Recruiting and Engaging American Indian and Alaska Native Teens and Young Adults in a SMS Help-Seeking Intervention: Lessons Learned from the BRAVE Study


 ,
,  and
and 
Abstract
1. Introduction
1.1. mHealth Access in Indian Country
1.2. Efficacy of Technology-Based Interventions
1.3. Goal of this Study
1.4. Research Partners
2. Materials and Methods
2.1. Overview
2.2. Communication Theory
2.3. Behavioral Intervention
2.3.1. BRAVE Campaign Messages
2.3.2. BRAVE Role Model Videos
2.3.3. STEM Campaign Messages
2.4. Eligibility Criteria
We R Native is doing a study to evaluate a text messaging program and we think you might be eligible. Earn up to $40 for your time. It takes courage to change or to step up and help a friend. Reply BRAVE if you’re interested.
We R Native: Thanks for your interest in our study, but you must be AI/AN and 15–25 years old to participate. If you would like to receive text messages about science, engineering, technology, or medicine, reply with “STEM.” Or check out our other health resources at www.weRnative.org
2.5. Study Recruitment
Super! If you participate, you will receive either: 8 weeks of wellness messages designed to promote cultural pride and resilience, or 8 weeks of STEM messages designed to elevate Native voices in science, technology, engineering, and math.
Afterward, the two groups will switch and you’ll receive the other set of messages. Altogether, you’ll get 3–5 health msgs per week for 4 months. Earn $10 for answering four sets of Q’s over 8 months. More info about study is available at: http://lil.ms/1v5w
You may leave the study at any time by texting STOP. We will send you a pre-survey when the study begins.
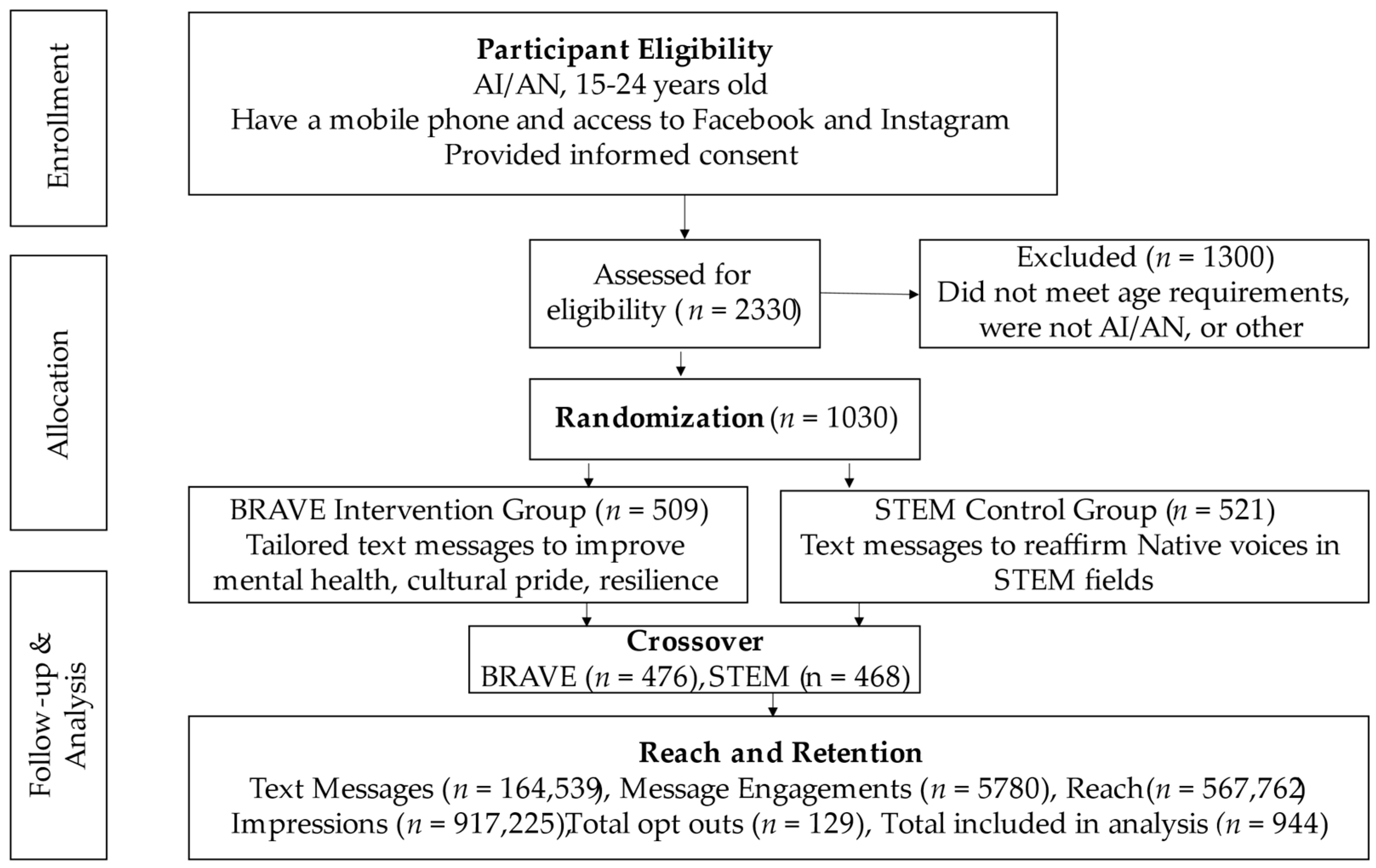
2.6. Enrollment
2.7. Brave Study Ad Design and Placement
2.8. Social Media Ads, Examples, Conversion Rates and Costs
2.9. Analysis
3. Results
3.1. SMS Message Analytics
3.1.1. Study Retention
3.1.2. Message Engagement
Video links requiring user engagement: Hey it’s Alex. I didn’t see it at the time, but Chris was my everything. The pow to my wow. The fry to my bread. The first real love of my life besides bball, and I f***ed it all up: Episode 2 (https://www.youtube.com/watch?v=9aRxIQd_62E&feature=youtu.be)
Text MORE engagement: Alex’s drinking was out of control. Drinking in moderation is defined as having no more than 1 drink per day for women and no more than 2 drinks per day for men. Drinking too much can cause lots of negative outcomes. Text MORE to learn more.
Additional MORE message: Regular excessive alcohol use is associated with hangovers, reduced sexual performance, aggressive behavior, accidents and injury, anxiety and depression, relationship difficulties, and suicide... just to name a few. Drinking in moderation (or not drinking at all) is the best way to keep in control.
Skill practice engagement: Many of us have grown up in traumatic environments. Now it’s up to us to break the cycle. Having people in our lives who love and care about us is one way to build resilience. Week 2 Challenge: Reach out to a friend or family member this week. Let them know you appreciate them and their support.
3.1.3. Message Engagement with a Call to Action
4. Discussion
4.1. Principal Findings
4.2. Limitations
4.3. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Craig Rushing, S.; Stephens, D. Use of media technologies by Native American teens and young adults in the Pacific Northwest: Exploring their utility for designing culturally appropriate technology-based health interventions. J. Prim. Prev. 2011, 32, 135–145. [Google Scholar] [CrossRef]
- Bee-Gates, D.; Howard-Pitney, B.; LaFromboise, T.; Rowe, W. Help-seeking behavior of Native American Indian high school students. Prof. Psychol. Res. Pract. 1996, 27, 495. [Google Scholar] [CrossRef]
- Schonert-Reichl, K.A.; Muller, J.R. Correlates of help-seeking in adolescence. J. Youth Adolesc. 1996, 25, 705–731. [Google Scholar] [CrossRef]
- Generation Indigenous: The State of Native Youth 2018. Available online: https://www.cnay.org/wp-content/uploads/2019/09/CNAY_AR2018_FINAL_Web_110618-2.pdf (accessed on 1 September 2020).
- Subica, A.M.; Wu, L.T. Substance Use and Suicide in Pacific Islander, American Indian, and Multiracial Youth. Am. J. Prev. Med. 2018, 54, 795–805. [Google Scholar] [CrossRef]
- Wexler, L.; Chandler, M.; Gone, J.P.; Cwik, M.; Kirmayer, L.J.; LaFromboise, T.; Brockie, T.; O’Keefe, V.; Walkup, J.; Allen, J. Advancing suicide prevention research with rural American Indian and Alaska Native populations. Am. J. Public Health 2015, 105, 891–899. [Google Scholar] [CrossRef]
- Bartgis, J.; Albright, G. Online role-play simulations with emotionally responsive avatars for the early detection of Native youth psychological distress, including depression and suicidal ideation. Am. Indian Alsk. Nativ. Ment. Health Res. 2016, 23, 1–27. [Google Scholar] [CrossRef]
- Compressed Mortality File 1999–2015 on CDC WONDER Online Database. Available online: https://wonder.cdc.gov/controller/datarequest/D132;jsessionid=CB6D30304A7A062BF98C5C2202BF535B (accessed on 1 September 2020).
- Kaufman, C.E.; Schwinn, T.M.; Black, K.; Keane, E.M.; Big Crow, C.K. The Promise of Technology to Advance Rigorous Evaluation of Adolescent Pregnancy Prevention Programs in American Indian and Alaska Native Tribal Communities. Am. J. Public Health 2016, 106, S18–S20. [Google Scholar] [CrossRef]
- Use of Media Technologies by Native American Teens and Young Adults: Evaluating Their Utility for Designing Culturally-Appropriate Sexual Health Interventions Targeting Native Youth in the Pacific Northwest. Available online: http://dr.archives.pdx.edu/xmlui/handle/psu/4743 (accessed on 1 September 2020).
- Youth Health Tech Media Surveys. 2017. Available online: http://www.npaihb.org/wernative (accessed on 1 September 2020).
- Rushing, S.C.; Gaston, A.; Kaufman, C.; Markham, C.; Jessen, C.; Gorman, G. Using Technology to Promote Health and Wellbeing among American Indian and Alaska Native Teens and Young Adults. In Indigenous People and Mobile Technologies; Dyson, L.E., Grant, S., Hendriks, M., Eds.; Routledge: New York, NY, USA, 2016; Volume 1, pp. 1–340. [Google Scholar] [CrossRef]
- Chavez, N.R.; Shearer, L.S.; Rosenthal, S.L. Use of Digital Media Technology for Primary Prevention of STIs/HIV in Youth. J. Pediatr. Adolesc. Gynecol. 2013. [Google Scholar] [CrossRef]
- Berrouiguet, S.; Baca-Garcia, E.; Brandt, S.; Walter, M.; Courtet, P. Fundamentals for Future Mobile-Health (mHealth): A Systematic Review of Mobile Phone and Web-Based Text Messaging in Mental Health. J. Med. Internet Res. 2016, 18. [Google Scholar] [CrossRef]
- Cash, S.J.; Rushing, S.C.; Stephens, D. Comprehensive Approaches Using Technology to Address Mental Health. In Technology and Adolescent Mental Health; Moreno, M.A., Radovic, A., Eds.; Springer: Cham, Switzerland, 2018; pp. 265–291. [Google Scholar]
- Farvolden, P.; Cunningham, J.; Selby, P. Using E-Health Programs to Overcome Barriers to the Effective Treatment of Mental Health and Addiction Problems. J. Technol. Hum. Serv. 2009, 27, 5–22. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Eaton, W.W. Internet-Based Mental Health Interventions. Ment. Health Serv. Res. 2005, 7, 75–87. [Google Scholar] [CrossRef]
- mHealth: New Horizons for Health through Mobile Technologies. 2011. Available online: http://www.who.int/goe/publications/goe_mhealth_web.pdf (accessed on 1 September 2020).
- Kodama, T.; Syouji, H.; Takaki, S.; Fujimoto, H.; Ishikawa, S.; Fukutake, M.; Taira, M.; Hashimoto, T. Text Messaging for Psychiatric Outpatients: Effect on Help-Seeking and Self-Harming Behaviors. J. Psychosoc. Nurs. Ment. Health Serv. 2016, 54, 31–37. [Google Scholar] [CrossRef]
- Yao, P.; Fu, R.; Craig Rushing, S.; Stephens, D.; Ash, J.S.; Eden, K.B. Texting 4 Sexual Health: Improving Attitudes, Intention, and Behavior among American Indian and Alaska Native Youth. Health Promot. Pract. 2018, 19, 833–843. [Google Scholar] [CrossRef]
- Watson, N.L.; Mull, K.E.; Heffner, J.L.; McClure, J.B.; Bricker, J.B. Participant recruitment and retention in remote eHealth intervention trials: Methods and lessons learned from a large randomized controlled trial of two web-based smoking interventions. J. Med. Internet Res. 2018, 20, e10351. [Google Scholar] [CrossRef]
- Shrestha, U.; Hanson, J.; Weber, T.; Ingersoll, K. Community Perceptions of Alcohol Exposed Pregnancy Prevention Program for American Indian and Alaska Native Teens. Int. J. Environ. Res. Public Health 2019, 16, 1795. [Google Scholar] [CrossRef]
- Chapter 45. Social Marketing of Successful Components of the Initiative. Available online: http://ctb.ku.edu/en/table-of-contents/sustain/social-marketing (accessed on 1 September 2020).
- Kreuter, M.W.; Oswald, D.L.; Bull, F.C.; Clark, E.M. Are Tailored Health Education Materials always More Effective than Non-tailored Materials? Health Educ. Res. 2000, 15, 305–315. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Lukwago, S.N.; Bucholtz, R.D.; Clark, E.M.; Sanders-Thompson, V. Achieving Cultural Appropriateness in Health Promotion Programs: Targeted and Tailored Approaches. Health Educ. Behav. 2003, 30, 133–146. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Sugg-Skinner, C.; Holt, C.L.; Clark, E.M.; Haire-Joshu, D.; Fu, Q.; Booker, A.C.; Steger-May, K.; Bucholtz, D. Cultural tailoring for Mammography and Fruit and Vegetable Intake among Low-income African-American Women in Urban Public Health Centers. Prev. Med. 2005, 41, 53–62. [Google Scholar] [CrossRef]
- Ito, K.E.; Kalyanaraman, S.; Ford, C.A.; Brown, J.D.; Miller, W.C. “Let’s talk about sex”: Pilot study of an interactive CD–ROM to prevent HIV/STIs in female adolescents. AIDS Educ. Prev. 2008, 20, 78–89. [Google Scholar] [CrossRef]
- Rushing, S.C.; Stephens, D. Tribal recommendations for designing culturally appropriate technology-based sexual health interventions targeting Native youth in the Pacific Northwest. Am. Indian Alsk. Nativ. Ment. Health Res. J. Natl. Cent. 2012, 19, 76–101. [Google Scholar] [CrossRef]
- Devine, S.; Leeds, C.; Shlay, J.C.; Leytem, A.; Beum, R.; Bull, S. Methods to assess youth engagement in a text messaging supplement to an effective teen pregnancy program. J. Biomed. Inform. 2015, 56, 379–386. [Google Scholar] [CrossRef]
- Most U.S. Teens Who Use Cellphones Do it to Pass Time, Connect with Others, Learn New Things. Available online: https://www.pewresearch.org/fact-tank/2019/08/23/most-u-s-teens-who-use-cellphones-do-it-to-pass-time-connect-with-others-learn-new-things/ (accessed on 24 October 2020).


{kind=link}
| BRAVE Arm Messages—Week 2 | STEM Arm Messages—Week 2 |
|---|---|
| Sunday Hi! I’m Alex. I’ve been through a lot this year—parties, girl drama, rez life. To really get to know me, you should see where I grew up. Watch this video to learn more about me: Alex—Episode 1 (https://www.youtube.com/watch?v=pPBI8oUXZ8Q) Follow-up Text: As you can see, my dad taught me everything I know—the good and the bad. My dad’s drinking, the arguments that would follow… I thought those things were normal. | Sunday [Emojis—OK, Sunglasses, Pointing Left; $ signs Face] Cool? Wanna make some $? The Bureau of Labor predicts a 27% growth in IT jobs by 2024... Web development and computer science are ideal jobs in rural (and urban) communities. People who can do the work are highly sought after and well paid, and you can often work remotely. You can even use coding skills to help preserve Native languages: https://www.youtube.com/watch?v=pPBI8oUXZ8Q Follow-up Text: We’re descended from scientists, inventors, and innovators. Imagine bridging the digital divide in native communities!? Learn tech to continue our traditions. |
| Ad Name | Impressions |
|---|---|
| FB Post: “We Need Your Help! We R Native is recruiting…” | 12,982 |
| FB Post: “🤳 Text BRAVE to 97779” | 12,766 |
| Instagram Post: An Auntie’s hug and laugh… | 114,713 |
| Instagram Post: Are you a Native teen or young… | 124,492 |
| Instagram Post: How can we help our friends who… | 68,876 |
| Platform/Ad Type | Text Example | Impressions | Link Clicks | Conversion Rate (%) | Ad Costs (US$) | Cost per Link Click (US$) |
|---|---|---|---|---|---|---|
| Instagram Link Clicks | I am building a better world for… | 550,880 | 353,150 | 0.64 | $2606 | $2.69 |
| Facebook Post Link Clicks | We Need Your Help! We R Native is recruiting… | 25,748 | 12,020 | 0.46 | $119 | $0.65 |
| Facebook Post Engagement | I am building a better world for our people… | 188,550 | 111,081 | 0.58 | $1906 | $0.12 |
| Facebook ThruPlay | Abuse isn’t always physical. Abuse can come in… | 152,047 | 91,511 | 0.60 | $510 | $0.05 |
| Total | 917,225 | 567,762 | $5141 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stephens, D.; Peterson, R.; Singer, M.; Johnson, J.; Rushing, S.C.; Kelley, A. Recruiting and Engaging American Indian and Alaska Native Teens and Young Adults in a SMS Help-Seeking Intervention: Lessons Learned from the BRAVE Study. Int. J. Environ. Res. Public Health 2020, 17, 9437. https://doi.org/10.3390/ijerph17249437
Stephens D, Peterson R, Singer M, Johnson J, Rushing SC, Kelley A. Recruiting and Engaging American Indian and Alaska Native Teens and Young Adults in a SMS Help-Seeking Intervention: Lessons Learned from the BRAVE Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9437. https://doi.org/10.3390/ijerph17249437
Chicago/Turabian StyleStephens, David, Roger Peterson, Michelle Singer, Jacqueline Johnson, Stephanie Craig Rushing, and Allyson Kelley. 2020. "Recruiting and Engaging American Indian and Alaska Native Teens and Young Adults in a SMS Help-Seeking Intervention: Lessons Learned from the BRAVE Study" International Journal of Environmental Research and Public Health 17, no. 24: 9437. https://doi.org/10.3390/ijerph17249437
APA StyleStephens, D., Peterson, R., Singer, M., Johnson, J., Rushing, S. C., & Kelley, A. (2020). Recruiting and Engaging American Indian and Alaska Native Teens and Young Adults in a SMS Help-Seeking Intervention: Lessons Learned from the BRAVE Study. International Journal of Environmental Research and Public Health, 17(24), 9437. https://doi.org/10.3390/ijerph17249437