Teratol. 2015, 103, 972–993. [Google Scholar] [CrossRef] [PubMed]
- Fredell, L.; Kockum, I.; Hansson, E.; Holmner, S.; Lundquist, L.; Lackgren, G.; Pedersen, J.; Stenberg, A.; Westbacke, G.; Nordenskjold, A. Heredity of hypospadias and the significance of low birth weight. J. Urol. 2002, 167, 1423–1427. [Google Scholar] [CrossRef]
- Carmichael, S.L.; Shaw, G.M.; Lammer, E.J. Environmental and genetic contributors to hypospadias: A review of the epidemiologic evidence. Birth Defects Res. A Clin. Mol. Teratol. 2012, 94, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Bouty, A.; Ayers, K.L.; Pask, A.; Heloury, Y.; Sinclair, A.H. The Genetic and Environmental Factors Underlying Hypospadias. Sex. Dev. 2015, 9, 239–259. [Google Scholar] [CrossRef] [PubMed]
- Shih, E.M.; Graham, J.M., Jr. Review of genetic and environmental factors leading to hypospadias. Eur. J. Med. Genet. 2014, 57, 453–463. [Google Scholar] [CrossRef]
- Akre, O.; Boyd, H.A.; Ahlgren, M.; Wilbrand, K.; Westergaard, T.; Hjalgrim, H.; Nordenskjold, A.; Ekbom, A.; Melbye, M. Maternal and gestational risk factors for hypospadias. Environ. Health Perspect. 2008, 116, 1071–1076. [Google Scholar] [CrossRef]
- USEPA. Comprehensive Disinfectants and Disinfection Byproducts Rules (Stage 1 and Stage 2): Quick Reference Guide; USEPA: Washington, DC, USA, 2010.
- Bielmeier, S.R.; Best, D.S.; Guidici, D.L.; Narotsky, M.G. Pregnancy loss in the rat caused by bromodichloromethane. Toxicol. Sci. 2001, 59, 309–315. [Google Scholar] [CrossRef]
- Narotsky, M.G.; Best, D.S.; McDonald, A.; Godin, E.A.; Hunter, E.S., 3rd; Simmons, J.E. Pregnancy loss and eye malformations in offspring of F344 rats following gestational exposure to mixtures of regulated trihalomethanes and haloacetic acids. Reprod. Toxicol. 2011, 31, 59–65. [Google Scholar] [CrossRef]
- Murray, F.; Schwetz, B.; McBride, J.; Staples, R. Toxicity of inhaled chloroform in pregnant mice and their offspring. Toxicol. Appl. Pharmacol. 1979, 50, 515–522. [Google Scholar] [CrossRef]
- Wright, J.M.; Schwartz, J.; Dockery, D.W. Effect of trihalomethane exposure on fetal development. Occup. Environ. Med. 2003, 60, 173–180. [Google Scholar] [CrossRef]
- Savitz, D.A.; Singer, P.C.; Herring, A.H.; Hartmann, K.E.; Weinberg, H.S.; Makarushka, C. Exposure to drinking water disinfection by-products and pregnancy loss. Am. J. Epidemiol. 2006, 164, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, C.S.; Mendola, P.; Savitz, D.A.; Herring, A.H.; Loomis, D.; Hartmann, K.E.; Singer, P.C.; Weinberg, H.S.; Olshan, A.F. Drinking water disinfection by-product exposure and duration of gestation. Epidemiology 2008, 19, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Klotz, J.B.; Pyrch, L.A. Neural tube defects and drinking water disinfection by-products. Epidemiology 1999, 10, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Gonsioroski, A.; Mourikes, V.E.; Flaws, J.A. Endocrine Disruptors in Water and Their Effects on the Reproductive System. Int. J. Mol. Sci. 2020, 21, 1929. [Google Scholar] [CrossRef] [PubMed]
- Melnick, R.L.; Nyska, A.; Foster, P.M.; Roycroft, J.H.; Kissling, G.E. Toxicity and carcinogenicity of the water disinfection byproduct, dibromoacetic acid, in rats and mice. Toxicology 2007, 230, 126–136. [Google Scholar] [CrossRef]
- Jiang, J.; Ma, L.; Yuan, L.; Wang, X.; Zhang, W. Study on developmental abnormalities in hypospadiac male rats induced by maternal exposure to di-n-butyl phthalate (DBP). Toxicology 2007, 232, 286–293. [Google Scholar] [CrossRef]
- Foster, P.M.; Harris, M.W. Changes in androgen-mediated reproductive development in male rat offspring following exposure to a single oral dose of flutamide at different gestational ages. Toxicol. Sci. 2005, 85, 1024–1032. [Google Scholar] [CrossRef]
- Kim, K.S.; Torres, C.R., Jr.; Yucel, S.; Raimondo, K.; Cunha, G.R.; Baskin, L.S. Induction of hypospadias in a murine model by maternal exposure to synthetic estrogens. Environ. Res. 2004, 94, 267–275. [Google Scholar] [CrossRef]
- Hwang, B.-F.; Jaakkola, J.J.; Guo, H.-R. Water disinfection by-products and the risk of specific birth defects: A population-based cross-sectional study in Taiwan. Environ. Health 2008, 7, 23. [Google Scholar] [CrossRef]
- Iszatt, N.; Nieuwenhuijsen, M.J.; Nelson, P.; Elliott, P.; Toledano, M.B. Water consumption and use, trihalomethane exposure, and the risk of hypospadias. Pediatrics 2011, 127, e389–e397. [Google Scholar] [CrossRef]
- Luben, T.J.; Nuckols, J.R.; Mosley, B.S.; Hobbs, C.; Reif, J.S. Maternal exposure to water disinfection by-products during gestation and risk of hypospadias. Occup. Environ. Med. 2008, 65, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Reefhuis, J.; Gilboa, S.M.; Anderka, M.; Browne, M.L.; Feldkamp, M.L.; Hobbs, C.A.; Jenkins, M.M.; Langlois, P.H.; Newsome, K.B.; Olshan, A.F.; et al. The National Birth Defects Prevention Study: A review of the methods. Birth Defects Res. A Clin. Mol. Teratol. 2015, 103, 656–669. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, M.E.; Bitsko, R.H.; Anderka, M.; Caton, A.R.; Feldkamp, M.L.; Hockett Sherlock, S.M.; Meyer, R.E.; Ramadhani, T.; Robbins, J.M.; Shaw, G.M.; et al. Control selection and participation in an ongoing, population-based, case-control study of birth defects: The National Birth Defects Prevention Study. Am. J. Epidemiol. 2009, 170, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Weyer, P.; Rhoads, A.; Suhl, J.; Luben, T.J.; Conway, K.M.; Langlois, P.H.; Shen, D.; Liang, D.; Puzhankara, S.; Anderka, M.; et al. Drinking water disinfection byproducts and risk of orofacial clefts in the National Birth Defects Prevention Study. Birth Defects Res. 2018, 110, 1027–1042. [Google Scholar] [CrossRef]
- Rocheleau, C.M.; Romitti, P.A.; Sanderson, W.T.; Sun, L.; Lawson, C.C.; Waters, M.A.; Stewart, P.A.; Olney, R.S.; Reefhuis, J. Maternal occupational pesticide exposure and risk of hypospadias in the National Birth Defects Prevention Study. Birth Defects Res. A Clin. Mol. Teratol. 2011, 91, 927–936. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Botta, S.; Cunha, G.R.; Baskin, L.S. Do endocrine disruptors cause hypospadias? Transl. Androl. Urol. 2014, 3, 330. [Google Scholar]
- Baskin, L.S.; Himes, K.; Colborn, T. Hypospadias and endocrine disruption: Is there a connection? Environ. Health Perspect. 2001, 109, 1175–1183. [Google Scholar] [CrossRef]
- Blaschko, S.D.; Cunha, G.R.; Baskin, L.S. Molecular mechanisms of external genitalia development. Differentiation 2012, 84, 261–268. [Google Scholar] [CrossRef]
- Ma, L. Battle of sex hormones in genitalia anomalies. Proc. Natl. Acad. Sci. USA 2015, 112, 15779–15780. [Google Scholar] [CrossRef]
- Hyun, G.; Kolon, T.F. Endocrine evaluation of hypospadias. Adv. Exp. Med. Biol. 2004, 545, 31–43. [Google Scholar] [CrossRef]
- Holmes, B.E.; Smeester, L.; Fry, R.C.; Weinberg, H.S. Identification of endocrine active disinfection by-products (DBPs) that bind to the androgen receptor. Chemosphere 2017, 187, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Holmes, B.E.; Smeester, L.; Fry, R.C.; Weinberg, H.S. Disinfection Byproducts Bind Human Estrogen Receptor-alpha. Environ. Toxicol. Chem. 2019, 38, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Rocheleau, C.M.; Romitti, P.A.; Dennis, L.K. Pesticides and hypospadias: A meta-analysis. J. Pediatr. Urol. 2009, 5, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, S.L.; Yang, W.; Roberts, E.M.; Kegley, S.E.; Wolff, C.; Guo, L.; Lammer, E.J.; English, P.; Shaw, G.M. Hypospadias and residential proximity to pesticide applications. Pediatrics 2013, 132, e1216–e1226. [Google Scholar] [CrossRef]
- Rodriguez, M.J.; Serodes, J.B. Spatial and temporal evolution of trihalomethanes in three water distribution systems. Water Res. 2001, 35, 1572–1586. [Google Scholar] [CrossRef]
- Wright, J.M.; Bateson, T.F. A sensitivity analysis of bias in relative risk estimates due to disinfection by-product exposure misclassification. J. Expo. Anal. Environ. Epidemiol. 2005, 15, 212–216. [Google Scholar] [CrossRef]
- Parvez, S.; Frost, K.; Sundararajan, M. Evaluation of Drinking Water Disinfectant Byproducts Compliance Data as an Indirect Measure for Short-Term Exposure in Humans. Int. J. Environ. Res. Public Health 2017, 14, 548. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Toledano, M.B.; Elliott, P. Uptake of chlorination disinfection by-products; a review and a discussion of its implications for exposure assessment in epidemiological studies. J. Expo. Anal Environ. Epidemiol. 2000, 10, 586–599. [Google Scholar] [CrossRef]
- Wright, J.M.; Evans, A.; Kaufman, J.A.; Rivera-Nunez, Z.; Narotsky, M.G. Disinfection By-Product Exposures and the Risk of Specific Cardiac Birth Defects. Environ. Health Perspect. 2017, 125, 269–277. [Google Scholar] [CrossRef]
- Kaufman, J.A.; Wright, J.M.; Evans, A.; Rivera-Núñez, Z.; Meyer, A.; Narotsky, M.G. Associations between disinfection by-product exposures and craniofacial birth defects. J. Occup. Environ. Med. 2018, 60, 109. [Google Scholar] [CrossRef]
- Sparks, P.J. Rural-urban differences in breastfeeding initiation in the United States. J. Hum. Lact. 2010, 26, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Ayotte, J.D.; Medalie, L.; Qi, S.L.; Backer, L.C.; Nolan, B.T. Estimating the high-arsenic domestic-well population in the conterminous United States. Environ. Sci. Technol. 2017, 51, 12443–12454. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.H.; Jones, R.R.; Brender, J.D.; de Kok, T.M.; Weyer, P.J.; Nolan, B.T.; Villanueva, C.M.; van Breda, S.G. Drinking Water Nitrate and Human Health: An Updated Review. Int. J. Environ. Res. Public Health 2018, 15, 1557. [Google Scholar] [CrossRef] [PubMed]
- Backer, L.C.; Ashley, D.L.; Bonin, M.A.; Cardinali, F.L.; Kieszak, S.M.; Wooten, J.V. Household exposures to drinking water disinfection by-products: Whole blood trihalomethane levels. J. Expo. Anal. Environ. Epidemiol. 2000, 10, 321–326. [Google Scholar] [CrossRef]


{kind=link}
| Maternal Characteristic | Cases α | Controls | ||
|---|---|---|---|---|
| n | % | n | % | |
| Maternal age at conception | ||||
| <20 years | 26 | 7.9 | 110 | 12.0 |
| 20–25 years | 81 | 24.6 | 264 | 28.8 |
| 26–35 years | 182 | 55.2 | 468 | 51.0 |
| 36+ years | 41 | 12.4 | 75 | 8.2 |
| Maternal race/ethnicity | ||||
| Non-Hispanic White | 236 | 71.5 | 540 | 58.9 |
| Non-Hispanic Black | 49 | 14.9 | 136 | 14.8 |
| Hispanic | 20 | 6.1 | 175 | 19.1 |
| Other | 25 | 7.6 | 66 | 7.2 |
| Pre-pregnancy body mass index * | ||||
| Underweight | 19 | 5.9 | 40 | 4.6 |
| Normal weight | 160 | 49.5 | 462 | 52.6 |
| Overweight | 86 | 26.6 | 210 | 23.9 |
| Obese | 58 | 18.0 | 166 | 18.9 |
| Missing | 7 | 39 | ||
| Maternal education | ||||
| <High school | 25 | 7.6 | 145 | 15.8 |
| High school | 53 | 16.1 | 219 | 23.9 |
| >High school | 252 | 76.4 | 552 | 60.3 |
| Missing | 0 | 1 | ||
| Number of previous livebirths | ||||
| 0 | 181 | 54.9 | 385 | 42.0 |
| 1 | 97 | 29.4 | 290 | 31.6 |
| ≥2 | 52 | 15.8 | 242 | 26.4 |
| Family history of hypospadias (1 degree relative) | ||||
| No | 319 | 96.7 | 913 | 99.6 |
| Yes | 11 | 3.3 | 4 | 0.4 |
| Study Site | ||||
| Arkansas | 62 | 18.8 | 157 | 17.1 |
| Georgia | 64 | 19.4 | 164 | 17.9 |
| Iowa | 28 | 8.5 | 142 | 15.5 |
| Massachusetts | 97 | 29.4 | 128 | 14.0 |
| New York | 5 | 1.5 | 27 | 2.9 |
| North Carolina | 46 | 13.9 | 128 | 14.0 |
| Texas | 6 | 1.8 | 127 | 13.9 |
| Utah | 22 | 6.7 | 44 | 4.8 |
| DBP | Quantile | μg/L | Total | Cases | Controls | OR | 95% CI | aOR φ | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| TTHM | 1235 | ||||||||
| Q1 (<50%) | <37.2 | 162 (50.0) | 455 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥37.2–<52.9 | 89 (27.5) | 228 (25.0) | 1.1 | 0.8, 1.5 | 1.1 | 0.8, 1.5 | ||
| Q3 (≥75%) | ≥52.9 | 73 (22.5) | 228 (25.0) | 0.9 | 0.7, 1.2 | 0.8 | 0.5, 1.1 | ||
| BRF | 869 | ||||||||
| Q1 (<50%) | <0.5 | 121 (63.4) | 339 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥0.5–<3.1 | 52 (27.2) | 169 (24.9) | 0.9 | 0.6, 1.3 | 0.6 | 0.3, 1.2 | ||
| Q3 (≥75%) | ≥3.1 | 18 (9.4) | 170 (25.1) | 0.3 | 0.2, 0.5 | 0.3 | 0.1, 0.8 | ||
| CHLF | 869 | ||||||||
| Q1 (<50%) | <19.7 | 66 (34.6) | 339 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥19.7–<35.0 | 64 (33.5) | 168 (24.8) | 2.0 | 1.3, 2.9 | 1.2 | 0.8, 1.9 | ||
| Q3 (≥75%) | ≥35.0 | 61 (31.9) | 171 (25.2) | 1.8 | 1.2, 2.7 | 1.1 | 0.7, 1.8 | ||
| BDCM | 868 | ||||||||
| Q1 (<50%) | <7.0 | 82 (42.9) | 338 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥7.0–<11.0 | 72 (37.7) | 167 (24.7) | 1.8 | 1.2, 2.6 | 1.8 | 1.2, 2.7 | ||
| Q3 (≥75%) | ≥11.0 | 37 (19.4) | 172 (25.4) | 0.9 | 0.6, 1.4 | 0.7 | 0.4, 1.1 | ||
| DBCM | 867 | ||||||||
| Q1 (<50%) | <2.5 | 127 (66.8) | 335 (49.5) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥2.5–<7.0 | 44 (23.2) | 173 (25.6) | 0.7 | 0.5, 1.0 | 0.8 | 0.5, 1.3 | ||
| Q3 (≥75%) | ≥7.0 | 19 (10.0) | 169 (25.0) | 0.3 | 0.2, 0.5 | 0.5 | 0.3, 0.9 | ||
| HAA5 | 953 | ||||||||
| Q1 (<50%) | <24.5 | 148 (53.8) | 335 (49.4) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥24.5–<37.4 | 61 (22.2) | 173 (25.5) | 0.8 | 0.6, 1.1 | 0.8 | 0.6, 1.2 | ||
| Q3 (≥75%) | ≥37.4 | 66 (24.0) | 170 (25.1) | 0.9 | 0.6, 1.2 | 0.8 | 0.6, 1.2 | ||
| MBAA | 759 | ||||||||
| Q1 (No exposure) α | 0 | 112 (58.0) | 325 (57.4) | 1.0 | REF | 1.0 | REF | ||
| Q2 (<75%) | >0–<1.0 | 16 (8.3) | 38 (6.8) | 1.2 | 0.7, 2.3 | 1.5 | 0.7, 3.0 | ||
| Q3 (≥75%) | ≥1.0 | 65 (33.7) | 203 (35.9) | 0.9 | 0.7, 1.3 | 0.8 | 0.5, 1.4 | ||
| MCAA | 759 | ||||||||
| Q1 (<50%) | <1.3 | 103 (53.4) | 283 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥1.3–<3.5 | 48 (24.9) | 141 (24.9) | 0.9 | 0.6, 1.4 | 0.7 | 0.4, 1.3 | ||
| Q3 (≥ 75%) | ≥ 3.5 | 42 (21.8) | 142 (25.1) | 0.8 | 0.5, 1.2 | 0.6 | 0.4, 1.2 | ||
| DBAA | 759 | ||||||||
| Q1 (<50%) | <0.9 | 113 (58.6) | 283 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥0.9–<2.1 | 55 (28.5) | 141 (24.9) | 1.0 | 0.7, 1.4 | 1.0 | 0.6, 1.6 | ||
| Q3 (≥75%) | ≥2.1 | 25 (13.0) | 142 (25.1) | 0.4 | 0.3, 0.7 | 0.6 | 0.3, 1.1 | ||
| DCAA | 759 | ||||||||
| Q1 (<50%) | <12.4 | 91 (47.15) | 283 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥12.4–<19.9 | 50 (25.9) | 141 (24.9) | 1.1 | 0.7, 1.6 | 0.8 | 0.5, 1.3 | ||
| Q3 (≥75%) | ≥ 19.9 | 52 (26.9) | 142 (25.1) | 1.1 | 0.8, 1.7 | 0.8 | 0.5, 1.3 | ||
| TCAA | 759 | ||||||||
| Q1 (<50%) | <9.4 | 88 (45.6) | 285 (50.4) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥9.4–<15.8 | 46 (23.8) | 139 (24.6) | 1.1 | 0.7, 1.6 | 0.8 | 0.5, 1.3 | ||
| Q3 (≥75%) | ≥15.8 | 59 (30.6) | 142 (25.1) | 1.3 | 0.9, 2.0 | 1.0 | 0.6, 1.5 |
| Regulation Categorizations | Cases | Controls | OR | 95% CI | aOR * | 95% CI |
|---|---|---|---|---|---|---|
| Total Trihalomethanes (TTHMs) ≤ 80 μg/L | 300 (92.6) | 834 (91.6) | 1.0 | REF | 1.0 | REF |
| TTHMs > 80 μg/L | 24 (7.4) | 77 (8.5) | 0.9 | 0.5, 1.4 | 0.7 | 0.4, 1.1 |
| Total | 324 | 911 | ||||
| Total Haloacetic Acids (HAA5s) ≤ 60 μg/L | 257 (93.5) | 623 (91.9) | 1.0 | REF | 1.0 | REF |
| HAA5s > 60 μg/L | 18 (6.6) | 55 (8.1) | 0.8 | 0.5, 1.4 | 0.8 | 0.4, 1.4 |
| Total | 275 | 678 |
| DBP | Quantile | μg/Day | Total | Cases | Controls | OR | 95% CI | aOR φ | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| TTHM | 1201 | ||||||||
| Q1 (<50%) | <16.3 | 163 (51.3) | 442 (50.1) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<5%) | ≥16.3–<49.6 | 85 (26.7) | 222 (25.1) | 1.0 | 0.8, 1.4 | 1.0 | 0.7, 1.4 | ||
| Q3 (≥75%) | ≥49.6 | 70 (22.0) | 219 (24.8) | 0.9 | 0.6, 1.2 | 0.8 | 0.5, 1.1 | ||
| BRF | 842 | ||||||||
| Q1 (No exposure) α | 0 | 127 (67.9) | 393 (60.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (<75%) | >0–<1.2 | 25 (13.4) | 99 (15.1) | 0.8 | 0.5, 1.3 | 0.6 | 0.4, 1.2 | ||
| Q3 (≥75%) | ≥1.2 | 35 (18.7) | 163 (24.9) | 0.7 | 0.4, 1.0 | 0.7 | 0.4, 1.2 | ||
| CHLF | 842 | ||||||||
| Q1 (<50%) | <7.5 | 76 (40.6) | 327 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥7.5–<28.5 | 58 (31.0) | 164 (25.0) | 1.5 | 1.0, 2.2 | 1.0 | 0.6, 1.5 | ||
| Q3 (≥75%) | ≥28.5 | 53 (28.3) | 164 (25.0) | 1.4 | 0.9, 2.1 | 0.8 | 0.5, 1.3 | ||
| BDCM | 841 | ||||||||
| Q1 (<50%) | <3.6 | 88 (47.1) | 327 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥3.6–<10.7 | 52 (27.8) | 163 (24.9) | 1.2 | 0.8, 1.8 | 0.9 | 0.6, 1.5 | ||
| Q3 (≥75%) | ≥10.7 | 47 (25.1) | 164 (25.1) | 1.1 | 0.7, 1.6 | 0.9 | 0.6, 1.4 | ||
| DBCM | 840 | ||||||||
| Q1 (<50%) | <1.1 | 109 (58.6) | 327 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥1.1–<4.1 | 45 (24.2) | 164 (25.1) | 0.8 | 0.6, 1.2 | 0.7 | 0.4, 1.0 | ||
| Q3 (≥75%) | ≥4.1 | 32 (17.2) | 163 (24.9) | 0.6 | 0.4, 0.9 | 0.7 | 0.4, 1.1 | ||
| HAA5 | 928 | ||||||||
| Q1 (<50%) | <11.5 | 151 (55.7) | 328 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥ 50%–<75%) | ≥11.5–<33.7 | 66 (24.4) | 164 (25.0) | 0.9 | 0.6, 1.2 | 0.9 | 0.6, 1.3 | ||
| Q3 (≥75%) | ≥33.7 | 54 (19.9) | 165 (25.1) | 0.7 | 0.5, 1.0 | 0.7 | 0.5, 1.1 | ||
| MBAA | 736 | ||||||||
| Q1 (No exposure) α | 0 | 134 (70.5) | 360 (65.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (<75%) | >0–<0.7 | 16 (8.4) | 50 (9.2) | 0.9 | 0.5, 1.6 | 0.7 | 0.4, 1.4 | ||
| Q3 (≥75%) | ≥0.7 | 40 (21.1) | 136 (24.9) | 0.8 | 0.5, 1.2 | 0.7 | 0.4, 1.1 | ||
| MCAA | 736 | ||||||||
| Q1 (No exposure) α | 0 | 116 (61.1) | 298 (54.6) | 1.0 | REF | 1.0 | REF | ||
| Q2 (<75%) | >0–<2.5 | 29 (15.3) | 112 (20.5) | 0.7 | 0.4, 1.1 | 0.5 | 0.3, 0.9 | ||
| Q3 (≥75%) | ≥2.5 | 45 (23.7) | 136 (24.9) | 0.9 | 0.6, 1.3 | 0.6 | 0.4, 1.0 | ||
| DBAA | 736 | ||||||||
| Q1 (No exposure) α | 0 | 123 (64.7) | 326 (59.7) | 1.0 | REF | 1.0 | REF | ||
| Q2 (<75%) | >0–<1.2 | 26 (13.7) | 83 (15.2) | 0.8 | 0.5, 1.4 | 0.7 | 0.4, 1.2 | ||
| Q3 (≥75%) | ≥1.2 | 41 (21.6) | 137 (25.1) | 0.8 | 0.5, 1.2 | 0.8 | 0.5, 1.3 | ||
| DCAA | 736 | ||||||||
| Q1 (<50%) | <6.5 | 90 (47.4) | 273 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥6.5–<17.8 | 57 (30.0) | 136 (24.9) | 1.3 | 0.9, 1.9 | 1.0 | 0.6, 1.5 | ||
| Q3 (≥75%) | ≥17.8 | 43 (22.6) | 137 (25.1) | 1.0 | 0.6, 1.4 | 0.7 | 0.5, 1.2 | ||
| TCAA | 736 | ||||||||
| Q1 (<50%) | <3.6 | 92 (48.4) | 273 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥3.6–<13.8 | 52 (27.4) | 137 (25.1) | 1.1 | 0.8, 1.7 | 0.8 | 0.5, 1.3 | ||
| Q3 (≥75%) | ≥13.8 | 46 (24.2) | 136 (24.9) | 1.0 | 0.7, 1.5 | 0.7 | 0.5, 1.2 |
| DBP | Quantile | μg/Day | Total | Cases | Controls | OR | 95% CI | aOR φ | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| TTHM | 1201 | ||||||||
| Q1 (<50%) | <2.60 | 175 (55.0) | 441 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥2.60–<4.60 | 81 (25.5) | 221 (25.0) | 0.9 | 0.7,1.3 | 1.0 | 0.7, 1.4 | ||
| Q3 (≥75%) | ≥4.60 | 62 (19.5) | 221 (25.0) | 0.7 | 0.5, 1.0 | 0.7 | 0.5, 1.0 | ||
| BRF | 842 | ||||||||
| Q1 (<50%) | <0.04 | 116 (62.0) | 327 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥0.04–<0.26 | 51 (27.3) | 164 (25.0) | 0.9 | 0.6, 1.3 | 0.8 | 0.4, 1.5 | ||
| Q3 (≥75%) | ≥0.26 | 20 (10.7) | 164 (25.0) | 0.3 | 0.2, 0.6 | 0.5 | 0.2, 1.1 | ||
| CHLF | 842 | ||||||||
| Q1 (<50%) | <1.43 | 78 (41.7) | 327 (49.9) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥1.43–<2.99 | 51 (27.3) | 164 (25.0) | 1.3 | 0.9, 1.9 | 0.7 | 0.5, 1.2 | ||
| Q3 (≥75%) | ≥2.99 | 58 (31.0) | 164 (25.0) | 1.5 | 1.0, 2.2 | 0.8 | 0.5, 1.3 | ||
| BDCM | 841 | ||||||||
| Q1 (<50%) | <0.54 | 89 (47.6) | 327 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥0.54–<1.00 | 60 (32.1) | 163 (24.9) | 1.4 | 0.9, 2.0 | 1.3 | 0.8, 1.9 | ||
| Q3 (≥75%) | ≥1.00 | 38 (20.3) | 164 (25.1) | 0.9 | 0.6, 1.3 | 0.7 | 0.5, 1.2 | ||
| DBCM | 840 | ||||||||
| Q1 (<50%) | <0.33 | 107 (57.5) | 327 (50.0) | 1.0 | REF | 1.0 | REF | ||
| Q2 (≥50%–<75%) | ≥0.33–<0.70 | 43 (23.1) | 163 (24.9) | 0.8 | 0.5, 1.2 | 1.0 | 0.7, 1.6 | ||
| Q3 (≥75%) | ≥0.70 | 36 (19.4) | 164 (25.1) | 0.7 | 0.4, 1.0 | 0.9 | 0.6, 1.5 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaganjor, I.; Luben, T.J.; Desrosiers, T.A.; Keil, A.P.; Engel, L.S.; Michalski, A.M.; Carmichael, S.L.; Nembhard, W.N.; Shaw, G.M.; Reefhuis, J.; et al. Maternal Exposure to Disinfection By-Products and Risk of Hypospadias in the National Birth Defects Prevention Study (2000–2005). Int. J. Environ. Res. Public Health 2020, 17, 9564. https://doi.org/10.3390/ijerph17249564
Zaganjor I, Luben TJ, Desrosiers TA, Keil AP, Engel LS, Michalski AM, Carmichael SL, Nembhard WN, Shaw GM, Reefhuis J, et al. Maternal Exposure to Disinfection By-Products and Risk of Hypospadias in the National Birth Defects Prevention Study (2000–2005). International Journal of Environmental Research and Public Health. 2020; 17(24):9564. https://doi.org/10.3390/ijerph17249564
Chicago/Turabian StyleZaganjor, Ibrahim, Thomas J. Luben, Tania A. Desrosiers, Alexander P. Keil, Lawrence S. Engel, Adrian M. Michalski, Suzan L. Carmichael, Wendy N. Nembhard, Gary M. Shaw, Jennita Reefhuis, and et al. 2020. "Maternal Exposure to Disinfection By-Products and Risk of Hypospadias in the National Birth Defects Prevention Study (2000–2005)" International Journal of Environmental Research and Public Health 17, no. 24: 9564. https://doi.org/10.3390/ijerph17249564
APA StyleZaganjor, I., Luben, T. J., Desrosiers, T. A., Keil, A. P., Engel, L. S., Michalski, A. M., Carmichael, S. L., Nembhard, W. N., Shaw, G. M., Reefhuis, J., Yazdy, M. M., Langlois, P. H., Feldkamp, M. L., Romitti, P. A., Olshan, A. F., & The National Birth Defects Prevention Study. (2020). Maternal Exposure to Disinfection By-Products and Risk of Hypospadias in the National Birth Defects Prevention Study (2000–2005). International Journal of Environmental Research and Public Health, 17(24), 9564. https://doi.org/10.3390/ijerph17249564