Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
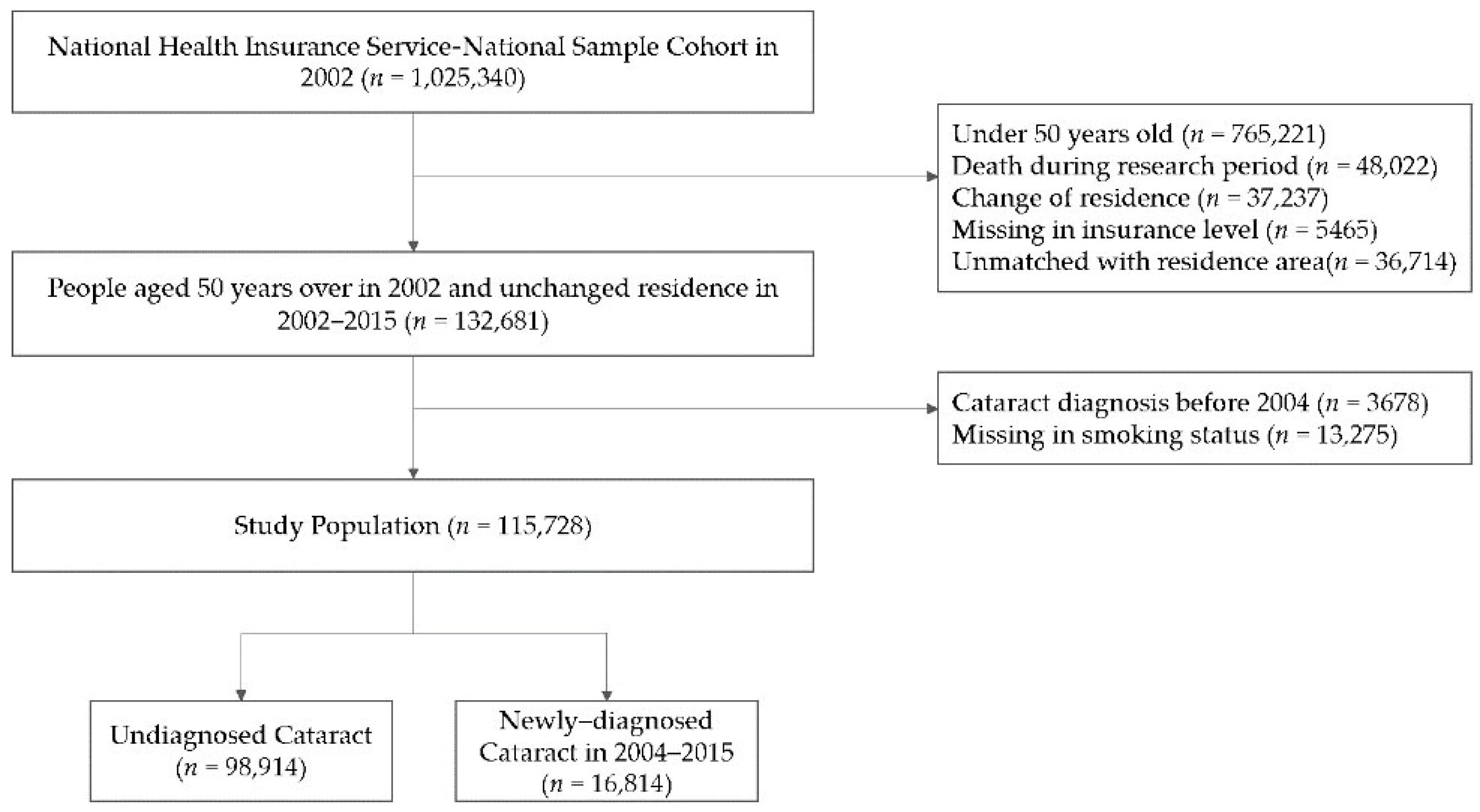
2.2. Study Participants
2.3. Air Pollutant Variables
2.4. Other Variables
2.5. Statistical Analyses
3. Results
3.1. Demographic Characteristics
3.2. Association of Newly Developed Cataract and Air Pollutants
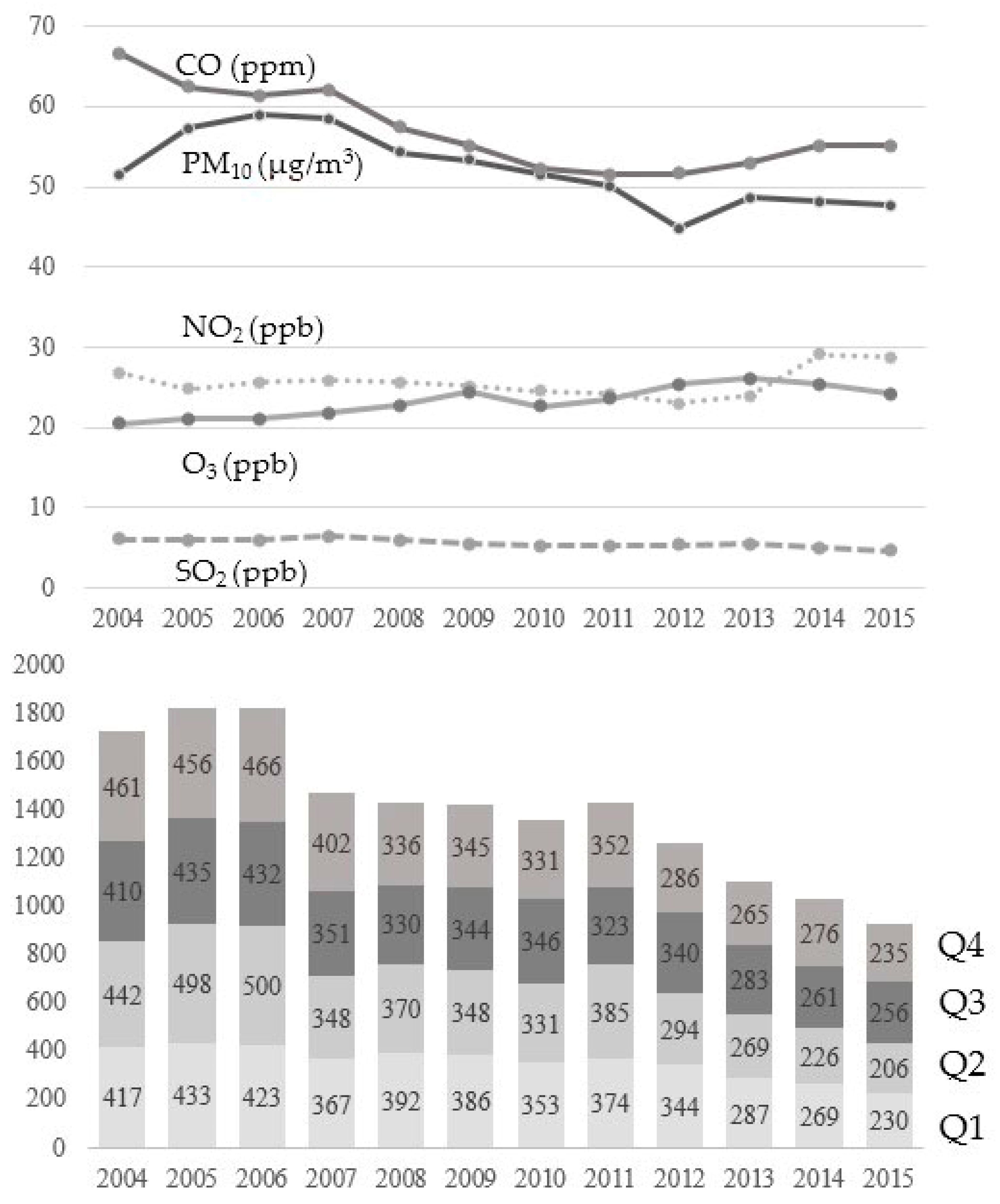
3.3. The Annual Trends of Mean Concentration of Air Pollutants and Number of Diagnosed Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Asbell, P.A.; Dualan, I.; Mindel, J.; Brocks, D.; Ahmad, M.; Epstein, S. Age-related cataract. Lancet 2005, 365, 599–609. [Google Scholar] [CrossRef]
- Apple, D.J.; Ram, J.; Foster, A.; Peng, Q. Cataract: Epidemiology and Service Delivery. Surv. Ophthalmol. 2000, 45, S32–S44. [Google Scholar] [CrossRef]
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Global Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef]
- Lee, C.M.; Afshari, N.A. The global state of cataract blindness. Curr. Opin. Ophthalmol. 2017, 28, 98–103. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service. Statistic for Common Disease in South Korea. Available online: http://opendata.hira.or.kr/op/opc/olapHifrqSickInfo.do (accessed on 14 October 2020).
- Mimura, T.; Ichinose, T.; Yamagami, S.; Fujishima, H.; Kamei, Y.; Goto, M.; Takada, S.; Matsubara, M. Airborne particulate matter (PM2.5) and the prevalence of allergic conjunctivitis in Japan. Sci. Total Environ. 2014, 487, 493–499. [Google Scholar] [CrossRef]
- Zhong, J.Y.; Lee, Y.C.; Hsieh, C.J.; Tseng, C.C.; Yiin, L.M. Association between Dry Eye Disease, Air Pollution and Weather Changes in Taiwan. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef]
- Um, S.B.; Kim, N.H.; Lee, H.K.; Song, J.S.; Kim, H.C. Spatial epidemiology of dry eye disease: Findings from South Korea. Int. J. Health Geogr. 2014, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.H.; Hsu, P.Y.; Lin, C.J.; Lin, C.L.; Juo, S.H.; Liang, C.L. Traffic-related air pollutants increase the risk for age-related macular degeneration. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2019, 67, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Ravilla, T.D.; Gupta, S.; Ravindran, R.D.; Vashist, P.; Krishnan, T.; Maraini, G.; Chakravarthy, U.; Fletcher, A.E. Use of Cooking Fuels and Cataract in a Population-Based Study: The India Eye Disease Study. Environ. Health Perspect. 2016, 124, 1857–1862. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Schaumberg, D.A.; Park, S.K. Cadmium and lead exposure and risk of cataract surgery in U.S. adults. Int. J. Hyg. Environ. Health 2016, 219, 850–856. [Google Scholar] [CrossRef]
- Choi, Y.H.; Park, S.J.; Paik, H.J.; Kim, M.K.; Wee, W.R.; Kim, D.H. Unexpected potential protective associations between outdoor air pollution and cataracts. Environ. Sci. Pollut. Res. Int. 2018, 25, 10636–10643. [Google Scholar] [CrossRef] [PubMed]
- Hammond, C.J.; Duncan, D.D.; Snieder, H.; de Lange, M.; West, S.K.; Spector, T.D.; Gilbert, C.E. The heritability of age-related cortical cataract: The twin eye study. Investig. Ophthalmol. Vis. Sci. 2001, 42, 601–605. [Google Scholar]
- Nam, G.E.; Han, K.; Ha, S.G.; Han, B.D.; Kim, D.H.; Kim, Y.H.; Cho, K.H.; Park, Y.G.; Ko, B.J. Relationship between socioeconomic and lifestyle factors and cataracts in Koreans: The Korea National Health and Nutrition Examination Survey 2008–2011. Eye 2015, 29, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Han, S.H.; Choi, J. Exposure to Ambient Air Pollution and Cognitive Impairment in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Kang, D.; Lee, H.; Shin, S.H.; Kang, M.; Kong, S.; Rhee, C.K.; Cho, J.; Yoo, K.H. Impact of chronic obstructive pulmonary disease on mortality: A large national cohort study. Respirology 2020, 25, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- D’Hoore, W.; Sicotte, C.; Tilquin, C. Risk adjustment in outcome assessment: The Charlson comorbidity index. Methods Inf. Med. 1993, 32, 382–387. [Google Scholar]
- Lou, L.; Ye, X.; Xu, P.; Wang, J.; Xu, Y.; Jin, K.; Ye, J. Association of Sex With the Global Burden of Cataract. JAMA Ophthalmol. 2018, 136, 116–121. [Google Scholar] [CrossRef]
- Periyasamy, P.; Shinohara, T. Age-related cataracts: Role of unfolded protein response, Ca2+ mobilization, epigenetic DNA modifications, and loss of Nrf2/Keap1 dependent cytoprotection. Prog. Retin. Eye Res. 2017, 60, 1–19. [Google Scholar] [CrossRef]
- Truscott, R.J. Human cataract: The mechanisms responsible; light and butterfly eyes. Int. J. Biochem. Cell Biol. 2003, 35, 1500–1504. [Google Scholar] [CrossRef]
- Beebe, D.C.; Holekamp, N.M.; Shui, Y.-B. Oxidative damage and the prevention of age-related cataracts. Ophthalmic. Res. 2010, 44, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Elminir, H.K. Sensitivity of ultraviolet solar radiation to anthropogenic air pollutants and weather conditions. Atmos. Res. 2007, 84, 250–264. [Google Scholar] [CrossRef]
- Zegarska, B.; Pietkun, K.; Zegarski, W.; Bolibok, P.; Wiśniewski, M.; Roszek, K.; Czarnecka, J.; Nowacki, M. Air pollution, UV irradiation and skin carcinogenesis: What we know, where we stand and what is likely to happen in the future? Postepy Dermatol. Alergol. 2017, 34, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Ryou, H.g.; Heo, J.; Kim, S.-Y. Source apportionment of PM10 and PM2.5 air pollution, and possible impacts of study characteristics in South Korea. Environ. Pollut. 2018, 240, 963–972. [Google Scholar] [CrossRef]
- Tang, Y.; Ji, Y.; Ye, X.; Wang, X.; Cai, L.; Xu, J.; Lu, Y. The Association of Outdoor Activity and Age-Related Cataract in a Rural Population of Taizhou Eye Study: Phase 1 Report. PLoS ONE 2015, 10, e0135870. [Google Scholar] [CrossRef]
- Lindblad, B.E.; Håkansson, N.; Philipson, B.; Wolk, A. Hormone replacement therapy in relation to risk of cataract extraction: A prospective study of women. Ophthalmology 2010, 117, 424–430. [Google Scholar] [CrossRef]
- Lee, H.; Kim, E.K.; Kim, H.Y.; Kim, T.-I. Effects of Exposure to Ozone on the Ocular Surface in an Experimental Model of Allergic Conjunctivitis. PLoS ONE 2017, 12, e0169209. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, Y.H.; Kim, M.K.; Paik, H.J.; Kim, D.H. Different adverse effects of air pollutants on dry eye disease: Ozone, PM2.5, and PM10. Environ. Pollut. 2020, 265, 115039. [Google Scholar] [CrossRef]
- Air Quality Guidelines, Global Update. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/78638/E90038.pdf (accessed on 4 October 2020).
- Hwang, S.H.; Choi, Y.H.; Paik, H.J.; Wee, W.R.; Kim, M.K.; Kim, D.H. Potential Importance of Ozone in the Association Between Outdoor Air Pollution and Dry Eye Disease in South Korea. JAMA Ophthalmol. 2016, 134, 503–510. [Google Scholar] [CrossRef]
- Kim, R.; Yoo, D.; Jung, Y.J.; Han, K.; Lee, J.Y. Sex differences in smoking, alcohol consumption, and risk of Parkinson’s disease: A nationwide cohort study. Parkinsonism Relat. Disord. 2020, 71, 60–65. [Google Scholar] [CrossRef]
- Wang, W.; Yan, W.; Fotis, K.; Prasad, N.M.; Lansingh, V.C.; Taylor, H.R.; Finger, R.P.; Facciolo, D.; He, M. Cataract Surgical Rate and Socioeconomics: A Global Study. Investig. Ophthalmol. Visual Sci. 2016, 57, 5872–5881. [Google Scholar] [CrossRef] [PubMed]
- Adamkiewicz, G.; Liddie, J.; Gaffin, J.M. The Respiratory Risks of Ambient/Outdoor Air Pollution. Clin. Chest Med. 2020, 41, 809–824. [Google Scholar] [CrossRef] [PubMed]
- Vimercati, L.; Cavone, D.; Caputi, A.; Delfino, M.C.; De Maria, L.; Ferri, G.M.; Serio, G. Malignant mesothelioma in construction workers: The Apulia regional mesothelioma register, Southern Italy. BMC Res. Notes 2019, 12, 636. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 115,728) | No Cataract (n = 98,914) | Cataract (n = 16,814) | p-Value | |
|---|---|---|---|---|
| Age, year | 60.0 ± 7.2 | 59.4 ± 7.5 | 63.2 ± 6.9 | <0.001 |
| Sex | <0.001 | |||
| Male | 54,679 (47.2) | 48,395 (88.5) | 6284 (11.5) | |
| Female | 61,049 (52.8) | 50,519 (82.8) | 10,530 (17.2) | |
| Smoking status | <0.001 | |||
| Non-smoker | 86,453 (74.7) | 72,860 (84.3) | 13,593 (15.7) | |
| Former smoker | 9663 (8.4) | 8429 (87.2) | 1234 (12.8) | |
| Current smoker | 19,612 (16.9) | 17,625 (89.9) | 1987 (10.1) | |
| Insurance levels | <0.001 | |||
| Lower | 45,884 (39.6) | 39,319 (85.7) | 6565 (14.3) | |
| Upper | 69,844 (60.4) | 59,595 (85.3) | 10,249 (14.7) | |
| Urbanization | <0.001 | |||
| High | 50,207 (43.4) | 43,382 (86.4) | 6825 (13.6) | |
| Less | 65,521 (56.6) | 55,532 (84.8) | 9989 (15.2) | |
| Comorbidity | ||||
| Diabetes mellitus | 22,314 (19.3) | 17,734 (17.9) | 4580 (27.2) | <0.001 |
| Cerebrovascular disease | 4360 (3.8) | 4200 (4.2) | 1060 (6.3) | <0.001 |
| Peripheral vascular disease | 4203 (3.6) | 3347 (3.4) | 856 (5.1) | <0.001 |
| Chronic pulmonary disease | 2712 (2.3) | 2172 (2.2) | 540 (3.2) | <0.001 |
| Mental disorder | 2243 (1.9) | 1776 (1.8) | 467 (2.8) | <0.001 |
| Congestive heart failure | 1449 (1.3) | 1153 (1.2) | 296 (1.8) | <0.001 |
| Myocardial infarction | 599 (0.52) | 500 (0.51) | 99 (0.59) | <0.001 |
| Malignancy | 550 (0.48) | 475 (0.48) | 75 (0.45) | 0.516 |
| Hemiplegia | 533 (0.46) | 454 (0.46) | 79 (0.47) | 0.848 |
| Liver disease | 409 (0.36) | 330 (0.33) | 79 (0.47) | 0.526 |
| Chronic kidney disease | 314 (0.27) | 254 (0.26) | 60 (0.36) | 0.021 |
| Total (n = 115,728) | Male (n = 54,679) | Female (n = 61,049) | <65 Years Old (n = 101,372) | ≥65 Years Old (n = 14,356) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted HR | 95% CI | p Value for Trend | Adjusted HR | 95% CI | p Value for Trend | Adjusted HR | 95% CI | p Value for Trend | Adjusted HR | 95% CI | p Value for Trend | Adjusted HR | 95% CI | p Value for Trend | |||||||
| PM10 | Q1 | 1 | <0.001 | 1 | 0.028 | 1 | <0.001 | 1 | 0.106 | 1 | <0.001 | ||||||||||
| Q2 | 1.071 | 1.026 | 1.118 | 1.076 | 1.004 | 1.154 | 1.068 | 1.012 | 1.127 | 1.011 | 0.954 | 1.070 | 1.129 | 1.059 | 1.203 | ||||||
| Q3 | 0.992 | 0.951 | 1.036 | 1.016 | 0.947 | 1.089 | 0.980 | 0.928 | 1.035 | 0.946 | 0.894 | 1.010 | 1.031 | 0.966 | 1.101 | ||||||
| Q4 | 1.069 | 1.025 | 1.115 | 1.094 | 1.021 | 1.173 | 1.058 | 1.004 | 1.116 | 0.998 | 0.943 | 1.055 | 1.143 | 1.071 | 1.218 | ||||||
| PM2.5 | Q1 | 1 | 0.547 | 1 | 0.891 | 1 | 0.646 | 1 | 0.475 | 1 | 0.437 | ||||||||||
| Q2 | 1.012 | 0.833 | 1.230 | 0.934 | 0.679 | 1.284 | 1.039 | 0.810 | 1.314 | 0.907 | 0.720 | 1.142 | 1.387 | 0.939 | 2.049 | ||||||
| Q3 | 0.927 | 0.760 | 1.130 | 1.001 | 0.752 | 1.333 | 0.866 | 0.657 | 1.141 | 0.883 | 0.706 | 1.105 | 1.127 | 0.719 | 1.766 | ||||||
| Q4 | 0.905 | 0.772 | 1.062 | 0.917 | 0.717 | 1.784 | 0.903 | 0.731 | 1.115 | 0.873 | 0.724 | 1.054 | 1.079 | 0.791 | 1.471 | ||||||
| NO2 | Q1 | 1 | 0.011 | 1 | 0.122 | 1 | 0.001 | 1 | 0.699 | 1 | 0.004 | ||||||||||
| Q2 | 1.035 | 0.993 | 1.079 | 1.053 | 0.984 | 1.128 | 1.026 | 0.974 | 1.085 | 1.025 | 0.969 | 1.084 | 1.043 | 0.981 | 1.108 | ||||||
| Q3 | 1.062 | 1.015 | 1.112 | 1.070 | 0.993 | 1.153 | 1.059 | 1.000 | 1.122 | 1.029 | 0.969 | 1.093 | 1.102 | 1.027 | 1.181 | ||||||
| Q4 | 1.080 | 1.030 | 1.133 | 1.097 | 1.014 | 1.186 | 1.072 | 1.009 | 1.139 | 1.036 | 0.973 | 1.103 | 1.137 | 1.056 | 1.224 | ||||||
| SO2 | Q1 | 1 | 0.026 | 1 | 0.732 | 1 | 0.031 | 1 | 0.332 | 1 | 0.025 | ||||||||||
| Q2 | 1.065 | 1.021 | 1.111 | 1.010 | 0.942 | 1.083 | 1.102 | 1.044 | 1.162 | 1.044 | 0.986 | 1.106 | 1.086 | 1.019 | 1.157 | ||||||
| Q3 | 1.046 | 1.002 | 1.091 | 1.033 | 0.964 | 1.108 | 1.055 | 0.999 | 1.113 | 1.004 | 0.949 | 1.063 | 1.090 | 1.022 | 1.163 | ||||||
| Q4 | 1.027 | 0.984 | 1.073 | 1.035 | 0.963 | 1.112 | 1.026 | 0.971 | 1.083 | 0.993 | 0.937 | 1.052 | 1.067 | 0.998 | 1.141 | ||||||
| CO | Q1 | 1 | 0.064 | 1 | 0.286 | 1 | 0.033 | 1 | 0.409 | 1 | 0.091 | ||||||||||
| Q2 | 1.006 | 0.964 | 1.049 | 0.946 | 0.882 | 1.014 | 1.043 | 0.989 | 1.100 | 1.000 | 0.946 | 1.058 | 1.013 | 0.949 | 1.080 | ||||||
| Q3 | 1.047 | 1.004 | 1.093 | 1.007 | 0.939 | 1.079 | 1.072 | 1.015 | 1.132 | 1.043 | 0.986 | 1.104 | 1.057 | 0.989 | 1.129 | ||||||
| Q4 | 0.991 | 0.949 | 1.035 | 0.979 | 0.911 | 1.051 | 1.001 | 0.948 | 1.057 | 1.016 | 0.959 | 1.076 | 0.969 | 0.907 | 1.036 | ||||||
| O3 | Q1 | 1 | 0.013 | 1 | 0.199 | 1 | 0.022 | 1 | 0.226 | 1 | 0.017 | ||||||||||
| Q2 | 0.991 | 0.947 | 1.038 | 0.997 | 0.927 | 1.074 | 0.990 | 0.933 | 1.049 | 0.993 | 0.935 | 1.053 | 0.989 | 0.921 | 1.063 | ||||||
| Q3 | 0.997 | 0.953 | 1.044 | 1.000 | 0.928 | 1.077 | 0.998 | 0.941 | 1.058 | 1.007 | 0.948 | 1.069 | 0.984 | 0.916 | 1.057 | ||||||
| Q4 | 0.931 | 0.888 | 0.977 | 0.936 | 0.866 | 1.012 | 0.928 | 0.874 | 0.986 | 0.952 | 0.893 | 1.014 | 0.908 | 0.844 | 0.977 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.; Lee, H.; Kim, H. Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 9231. https://doi.org/10.3390/ijerph17249231
Shin J, Lee H, Kim H. Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9231. https://doi.org/10.3390/ijerph17249231
Chicago/Turabian StyleShin, Jinyoung, Hyungwoo Lee, and Hyeongsu Kim. 2020. "Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 24: 9231. https://doi.org/10.3390/ijerph17249231
APA StyleShin, J., Lee, H., & Kim, H. (2020). Association between Exposure to Ambient Air Pollution and Age-Related Cataract: A Nationwide Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 17(24), 9231. https://doi.org/10.3390/ijerph17249231