The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review

 , , ,
, , ,
Abstract
1. Background
2. Chronic Kidney Disease of Unknown Etiology (CKDu)
3. Etiology of CKDu
3.1. Heat Stress and CKDu
3.2. Environmental Contaminants, Water Quality, and CKDu
3.3. Infectious Origin
4. Renal Biomarkers
5. Current Use of Novel Biomarkers in CKDu Hotspots and Their Diagnostic Potential
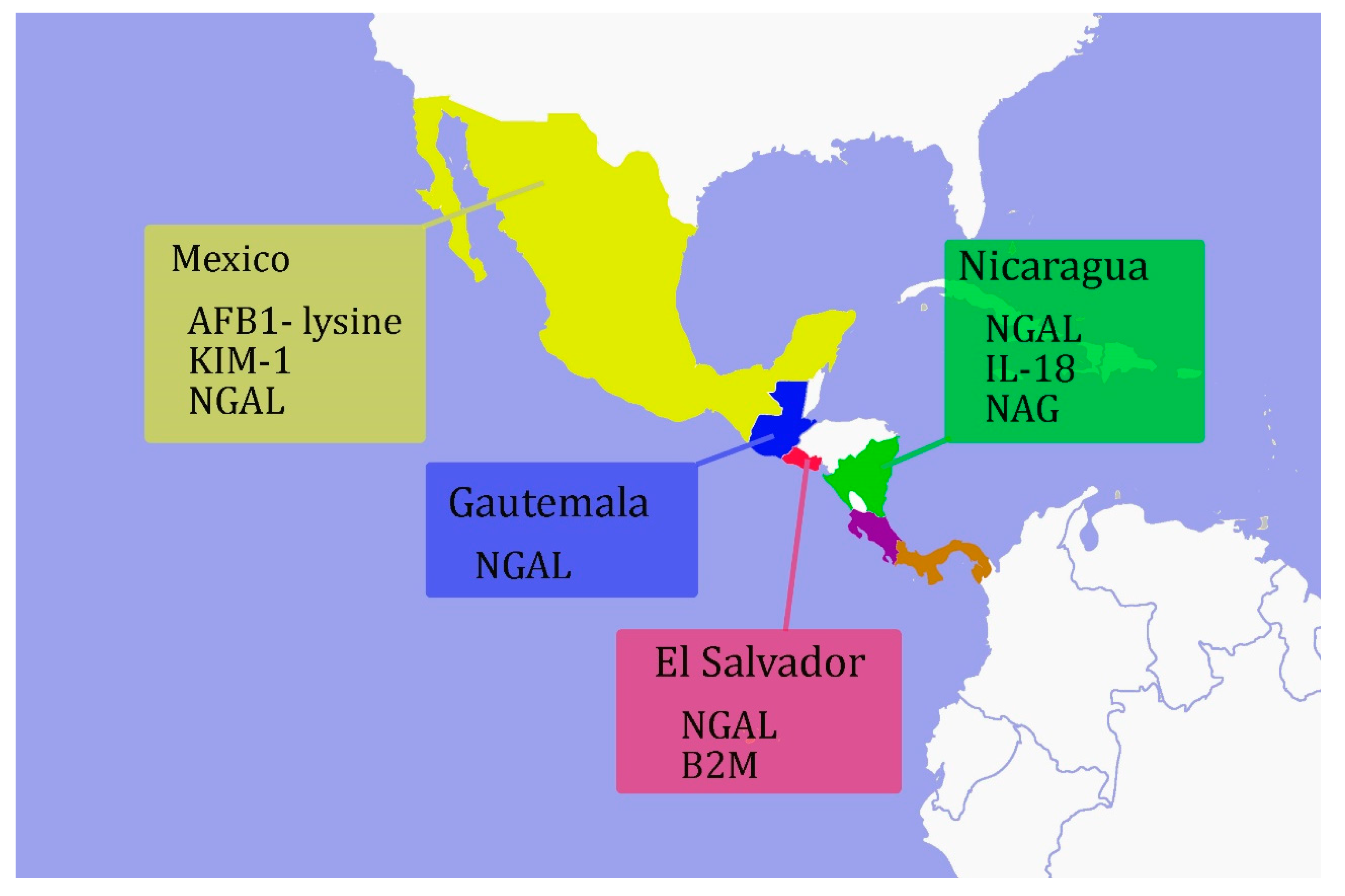
5.1. Mesoamerica
5.2. Sri Lanka
5.3. India
5.4. Egypt
5.5. Indonesia
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| A1M | α1-microglobulin. |
| ACR | albumin–creatinine ratio |
| AFB1 | aflatoxin-B1 |
| AKI | acute kidney injury |
| B2M | β2- macroglobulin |
| BUN | blood urea nitrogen |
| CKD | chronic kidney disease |
| CKDu | chronic kidney disease of unknown etiology |
| CLU | clusterin |
| CysC | cystatin-C |
| DALYS | disability-adjusted life years |
| eGFR | estimated glomerular filtration rate |
| FDA | food and drug administration |
| FN1 | fibronectin- 1 |
| GCLC | glutamate-cysteine ligase catalytic |
| GFR | glomerular filtration rate |
| GSTM1 | glutathione-S-transferase mu 1 |
| HGF | hepatocyte growth factor |
| HIV | human immune virus |
| IGFBP | insulin-like growth factor binding protein |
| IL-18 | interleukin-18 |
| KDIGO | Kidney disease: improving global outcomes |
| KIM-1 | kidney injury molecule -1 |
| L-FABP | liver type fatty acid binding protein |
| KLK1 | kallikrein-1 |
| NAG | N-acetyl-beta-D-glucosaminidase |
| NGAL | neutrophil gelatinase-associated lipocalin |
| NIH | National Institutes of Health |
| NLR | nod-like receptor |
| NLRP3 | NLR family pyrin domain containing 3 |
| OPN | osteopontin |
| Pi-GST | glutathione S-transferase |
| RBP | retinol binding protein |
| RRT | renal replacement therapy |
| SCR | serum creatinine |
| TIMP-2 | tissue inhibitor metalloproteinase-2 |
| uNGAL | urinary neutrophil gelatinase-associated lipocalin |
| μUNPD | micro-urine nano particle detection |
References
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed]
- Barsoum, R.S. Chronic Kidney Disease in the Developing World. N. Engl. J. Med. 2006, 354, 997–999. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic Kidney Disease: Global Dimension and Perspectives. Lancet Lond. Engl. 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Barber, R.M.; Foreman, K.J.; Lopez, A.D.; Vos, T.; GBD 2013 DALYs and HALE Collaborators. Global, Regional, and National Disability-Adjusted Life Years (DALYs) for 306 Diseases and Injuries and Healthy Life Expectancy (HALE) for 188 Countries, 1990–2013: Quantifying the Epidemiological Transition. Lancet Lond. Engl. 2015, 386, 2145–2191. [Google Scholar] [CrossRef]
- Mendley, S.R.; Levin, A.; Correa-Rotter, R.; Joubert, B.R.; Whelan, E.A.; Curwin, B.; Koritzinsky, E.H.; Gaughan, D.M.; Kimmel, P.L.; Anand, S.; et al. Chronic Kidney Diseases in Agricultural Communities: Report from a Workshop. Kidney Int. 2019, 96, 1071–1076. [Google Scholar] [CrossRef]
- Vervaet, B.A.; Nast, C.C.; Jayasumana, C.; Schreurs, G.; Roels, F.; Herath, C.; Kojc, N.; Samaee, V.; Rodrigo, S.; Gowrishankar, S.; et al. Chronic Interstitial Nephritis in Agricultural Communities is a Toxin-Induced Proximal Tubular Nephropathy. Kidney Int. 2020, 97, 350–369. [Google Scholar] [CrossRef]
- Athuraliya, N.T.C.; Abeysekera, T.D.J.; Amerasinghe, P.H.; Kumarasiri, R.; Bandara, P.; Karunaratne, U.; Milton, A.H.; Jones, A.L. Uncertain Etiologies of Proteinuric-Chronic Kidney Disease in Rural Sri Lanka. Kidney Int. 2011, 80, 1212–1221. [Google Scholar] [CrossRef]
- González-Quiroz, M.; Pearce, N.; Caplin, B.; Nitsch, D. What Do Epidemiological Studies Tell Us about Chronic Kidney Disease of Undetermined Cause in Meso-America? A Systematic Review and Meta-Analysis. Clin. Kidney J. 2018, 11, 496–506. [Google Scholar] [CrossRef]
- Gifford, F.J.; Gifford, R.M.; Eddleston, M.; Dhaun, N. Endemic Nephropathy Around the World. Kidney Int. Rep. 2017, 2, 282–292. [Google Scholar] [CrossRef]
- Jha, V.; Ur-Rashid, H.; Agarwal, S.K.; Akhtar, S.F.; Kafle, R.K.; Sheriff, R. ISN South Asia Regional Board. The State of Nephrology in South Asia. Kidney Int. 2019, 95, 31–37. [Google Scholar] [CrossRef]
- Fitria, L.; Prihartono, N.A.; Ramdhan, D.H.; Wahyono, T.Y.M.; Kongtip, P.; Woskie, S. Environmental and Occupational Risk Factors Associated with Chronic Kidney Disease of Unknown Etiology in West Javanese Rice Farmers, Indonesia. Int. J. Environ. Res. Public. Health 2020, 17, 4521. [Google Scholar] [CrossRef]
- Glaser, J.; Lemery, J.; Rajagopalan, B.; Diaz, H.F.; García-Trabanino, R.; Taduri, G.; Madero, M.; Amarasinghe, M.; Abraham, G.; Anutrakulchai, S.; et al. Climate Change and the Emergent Epidemic of CKD from Heat Stress in Rural Communities: The Case for Heat Stress Nephropathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- McKinley, J.M.; Mueller, U.; Atkinson, P.M.; Ofterdinger, U.; Cox, S.F.; Doherty, R.; Fogarty, D.; Egozcue, J.J.; Pawlowsky-Glahn, V. Chronic Kidney Disease of Unknown Origin Is Associated with Environmental Urbanisation in Belfast, UK. Environ. Geochem. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Jayasumana, C.; Orantes, C.; Herrera, R.; Almaguer, M.; Lopez, L.; Silva, L.C.; Ordunez, P.; Siribaddana, S.; Gunatilake, S.; De Broe, M.E. Chronic Interstitial Nephritis in Agricultural Communities: A Worldwide Epidemic with Social, Occupational and Environmental Determinants. Nephrol. Dial. Transpl. 2017, 32, 234–241. [Google Scholar] [CrossRef]
- Wijkström, J.; Jayasumana, C.; Dassanayake, R.; Priyawardane, N.; Godakanda, N.; Siribaddana, S.; Ring, A.; Hultenby, K.; Söderberg, M.; Elinder, C.-G.; et al. Morphological and Clinical Findings in Sri Lankan Patients with Chronic Kidney Disease of Unknown Cause (CKDu): Similarities and Differences with Mesoamerican Nephropathy. PLoS ONE 2018, 13, e0193056. [Google Scholar] [CrossRef]
- Ranasinghe, A.V.; Kumara, G.W.G.P.; Karunarathna, R.H.; De Silva, A.P.; Sachintani, K.G.D.; Gunawardena, J.M.C.N.; Kumari, S.K.C.R.; Sarjana, M.S.F.; Chandraguptha, J.S.; De Silva, M.V.C. The Incidence, Prevalence and Trends of Chronic Kidney Disease and Chronic Kidney Disease of Uncertain Aetiology (CKDu) in the North Central Province of Sri Lanka: An Analysis of 30,566 Patients. BMC Nephrol. 2019, 20, 338. [Google Scholar] [CrossRef]
- Ruwanpathirana, T.; Senanayake, S.; Gunawardana, N.; Munasinghe, A.; Ginige, S.; Gamage, D.; Amarasekara, J.; Lokuketagoda, B.; Chulasiri, P.; Amunugama, S.; et al. Prevalence and Risk Factors for Impaired Kidney Function in the District of Anuradhapura, Sri Lanka: A Cross-Sectional Population-Representative Survey in Those at Risk of Chronic Kidney Disease of Unknown Aetiology. BMC Public Health 2019, 19, 763. [Google Scholar] [CrossRef]
- Selvarajah, M.; Weeratunga, P.; Sivayoganthan, S.; Rathnatunga, N.; Rajapakse, S. Clinicopathological Correlates of Chronic Kidney Disease of Unknown Etiology in Sri Lanka. Indian J. Nephrol. 2016, 26, 357–363. [Google Scholar] [CrossRef]
- Nanayakkara, S.; Komiya, T.; Ratnatunga, N.; Senevirathna, S.T.M.L.D.; Harada, K.H.; Hitomi, T.; Gobe, G.; Muso, E.; Abeysekera, T.; Koizumi, A. Tubulointerstitial Damage as the Major Pathological Lesion in Endemic Chronic Kidney Disease among Farmers in North Central Province of Sri Lanka. Environ. Health Prev. Med. 2012, 17, 213–221. [Google Scholar] [CrossRef]
- López-Marín, L.; Chávez, Y.; García, X.A.; Flores, W.M.; García, Y.M.; Herrera, R.; Almaguer, M.; Orantes, C.M.; Calero, D.; Bayarre, H.D.; et al. Histopathology of Chronic Kidney Disease of Unknown Etiology in Salvadoran Agricultural Communities. Med. Rev. 2014, 16, 49–54. [Google Scholar]
- Cohen, J. Mesoamerica’s Mystery Killer. Science 2014, 344, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Wanigasuriya, K. Update on Uncertain Etiology of Chronic Kidney Disease in Sri Lanka’s North-Central Dry Zone. Med. Rev. 2014, 16, 61–65. [Google Scholar]
- Murray, C.J.L.; Lopez, A.D. Measuring the Global Burden of Disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [PubMed]
- GBD Chronic Kidney Disease Collaboration. Global, Regional, and National Burden of Chronic Kidney Disease, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Lond. Engl. 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Fernando, B.N.T.W.; Sudeshika, T.S.H.; Hettiarachchi, T.W.; Badurdeen, Z.; Abeysekara, T.D.J.; Abeysundara, H.T.K.; Jayasinghe, S.; Ranasighe, S.; Nanayakkara, N. Evaluation of Biochemical Profile of Chronic Kidney Disease of Uncertain Etiology in Sri Lanka. PLoS ONE 2020, 15, e0232522. [Google Scholar] [CrossRef]
- Tatapudi, R.R.; Rentala, S.; Gullipalli, P.; Komarraju, A.L.; Singh, A.K.; Tatapudi, V.S.; Goru, K.B.; Bhimarasetty, D.M.; Narni, H. High Prevalence of CKD of Unknown Etiology in Uddanam, India. Kidney Int. Rep. 2019, 4, 380–389. [Google Scholar] [CrossRef]
- Lebov, J.F.; Valladares, E.; Peña, R.; Peña, E.M.; Sanoff, S.L.; Cisneros, E.C.; Colindres, R.E.; Morgan, D.R.; Hogan, S.L. A Population-Based Study of Prevalence and Risk Factors of Chronic Kidney Disease in León, Nicaragua. Can. J. Kidney Health Dis. 2015, 2, 6. [Google Scholar] [CrossRef]
- Jayasumana, C.; Paranagama, P.; Agampodi, S.; Wijewardane, C.; Gunatilake, S.; Siribaddana, S. Drinking Well Water and Occupational Exposure to Herbicides Is Associated with Chronic Kidney Disease, in Padavi-Sripura, Sri Lanka. Environ. Health Glob. Access Sci. Source 2015, 14, 6. [Google Scholar] [CrossRef]
- Babich, R.; Ulrich, J.C.; Ekanayake, E.M.D.V.; Massarsky, A.; De Silva, P.M.C.S.; Manage, P.M.; Jackson, B.P.; Ferguson, P.L.; Di Giulio, R.T.; Drummond, I.A.; et al. Kidney Developmental Effects of Metal-Herbicide Mixtures: Implications for Chronic Kidney Disease of Unknown Etiology. Environ. Int. 2020, 144, 106019. [Google Scholar] [CrossRef]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; José Vindell, J.; Stockfelt, L.; Roncal, C.; et al. Heat Stress, Dehydration, and Kidney Function in Sugarcane Cutters in El Salvador—A Cross-Shift Study of Workers at Risk of Mesoamerican Nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef]
- Roncal-Jimenez, C.; Lanaspa, M.A.; Jensen, T.; Sanchez-Lozada, L.G.; Johnson, R.J. Mechanisms by Which Dehydration May Lead to Chronic Kidney Disease. Ann. Nutr. Metab. 2015, 66 (Suppl. 3), 10–13. [Google Scholar] [CrossRef] [PubMed]
- Xing, W.M.; Yuan, T.J.; Xu, J.D.; Gu, L.L.; Liang, P.; Lu, H. Proteomic Identification of Mitochondrial Targets Involved in Andrographolide Sodium Bisulfite-Induced Nephrotoxicity in a Rat Model. Environ. Toxicol. Pharm. 2015, 40, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Perera, T.; Ranasinghe, S.; Alles, N.; Waduge, R. Experimental Rat Model for Acute Tubular Injury Induced by High Water Hardness and High Water Fluoride: Efficacy of Primary Preventive Intervention by Distilled Water Administration. BMC Nephrol. 2020, 21, 103. [Google Scholar] [CrossRef] [PubMed]
- Roncal-Jimenez, C.; García-Trabanino, R.; Barregard, L.; Lanaspa, M.A.; Wesseling, C.; Harra, T.; Aragón, A.; Grases, F.; Jarquin, E.R.; González, M.A.; et al. Heat Stress Nephropathy from Exercise-Induced Uric Acid Crystalluria: A Perspective on Mesoamerican Nephropathy. Am. J. Kidney Dis. 2016, 67, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-W. Leptospirosis Renal Disease: Emerging Culprit of Chronic Kidney Disease Unknown Etiology. Nephron 2018, 138, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, S.; Senevirathna, S.T.M.L.D.; Parahitiyawa, N.B.; Abeysekera, T.; Chandrajith, R.; Ratnatunga, N.; Hitomi, T.; Kobayashi, H.; Harada, K.H.; Koizumi, A. Whole-Exome Sequencing Reveals Genetic Variants Associated with Chronic Kidney Disease Characterized by Tubulointerstitial Damages in North Central Region, Sri Lanka. Environ. Health Prev. Med. 2015, 20, 354–359. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Bobadilla, N.A.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J.; Barregard, L. Kidney Function in Sugarcane Cutters in Nicaragua—A Longitudinal Study of Workers at Risk of Mesoamerican Nephropathy. Environ. Res. 2016, 147, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Correa-Rotter, R.; Wesseling, C.; Johnson, R.J. CKD of Unknown Origin in Central America: The Case for a Mesoamerican Nephropathy. Am. J. Kidney Dis. 2014, 63, 506–520. [Google Scholar] [CrossRef] [PubMed]
- Lunyera, J.; Mohottige, D.; Von Isenburg, M.; Jeuland, M.; Patel, U.D.; Stanifer, J.W. CKD of Uncertain Etiology: A Systematic Review. Clin. J. Am. Soc. Nephrol. 2016, 11, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Rivard, C.J.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J. Heat Stress, Hydration and Uric Acid: A Cross-Sectional Study in Workers of Three Occupations in a Hotspot of Mesoamerican Nephropathy in Nicaragua. BMJ Open 2016, 6, e011034. [Google Scholar] [CrossRef]
- VanDervort, D.R.; López, D.L.; Orantes, C.M.; Rodríguez, D.S. Spatial Distribution of Unspecified Chronic Kidney Disease in El Salvador by Crop Area Cultivated and Ambient Temperature. Med. Rev. 2014, 16, 31–38. [Google Scholar]
- Herath, C.; Jayasumana, C.; De Silva, P.M.C.S.; De Silva, P.H.C.; Siribaddana, S.; De Broe, M.E. Kidney Diseases in Agricultural Communities: A Case Against Heat-Stress Nephropathy. Kidney Int. Rep. 2018, 3, 271–280. [Google Scholar] [CrossRef]
- Weaver, V.M.; Fadrowski, J.J.; Jaar, B.G. Global Dimensions of Chronic Kidney Disease of Unknown Etiology (CKDu): A Modern Era Environmental and/or Occupational Nephropathy? BMC Nephrol. 2015, 16, 145. [Google Scholar] [CrossRef] [PubMed]
- Petejova, N.; Martinek, A.; Zadrazil, J.; Teplan, V. Acute Toxic Kidney Injury. Ren. Fail. 2019, 41, 576–594. [Google Scholar] [CrossRef] [PubMed]
- Orr, S.E.; Bridges, C.C. Chronic Kidney Disease and Exposure to Nephrotoxic Metals. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef]
- Nanayakkara, S.; Senevirathna, S.T.M.L.D.; Harada, K.H.; Chandrajith, R.; Hitomi, T.; Abeysekera, T.; Muso, E.; Watanabe, T.; Koizumi, A. Systematic Evaluation of Exposure to Trace Elements and Minerals in Patients with Chronic Kidney Disease of Uncertain Etiology (CKDu) in Sri Lanka. J. Trace Elem. Med. Biol. 2019, 54, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, S.; Senevirathna, S.T.M.L.D.; Karunaratne, U.; Chandrajith, R.; Harada, K.H.; Hitomi, T.; Watanabe, T.; Abeysekera, T.; Aturaliya, T.N.C.; Koizumi, A. Evidence of Tubular Damage in the Very Early Stage of Chronic Kidney Disease of Uncertain Etiology in the North Central Province of Sri Lanka: A Cross-Sectional Study. Environ. Health Prev. Med. 2012, 17, 109–117. [Google Scholar] [CrossRef]
- Kim, N.H.; Hyun, Y.Y.; Lee, K.-B.; Chang, Y.; Ryu, S.; Rhu, S.; Oh, K.-H.; Ahn, C. Environmental Heavy Metal Exposure and Chronic Kidney Disease in the General Population. J. Korean Med. Sci. 2015, 30, 272–277. [Google Scholar] [CrossRef]
- Chandrajith, R.; Dissanayake, C.B.; Ariyarathna, T.; Herath, H.M.J.M.K.; Padmasiri, J.P. Dose-Dependent Na and Ca in Fluoride-Rich Drinking Water--Another Major Cause of Chronic Renal Failure in Tropical Arid Regions. Sci. Total Environ. 2011, 409, 671–675. [Google Scholar] [CrossRef]
- Vanherweghem, J.L.; Depierreux, M.; Tielemans, C.; Abramowicz, D.; Dratwa, M.; Jadoul, M.; Richard, C.; Vandervelde, D.; Verbeelen, D.; Vanhaelen-Fastre, R. Rapidly Progressive Interstitial Renal Fibrosis in Young Women: Association with Slimming Regimen Including Chinese Herbs. Lancet Lond. Engl. 1993, 341, 387–391. [Google Scholar] [CrossRef]
- Debelle, F.D.; Vanherweghem, J.-L.; Nortier, J.L. Aristolochic Acid Nephropathy: A Worldwide Problem. Kidney Int. 2008, 74, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Depierreux, M.; Van Damme, B.; Vanden Houte, K.; Vanherweghem, J.L. Pathologic Aspects of a Newly Described Nephropathy Related to the Prolonged Use of Chinese Herbs. Am. J. Kidney Dis. 1994, 24, 172–180. [Google Scholar] [CrossRef]
- Cosyns, J.P.; Dehoux, J.P.; Guiot, Y.; Goebbels, R.M.; Robert, A.; Bernard, A.M.; van Ypersele de Strihou, C. Chronic Aristolochic Acid Toxicity in Rabbits: A Model of Chinese Herbs Nephropathy? Kidney Int. 2001, 59, 2164–2173. [Google Scholar] [CrossRef]
- Sato, N.; Takahashi, D.; Chen, S.-M.; Tsuchiya, R.; Mukoyama, T.; Yamagata, S.; Ogawa, M.; Yoshida, M.; Kondo, S.; Satoh, N.; et al. Acute Nephrotoxicity of Aristolochic Acids in Mice. J. Pharm. Pharmacol. 2004, 56, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Gamage, C.D.; Yoshimatsu, K.; Sarathkumara, Y.D.; Kulendiran, T.; Nanayakkara, N.; Arikawa, J. Serological Evidence of Hantavirus Infection in Girandurukotte, an Area Endemic for Chronic Kidney Disease of Unknown Aetiology (CKDu) in Sri Lanka. Int. J. Infect. Dis. 2017, 57, 77–78. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA; National Institutes of Health (US): Bethesda, MD, USA, 2020. [Google Scholar]
- Etzioni, R.; Urban, N.; Ramsey, S.; McIntosh, M.; Schwartz, S.; Reid, B.; Radich, J.; Anderson, G.; Hartwell, L. The Case for Early Detection. Nat. Rev. Cancer 2003, 3, 243–252. [Google Scholar] [CrossRef]
- Yu, A.; Chertow, G.; Luyckx, V.; Marsden, P.; Skorecki, K.; Taal, M. Brenner & Rector’s the Kidney, 11th ed.; Elsevier Inc: Philadelphia, PA, USA, 2019. [Google Scholar]
- Ostermann, M.; Philips, B.J.; Forni, L.G. Clinical Review: Biomarkers of Acute Kidney Injury: Where Are We Now? Crit. Care Lond. Engl. 2012, 16, 233. [Google Scholar] [CrossRef]
- Murray, P.T.; Mehta, R.L.; Shaw, A.; Ronco, C.; Endre, Z.; Kellum, J.A.; Chawla, L.S.; Cruz, D.; Ince, C.; Okusa, M.D.; et al. Potential Use of Biomarkers in Acute Kidney Injury: Report and Summary of Recommendations from the 10th Acute Dialysis Quality Initiative Consensus Conference. Kidney Int. 2014, 85, 513–521. [Google Scholar] [CrossRef]
- Food and Drug Administration US (FDA). List of Qualified Biomarkers; FDA: Silver Spring, MD, USA, 2020. [Google Scholar]
- Trabanino, R.G.; Aguilar, R.; Silva, C.R.; Mercado, M.O.; Merino, R.L. End-stage renal disease among patients in a referral hospital in El Salvador. Rev. Panam. Salud Publica 2002, 12, 202–206. [Google Scholar] [CrossRef]
- Torres, C.; Aragón, A.; González, M.; López, I.; Jakobsson, K.; Elinder, C.-G.; Lundberg, I.; Wesseling, C. Decreased Kidney Function of Unknown Cause in Nicaragua: A Community-Based Survey. Am. J. Kidney Dis. 2010, 55, 485–496. [Google Scholar] [CrossRef]
- Sanoff, S.L.; Callejas, L.; Alonso, C.D.; Hu, Y.; Colindres, R.E.; Chin, H.; Morgan, D.R.; Hogan, S.L. Positive Association of Renal Insufficiency with Agriculture Employment and Unregulated Alcohol Consumption in Nicaragua. Ren. Fail. 2010, 32, 766–777. [Google Scholar] [CrossRef]
- González-Quiroz, M.; Camacho, A.; Faber, D.; Aragón, A.; Wesseling, C.; Glaser, J.; Le Blond, J.; Smeeth, L.; Nitsch, D.; Pearce, N.; et al. Rationale, Description and Baseline Findings of a Community-Based Prospective Cohort Study of Kidney Function amongst the Young Rural Population of Northwest Nicaragua. BMC Nephrol. 2017, 18, 16. [Google Scholar] [CrossRef]
- Gonzalez-Quiroz, M.; Smpokou, E.-T.; Pearce, N.; Caplin, B.; Nitsch, D. Identification of Young Adults at Risk of an Accelerated Loss of Kidney Function in an Area Affected by Mesoamerican Nephropathy. BMC Nephrol. 2019, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, C.J.; Butler-Dawson, J.; Dally, M.; Krisher, L.; Griffin, B.R.; Johnson, R.J.; Lemery, J.; Asensio, C.; Tenney, L.; Newman, L.S. Risk Factors and Mechanisms Underlying Cross-Shift Decline in Kidney Function in Guatemalan Sugarcane Workers. J. Occup. Environ. Med. 2019, 61, 239–250. [Google Scholar] [CrossRef]
- Gonzalez-Quiroz, M.; Smpokou, E.-T.; Silverwood, R.J.; Camacho, A.; Faber, D.; Garcia, B.L.R.; Oomatia, A.; Hill, M.; Glaser, J.; Le Blond, J.; et al. Decline in Kidney Function among Apparently Healthy Young Adults at Risk of Mesoamerican Nephropathy. J. Am. Soc. Nephrol. 2018, 29, 2200–2212. [Google Scholar] [CrossRef] [PubMed]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramírez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, J.M.; et al. Biomarkers of Kidney Injury Among Nicaraguan Sugarcane Workers. Am. J. Kidney Dis. 2016, 67, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Herrera Valdés, R.; Orantes, C.M.; Almaguer López, M.; López Marín, L.; Arévalo, P.A.; Smith González, M.J.; Morales, F.E.; Bacallao, R.; Bayarre, H.D.; Vela Parada, X.F. Clinical Characteristics of Chronic Kidney Disease of Non-Traditional Causes in Women of Agricultural Communities in El Salvador. Clin. Nephrol. 2015, 83 (Suppl. 1), 56–63. [Google Scholar] [CrossRef]
- Ramírez-Rubio, O.; Amador, J.J.; Kaufman, J.S.; Weiner, D.E.; Parikh, C.R.; Khan, U.; McClean, M.D.; Laws, R.L.; López-Pilarte, D.; Friedman, D.J.; et al. Urine Biomarkers of Kidney Injury among Adolescents in Nicaragua, a Region Affected by an Epidemic of Chronic Kidney Disease of Unknown Aetiology. Nephrol. Dial. Transpl. 2016, 31, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Leibler, J.H.; Ramirez-Rubio, O.; Velázquez, J.J.A.; Pilarte, D.L.; Obeid, W.; Parikh, C.R.; Gadupudi, S.; Scammell, M.K.; Friedman, D.J.; Brooks, D.R. Biomarkers of Kidney Injury among Children in a High-Risk Region for Chronic Kidney Disease of Uncertain Etiology. Pediatr. Nephrol. Berl. Ger. 2020. [Google Scholar] [CrossRef] [PubMed]
- Orantes Navarro, C.; Herrera-Valdés, R.; Almaguer-López, M.; Brizuela-Díaz, E.; Alvarado-Ascencio, N.; Morales, E.; Bayarre, H.; Calero-Brizuela, D.; Vela Parada, X.; Zelaya-Quezada, S. Chronic Kidney Disease in Children and Adolescents in Salvadoran Farming Communities: NefroSalva Pediatric Study (2009–2011). Med. Rev. 2016, 18, 15–21. [Google Scholar] [CrossRef]
- Agampodi, S.B.; Amarasinghe, G.S.; Naotunna, P.G.C.R.; Jayasumana, C.S.; Siribaddana, S.H. Early Renal Damage among Children Living in the Region of Highest Burden of Chronic Kidney Disease of Unknown Etiology (CKDu) in Sri Lanka. BMC Nephrol. 2018, 19, 115. [Google Scholar] [CrossRef] [PubMed]
- Díaz de León-Martínez, L.; Díaz-Barriga, F.; Barbier, O.; Ortíz, D.L.G.; Ortega-Romero, M.; Pérez-Vázquez, F.; Flores-Ramírez, R. Evaluation of Emerging Biomarkers of Renal Damage and Exposure to Aflatoxin-B1 in Mexican Indigenous Women: A Pilot Study. Environ. Sci. Pollut. Res. Int. 2019, 26, 12205–12216. [Google Scholar] [CrossRef] [PubMed]
- Riefkohl, A.; Ramírez-Rubio, O.; Laws, R.L.; McClean, M.D.; Weiner, D.E.; Kaufman, J.S.; Galloway, R.L.; Shadomy, S.V.; Guerra, M.; Amador, J.J.; et al. Leptospira Seropositivity as a Risk Factor for Mesoamerican Nephropathy. Int. J. Occup. Environ. Health 2017, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jayasumana, C.; Gajanayake, R.; Siribaddana, S. Importance of Arsenic and Pesticides in Epidemic Chronic Kidney Disease in Sri Lanka. BMC Nephrol. 2014, 15, 124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kafle, K.; Balasubramanya, S.; Horbulyk, T. Prevalence of Chronic Kidney Disease in Sri Lanka: A Profile of Affected Districts Reliant on Groundwater. Sci. Total Environ. 2019, 694, 133767. [Google Scholar] [CrossRef]
- Ratnayake, S.; Badurdeen, Z.; Nanayakkara, N.; Abeysekara, T.; Ratnatunga, N.; Kumarasiri, R. Screening for Chronic Kidney Disease of Uncertain Aetiology in Sri Lanka: Usability of Surrogate Biomarkers over Dipstick Proteinuria. BMC Nephrol. 2017, 18, 199. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.M.C.S.; Mohammed Abdul, K.S.; Eakanayake, E.M.D.V.; Jayasinghe, S.S.; Jayasumana, C.; Asanthi, H.B.; Perera, H.S.D.; Chaminda, G.G.T.; Chandana, E.P.S.; Siribaddana, S.H. Urinary Biomarkers KIM-1 and NGAL for Detection of Chronic Kidney Disease of Uncertain Etiology (CKDu) among Agricultural Communities in Sri Lanka. PLoS Negl. Trop. Dis. 2016, 10, e0004979. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.J.; Pellegrini, K.L.; Chung, J.; Wanigasuriya, K.; Jayawardene, I.; Lee, K.; Lee, H.; Vaidya, V.S.; Weissleder, R. Nanoparticle Detection of Urinary Markers for Point-of-Care Diagnosis of Kidney Injury. PLoS ONE 2015, 10, e0133417. [Google Scholar] [CrossRef]
- Sayanthooran, S.; Magana-Arachchi, D.N.; Gunerathne, L.; Abeysekera, T. Potential Diagnostic Biomarkers for Chronic Kidney Disease of Unknown Etiology (CKDu) in Sri Lanka: A Pilot Study. BMC Nephrol. 2017, 18, 31. [Google Scholar] [CrossRef]
- Sayanthooran, S.; Magana-Arachchi, D.N.; Gunerathne, L.; Abeysekera, T.D.J.; Sooriyapathirana, S.S. Upregulation of Oxidative Stress Related Genes in a Chronic Kidney Disease Attributed to Specific Geographical Locations of Sri Lanka. Biomed. Res. Int. 2016, 2016, 7546265. [Google Scholar] [CrossRef]
- Fernando, B.N.T.W.; Alli-Shaik, A.; Hemage, R.K.D.; Badurdeen, Z.; Hettiarachchi, T.W.; Abeysundara, H.T.K.; Abeysekara, T.D.J.; Wazil, A.; Rathnayake, S.; Gunaratne, J.; et al. Pilot Study of Renal Urinary Biomarkers for Diagnosis of CKD of Uncertain Etiology. Kidney Int. Rep. 2019, 4, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Wanigasuriya, K.; Jayawardene, I.; Amarasiriwardena, C.; Wickremasinghe, R. Novel Urinary Biomarkers and Their Association with Urinary Heavy Metals in Chronic Kidney Disease of Unknown Aetiology in Sri Lanka: A Pilot Study. Ceylon Med. J. 2017, 62, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Siriwardhana, E.A.R.I.E.; Perera, P.A.J.; Sivakanesan, R.; Abeysekara, T.; Nugegoda, D.B.; Weerakoon, K.G.A.D. Is the Staple Diet Eaten in Medawachchiya, Sri Lanka, a Predisposing Factor in the Development of Chronic Kidney Disease of Unknown Etiology?—A Comparison Based on Urinary Β2-Microglobulin Measurements. BMC Nephrol. 2014, 15, 103. [Google Scholar] [CrossRef] [PubMed]
- Safouh, H.; Fadel, F.; Essam, R.; Salah, A.; Bekhet, A. Causes of Chronic Kidney Disease in Egyptian Children. Saudi J. Kidney Dis. Transpl. 2015, 26, 806–809. [Google Scholar] [CrossRef]
- Ghonemy, T.A.; Farag, S.E.; Soliman, S.A.; El-okely, A.; El-hendy, Y. Epidemiology and Risk Factors of Chronic Kidney Disease in the El-Sharkia Governorate, Egypt. Saudi J. Kidney Dis. Transpl. 2016, 27, 111–117. [Google Scholar] [CrossRef]
- Nejat, M.; Pickering, J.W.; Devarajan, P.; Bonventre, J.V.; Edelstein, C.L.; Walker, R.J.; Endre, Z.H. Some Biomarkers of Acute Kidney Injury Are Increased in Pre-Renal Acute Injury. Kidney Int. 2012, 81, 1254–1262. [Google Scholar] [CrossRef]
- Endre, Z.H. Recovery from Acute Kidney Injury: The Role of Biomarkers. Nephron Clin. Pract. 2014, 127, 101–105. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bio- Marker | Biochemical Significance | Site of Release in the Kidney | Clinical Significance |
|---|---|---|---|
| CLU | Referred to as apolipoprotein J (Apo J). 75–80 kDa glycoprotein. | Proximal tubule Dedifferentiated tubular cells Distal tubule | Elevated urinary expression observed in rat models of tubular proteinuria, but not in glomerular proteinuria. |
| CysC | Low molecular weight protein (13 kDa). Freely filtered at the glomerulus, subjected to reabsorption and catabolism, but not to tubular secretion. | Glomerulus Proximal tubule | Sensitive serum marker of GFR Prognostic marker of adverse outcomes such as renal replacement therapy. A predictive biomarker of cardiovascular events in patients with kidney diseases. |
| KIM-1 | A Highly conserved phosphatidylserine receptor of 38.7 kDa with a mucin-rich extracellular region. | Proximal tubule Dedifferentiated tubular cells | Proximal tubular injury marker A sensitive and early diagnostic marker of renal injury. Associated with tubule-interstitial fibrosis, tubular damage, and inflammation. |
| NAG | A proximal tubule lysosomal enzyme. | Proximal tubule | A sensitive and robust indicator of AKI Increased in impaired glucose tolerance, rheumatoid arthritis, and hyperthyroidism. |
| NGAL | 25 kDa lipocalin superfamily protein. A glycoprotein bound to matrix MMP-9 in human neutrophils. | Proximal tubule Distal tubule | A sensitive and early diagnostic marker of renal injury and AKI. Marked upregulation in proximal tubules within 3 h of ischemia/reperfusion injury. Also expressed in salivary glands, uterus, prostate, trachea, lung, stomach in addition to the kidney. |
| OPN | 44 kDa extracellular matrix glycol-phosphoprotein. Produced in high levels in bone tissue and epithelial cells. | Proximal tubule Loop of Henle Distal tubule | Marker of nephrotoxicity. Expressed with inflammation and tubulo-interstitial fibrosis in progressive idiopathic membranous nephropathy, crescentic glomerulonephritis, IgA nephritis, and diffuse proliferative lupus nephritis. Involved in remodeling and calcification of bones, cell adhesion, migration, and survival, immune responses and tumorigenesis. |
| A1M | 27 -30 kDa glycoprotein primarily synthesized by the liver. Detectable in human urine, serum and cerebrospinal fluid. Freely filtered at the glomerulus, subjected to complete reabsorption and catabolized by proximal tubular cells. | Proximal tubule | Elevated levels in urine reflects proximal tubular injury or dysfunction. Urinary levels increase with age. Plasma level varies with age, gender, liver diseases, ulcerative colitis, HIV infection, and mood disorders. |
| B2M | 13.7 kDa light chain MHC-I protein Expressed on all nucleated cells, serum, urine, and synovial fluid. Filtered at the glomerulus and almost entirely reabsorbed and catabolized by the proximal tubular cells. | Proximal tubule | Tubular injury marker in AKI and CKD. Increase in serum reflects the decrease in glomerular function in CKD. Elevated in cadmium toxicity, following cardiac surgery, liver and renal transplantation and idiopathic membranous nephropathy. |
| IL-18 | 18 kDa proinflammatory cytokine, activated via cleavage by caspase-1. Induced and cleaved mainly in the proximal tubules in human kidney and released into the urine. | Proximal tubule | Elevated urinary IL-18 levels are apparent in patients with kidney injury. |
| MCP-1 | 8.7 kDa protein of Chemotactic cytokine (chemokine) family. Produced in renal cells in response to proinflammatory cytokines. | Glomerular mesangial cells Podocytes Tubular epithelial cells | Expressed by renal cells following renal injury. Urinary MCP-1 is upregulated in inflammatory renal disease and diabetic nephropathy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunasekara, T.D.K.S.C.; De Silva, P.M.C.S.; Herath, C.; Siribaddana, S.; Siribaddana, N.; Jayasumana, C.; Jayasinghe, S.; Cardenas-Gonzalez, M.; Jayasundara, N. The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. Int. J. Environ. Res. Public Health 2020, 17, 9522. https://doi.org/10.3390/ijerph17249522
Gunasekara TDKSC, De Silva PMCS, Herath C, Siribaddana S, Siribaddana N, Jayasumana C, Jayasinghe S, Cardenas-Gonzalez M, Jayasundara N. The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9522. https://doi.org/10.3390/ijerph17249522
Chicago/Turabian StyleGunasekara, T.D.K.S.C., P. Mangala C.S. De Silva, Chula Herath, Sisira Siribaddana, Nipuna Siribaddana, Channa Jayasumana, Sudheera Jayasinghe, Maria Cardenas-Gonzalez, and Nishad Jayasundara. 2020. "The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review" International Journal of Environmental Research and Public Health 17, no. 24: 9522. https://doi.org/10.3390/ijerph17249522
APA StyleGunasekara, T. D. K. S. C., De Silva, P. M. C. S., Herath, C., Siribaddana, S., Siribaddana, N., Jayasumana, C., Jayasinghe, S., Cardenas-Gonzalez, M., & Jayasundara, N. (2020). The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. International Journal of Environmental Research and Public Health, 17(24), 9522. https://doi.org/10.3390/ijerph17249522