Two-Phase Evaluation of a Community-Based Lifestyle Intervention for Palestinian Women in East Jerusalem: A Quasi-Experimental Study Followed by Dissemination

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Statistical Analysis
3. Results
3.1. Quasi-Experiment
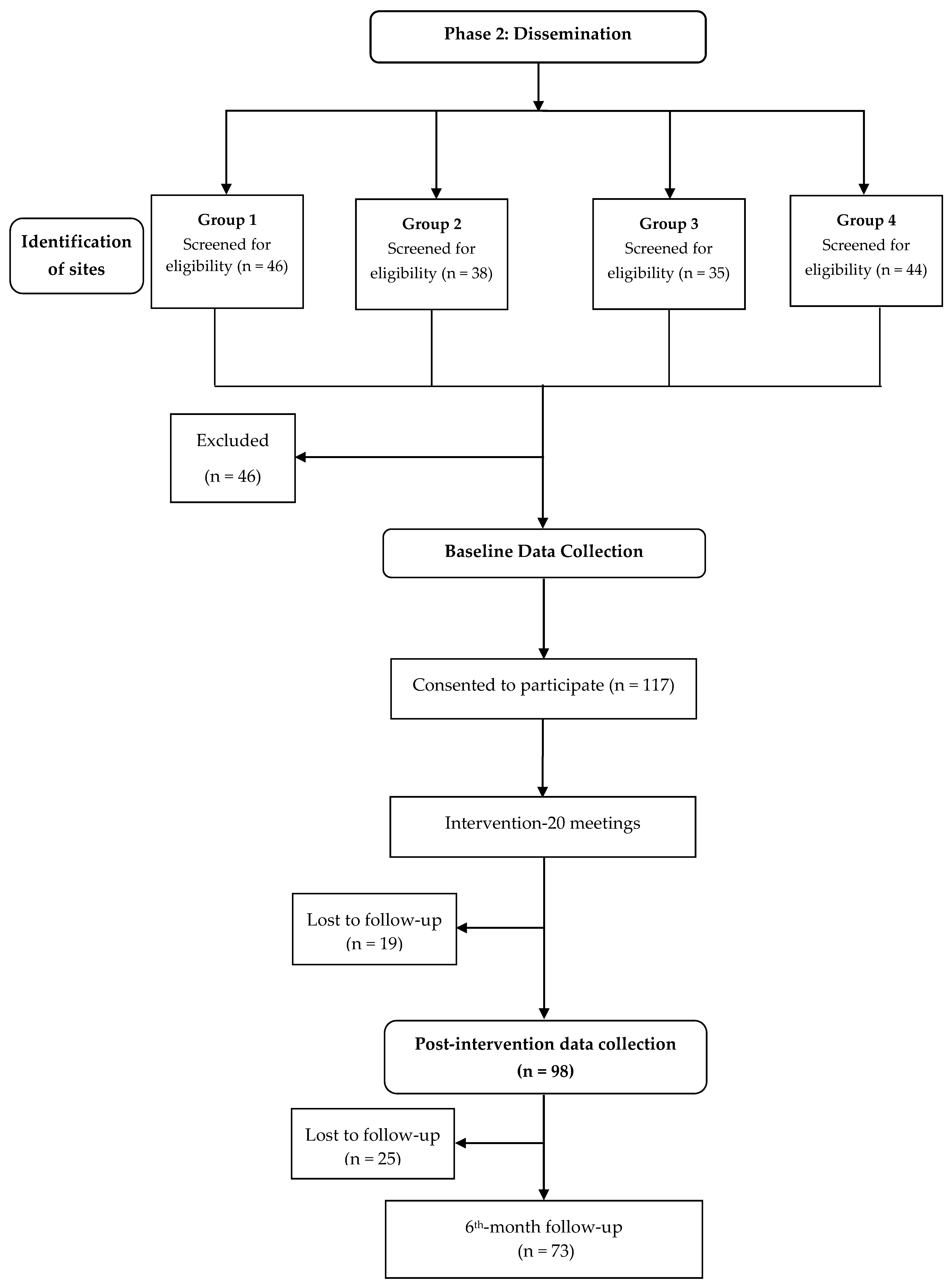
3.2. Dissemination Phase
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rahim, H.F.; Sibai, A.; Khader, Y.; Hwalla, N.; Fadhil, I.; Alsiyabi, H.; Mataria, A.; Mendis, S.; Mokdad, A.H.; Husseini, A. Non-communicable diseases in the Arab world. Lancet 2014, 383, 356–367. [Google Scholar] [CrossRef]
- Badran, M.; Laher, I. Type II Diabetes Mellitus in Arabic-Speaking Countries. Int. J. Endocrinol. 2012, 2012, 902873. [Google Scholar] [CrossRef] [PubMed]
- Kark, J.D.; Fink, R.; Adler, B.; Goldberger, N.; Goldman, S. The incidence of coronary heart disease among Palestinians and Israelis in Jerusalem. Int. J. Endocrinol. 2006, 35, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Shadmi, E. Healthcare disparities amongst vulnerable populations of Arabs and Jews in Israel. Isr. J. Health Policy Res. 2018, 7, 26. [Google Scholar] [CrossRef]
- Kalter-Leibovici, O.; Atamna, A.; Lubin, F.; Alpert, G.; Keren, M.G.; Murad, H.; Chetrit, A.; Goffer, D.; Eilat-Adar, S.; Goldbourt, U. Obesity among Arabs and Jews in Israel: A population-based study. IMAJ-RAMAT GAN- 2007, 9, 525. [Google Scholar]
- Bayram, T.; Donchin, M. Determinants of health behavior inequalities: A cross-sectional study from Israel. Health Promot. Int. 2019, 34, 941–952. [Google Scholar] [CrossRef]
- Tirosh, A.; Calderon-Margalit, R.; Mazar, M.; Stern, Z. Differences in Quality of Diabetes Care Between Jews and Arabs in Jerusalem. Am. J. Med. Qual. 2008, 23, 60–65. [Google Scholar] [CrossRef]
- Khaw, K.-T.; Wareham, N.; Bingham, S.; Welch, A.; Luben, R.; Day, N. Combined Impact of Health Behaviours and Mortality in Men and Women: The EPIC-Norfolk Prospective Population Study. PLoS Med. 2008, 5, e12. [Google Scholar]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; Report No.: 9241506237; WHO Document Production Services: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. The Protocol for the WHO Study on the Effectiveness of Community-Based Programmes for NCD Prevention and Control; Report No.: NMH/NPH/NCP/03.09; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Lawlor, E.R.; Bradley, D.T.; Cupples, M.E.; Tully, M.A. The effect of community-based interventions for cardiovascular disease secondary prevention on behavioural risk factors. Prev. Med. 2018, 114, 24–38. [Google Scholar] [CrossRef]
- Ashra, N.B.; Spong, R.; Carter, P.; Davies, M.J.; Dunkley, A.; Gillies, C.; Greaves, C.; Khunti, K.; Sutton, S.; Yates, T. A Systematic Review and Meta-Analysis Assessing the Effectiveness of Pragmatic Lifestyle Interventions for the Prevention of Type 2 Diabetes Mellitus in Routine Practice; Public Health England: London, UK, 2015. [Google Scholar]
- Sisti, L.G.; Dajko, M.; Campanella, P.; Shkurti, E.; Ricciardi, W.; de Waure, C. The effect of multifactorial lifestyle interventions on cardiovascular risk factors: A systematic review and meta-analysis of trials conducted in the general population and high risk groups. Prev. Med. 2018, 109, 82–97. [Google Scholar] [CrossRef]
- DPP Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef]
- Neamah, H.H.; Sebert Kuhlmann, A.K.; Tabak, R.G. Effectiveness of Program Modification Strategies of the Diabetes Prevention Program: A Systematic Review. Diabetes Educ. 2016, 42, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Qu, S.; Zhang, P.; Chattopadhyay, S.K.; Gregg, E.W.; Albright, A.; Hopkins, D.; Pronk, N.P. Economic Evaluation of Combined Diet and Physical Activity Promotion Programs to Prevent Type 2 Diabetes Among Persons at Increased Risk: A Systematic Review for the Community Preventive Services Task Force. Ann. Intern. Med. 2015, 163, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Mabry, R.M.; Koohsari, M.J.; Bull, F.; Owen, N. A systematic review of physical activity and sedentary behaviour research in the oil-producing countries of the Arabian Peninsula. BMC Public Health 2016, 16, 1003. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Prevention Program Research Group. DPP Lifestyle Materials for Sessions 1–16—Lifestyle Coach Materials and Optional Participant Handouts. Available online: https://dppos.bsc.gwu.edu/web/dppos/lifestyle-handouts (accessed on 2 March 2016).
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Stefanadis, C. Association between the prevalence of obesity and adherence to the Mediterranean diet: The ATTICA study. Nutrition 2006, 22, 449–456. [Google Scholar] [CrossRef]
- Hu, F.B.; Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Spiegelman, D.; Willett, W.C. Prospective study of major dietary patterns and risk of coronary heart disease in men. Am. J. Clin. Nutr. 2000, 72, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.A.H.; Wallentin, L.; Benatar, J.; Danchin, N.; Hagström, E.; Held, C.; Husted, S.; Lonn, E.; Stebbins, A.; Chiswell, K.; et al. Dietary patterns and the risk of major adverse cardiovascular events in a global study of high-risk patients with stable coronary heart disease. Eur. Heart J. 2016, 37, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, E.A.; Barreira, T.V.; Kang, M. Validity and reliability of Omron pedometers for prescribed and self-paced walking. Med. Sci. Sports Exerc. 2009, 41, 670–674. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Cook, N.R.; Shay, C.M.; Rexrode, K.M.; Albert, C.M.; Manson, J.E.; Willett, W.C.; Rimm, E.B. Lifestyle-based prediction model for the prevention of CVD: The Healthy Heart Score. J. Am. Heart Assoc. 2014, 3, e000954. [Google Scholar] [CrossRef]
- Ziegler, A.; Kastner, C.; Blettner, M. The generalised estimating equations: An annotated bibliography. Biom. J. J. Math. Methods Biosci. 1998, 40, 115–139. [Google Scholar] [CrossRef]
- Fitzmaurice, G.; Davidian, M.; Verbeke, G.; Molenberghs, G. Longitudinal Data Analysis; Chapman and Hall/CRC: New York, NY, USA, 2009; pp. 45–56. [Google Scholar]
- Jaffe, A.; Giveon, S.; Wulffhart, L.; Oberman, B.; Baidousi, M.; Ziv, A.; Kalter-Leibovici, O. Adult Arabs have higher risk for diabetes mellitus than Jews in Israel. PLoS ONE 2017, 12, e0176661. [Google Scholar] [CrossRef] [PubMed]
- Kalter-Leibovici, O.; Younis-Zeidan, N.; Atamna, A.; Lubin, F.; Alpert, G.; Chetrit, A.; Novikov, I.; Daoud, N.; Freedman, L.S. Lifestyle intervention in obese Arab women: A randomized controlled trial. Arch. Intern. Med. 2010, 170, 970–976. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Al-Hamdan, R.; Avery, A.; Salter, A.M.; Al-Disi, D.; Al-Daghri, N.M.; McCullough, F. Identification of education models to improve health outcomes in arab women with pre-diabetes. Nutrients 2019, 11, 1113. [Google Scholar] [CrossRef] [PubMed]
- Wani, K.; A Alfawaz, H.; Alnaami, A.M.; Sabico, S.; Khattak, M.N.K.; Al-Attas, O.; Alokail, M.S.; Alharbi, M.; Chrousos, G.; Kumar, S. Effects of a 12-month intensive lifestyle monitoring program in predominantly overweight/obese Arab adults with prediabetes. Nutrients 2020, 12, 464. [Google Scholar] [CrossRef]
- Sadiya, A.; Abdi, S.; Abusnana, S. Lifestyle Intervention for Weight Loss: A group-based program for Emiratis in Ajman, United Arab Emirates. Diabetes Metab. Syndr. Obesity Targets Ther. 2016, 9, 101–108. [Google Scholar] [CrossRef]
- Dunkley, A.J.; Bodicoat, D.H.; Greaves, C.J.; Russell, C.; Yates, T.; Davies, M.J.; Khunti, K. Diabetes prevention in the real world: Effectiveness of pragmatic lifestyle interventions for the prevention of type 2 diabetes and of the impact of adherence to guideline recommendations: A systematic review and meta-analysis. Diabetes Care 2014, 37, 922–933. [Google Scholar] [CrossRef]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef]
- Afshin, A.; Babalola, D.; McLean, M.; Yu, Z.; Ma, W.; Chen, C.Y.; Arabi, M.; Mozaffarian, D. Information Technology and Lifestyle: A Systematic Evaluation of Internet and Mobile Interventions for Improving Diet, Physical Activity, Obesity, Tobacco, and Alcohol Use. J. Am. Heart Assoc. 2016, 5, e003058. [Google Scholar] [CrossRef]
- Franz, M.J.; VanWormer, J.J.; Crain, A.L.; Boucher, J.L.; Histon, T.; Caplan, W.; Bowman, J.D.; Pronk, N.P. Weight-Loss Outcomes: A Systematic Review and Meta-Analysis of Weight-Loss Clinical Trials with a Minimum 1-Year Follow-Up. J. Am. Diet. Assoc. 2007, 107, 1755–1767. [Google Scholar] [CrossRef]
- Sidani, S.; Ibrahim, S.; Lok, J.; Fan, L.; Fox, M.; Guruge, S. An integrated strategy for the cultural adaptation of evidence-based interventions. Health 2017, 9, 738. [Google Scholar] [CrossRef]
- Kearney, A.; Daykin, A.; Shaw, A.R.G.; Lane, A.J.; Blazeby, J.M.; Clarke, M.; Williamson, P.; Gamble, C. Identifying research priorities for effective retention strategies in clinical trials. Trials 2017, 18, 406. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Intervention (n = 38) | Comparison (n = 22) | 1p-Value |
|---|---|---|---|
| Age, Mean ± SD | 48.4 ± 12.7 | 57 ± 11.3 | 0.12 |
| Education level; n (%) | 0.08 | ||
| Elementary school | 9 (23.7%) | 10 (45.5%) | |
| High school | 22 (57.9%) | 8 (36.4%) | |
| Matriculation exam | 7 (18.5%) | 4 (18.6%) | |
| Marital status; n (%) | 0.006 | ||
| Married | 34 (89.5%) | 13 (59.1%) | |
| Other | 4 (10.5%) | 9 (40.9%) | |
| Parity, Mean (SD) | 5.3 (2.3) | 5.4 (2.1) | 0.923 |
| Employed n (%) | 6 (16.2%) | 1 (4.5%) | 0.24 |
| Self-reported HOD, n (%) | |||
| Hypertension | 4 (11.4%) | 13 (59.1%) | <0.001 |
| Hypercholesterolemia | 14 (40.0%) | 13 (59.1%) | 0.16 |
| Diabetes | 6 (16.2%) | 1 (4.5%) | 0.18 |
| Health behaviors: smoker, n (%) | 7 (18.9%) | 5 (22.7%) | 0.73 |
| BMI categories, n (%) | 0.13 | ||
| Normal | 6 (15.8%) | 0 | |
| Overweight | 14 (36.8%) | 11 (52.4%) | |
| Obese | 18 (47.4%) | 10 (47.6%) | |
| SBP, Mean (SD), mmHg | 129.6 (17.2) | 126.5 (13.7) | 0.466 |
| DBP, Mean (SD), mmHg | 77.2 (9.7) | 79.9 (11.1) | 0.333 |
| Time | Group | Time × Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dependent Variable | Wald c | Before | After | Wald | Control | Intervention | Wald | Control Before | Control After | Intervention Before | Intervention After |
| Average daily portions of: | |||||||||||
| Vegetables | 6.11 * | 1.25 a (0.16) | 2.01 b (0.26) | 0.05 | 1.60 a (0.22) | 1.66 a (0.19) | 2.64 ~ | 1.47 a (0.23) | 1.58 a (0.41) | 1.15 a (0.21) | 2.23 b (0.32) |
| Fruits | 6.02 * | 1.33 a (0.14) | 2.00 b (0.25) | 7.73 ** | 2.05 b (0.25) | 1.28 a (0.15) | 7.99 ** | 2.09 a (0.28) | 1.68 a (0.43) | 0.73 a (0.10) | 1.92 b (0.27) |
| Vegetables and fruits | 6.77 ** | 2.57 a (0.25) | 3.92 b (0.47) | 1.84 | 3.58 a (0.43) | 2.91 a (0.30) | 7.51 ** | 3.56 (0.42) | 3.14 (0.70) | 1.86 a (0.26) | 4.10 b (0.57) |
| Whole grains | 0.07 | 0.8 (0.13) | 0.85 (0.14) | 1.2 | 0.7 (0.11) | 0.93 (0.16) | 6.2 * | 0.9 a (0.15) | 0.4 b (0.08) | 0.8 a (0.2) | 1.1 a (0.22) |
| Average daily Steps | 21.34 *** | 4456 a (388) | 6404 b (557.3) | - | - | - | - | - | - | - | - |
| SBP (mmHG) | 8.80 ** | 128.82 b (2.07) | 121.71 a (2.23) | 0.45 | 126.48 a (2.89) | 124.05 a (2.15) | 21.17 *** | 126.5 a (2.86) | 130.05 a (3.22) | 129.66 b (2.76) | 117.06 a (2.48) |
| DBP (mmHG) | 4.33 * | 78.54 a (1.39) | 73.86 b (2.38) | 0.52 | 77.27 a (2.81) | 75.12 a (1.26) | 0.06 | 79.95 a (2.32) | 74.28 a (5.71) | 77.26 a (1.57) | 73.09 a (1.37) |
| SBP ≥ 140 (mmHG) c | 4.39 * | 0.22 b (0.06) | 0.09 a (0.06) | 0.29 | 0.16 a (0.08) | 0.12 a (0.04) | 1.68 | 0.23 a (0.09) | 0.17 a (0.09) | 0.21 a (0.07) | 0.04 a (0.04) |
| Weight (kg) | 9.47 ** | 79.66 b (1.96) | 78.64 a (1.95) | 0.30 | 80.21 a (2.99) | 78.08 a (2.50) | 2.26 | 80.42 a (3.01) | 80.44 a (2.98) | 78.74 a (2.52) | 77.34 a (2.50) |
| BMI | 10.18 ** | 31.19 b (0.69) | 30.78 a (0.68) | 0.13 | 31.23 a (0.98) | 30.73 a (0.95) | 2.11 | 31.32 a (1.00) | 31.30 a (0.96) | 30.99 a (0.96) | 30.44 a (0.95) |
| Variable | n = 117 |
|---|---|
| Age group n (%) | |
| <45 | 44 (37.9%) |
| 45–59 | 54 (46.6%) |
| 60+ | 18 (15.5%) |
| Education level: n (%) | |
| Elementary school | 14 (12.1%) |
| High school | 53 (45.7%) |
| Vocational training | 27 (23.3%) |
| Academic degree | 22 (19%) |
| Marital status; n (%) | |
| Married | 92 (79.3%) |
| Other | 24 (20.7%) |
| Parity, Mean (SD) | 4.18 (2.3%) |
| Participant’s employment | |
| Yes | 8 (7%) |
| No | 107 (93%) |
| Spouse employed | 77 (81.1%) |
| Self-reported HOD, n (%) | |
| Hypertension | 20 (17.1%) |
| Heart attack | 3 (2.6%) |
| Hypercholesterolemia | 39 (33.3%) |
| Diabetes | 22 (18.8%) |
| Weight, Mean (SD), kg | 77.9 (16.0%) |
| BMI categories: n (%) | |
| Normal | 18 (5.5%) |
| Overweight | 39 (33.6%) |
| Obese | 58 (50%) |
| SBP, Mean (SD), mmHg | 128.6 (20%) |
| DBP, Mean (SD), mmHg | 81 (14.8%) |
| Dependent Variable | Wald Chi-Square | Marginal Means | |||||
|---|---|---|---|---|---|---|---|
| Time | Group | Time × Group | Time 1 | Time 2 | Time 3 | Total | |
| Average daily portions of: | |||||||
| Vegetables | 12.01 ** | 11.06 ** | 11.01 * | 1.76 a (0.11) | 2.32 b (0.13) | 2.09 b (0.14) | 2.06 (0.08) |
| Fruit | 0.62 | 4.57 | 5.02 | 1.81 (0.12) | 1.91 (0.09) | 1.89 (0.12) | 1.87 (0.08) |
| Vegetables & Fruit | 7.30 * | 9.63 ** | 6.20 | 3.60 a (0.20) | 4.25 b (0.18) | 3.99 a b (0.22) | 3.95 (0.14) |
| Achieving the recommended ≥ 5 per day | 10.88 ** | 1.81 | 2.58 | 0.25 a (0.04) | 0.43 b (0.05) | 0.44 b (0.06) | 0.37 (0.03) |
| Whole grains | 1.33 | 31.4 *** | 11.97 * | 1.23 (0.12) | 1.38(0.10) | 1.32 (0.10) | 1.31 (0.07) |
| Sweetened drinks | 2.66 | 6.41 * | 22.46 *** | 2.66 | 0.65 (0.12) | 0.85 (0.17) | 0.54 (0.10) |
| Sweets | 9.48 ** | 1.20 | 17.82 ** | 9.48 ** | 1.48 a (0.13) | 1.03 b (0.11) | 1.20 (0.14) |
| Olive oil (tbl per week) | 0.41 | 5.59 * | 7.71 * | 4.68 (0.33) | 4.77 (0.43) | 4.98 (0.47) | 4.81 (0.29) |
| Average daily steps (ADS) | 63.69 *** | 14.99 ** | 1.36 | 4087.4 a (188.6) | 5284.2 b (234.4) | - | 4647.4 (196.6) |
| Participants increased their ADS > 4500 | 26.70 *** | 8.70 * | 0.50 | 0.36 a (0.05) | 0.64 b (0.05) | - | 0.50 (0.05) |
| PA moderate intensity | 22.78 *** | 1.75 | 4.92 | 97.82 a (13.21) | 191.32 b (19.97) | 183.95 b (28.40) | 151.00 (13.68) |
| PA vigorous intensity | 12.10 ** | 4.02 | 15.36 ** | 99.12 a (16.16) | 155.72 b (24.50) | 99.92 a (22.28) | 104.59 (15.27) |
| Achieving the recommended PA > 150 min/week | 24.17 *** | 0.04 | 8.07 | 0.33 a (0.05) | 0.64 b (0.05) | 0.53 b (0.6) | 0.50 (0.04) |
| SBP | 22.54 *** | 3.40 | 10.84 * | 128.15 b (1.88) | 121.34 a (1.66) | 119.01 a (2.12) | 122.77 (1.44) |
| DBS | 11.52 ** | 3.56 | 2.24 | 80.80 b (1.40) | 77.03 a (0.95) | 75.46 a (1.69) | 77.73 (1.00) |
| SBP ≥ 140 | 7.66 * | 0.85 | 6.49 | 0.27 b (0.04) | 0.19 b (0.04) | 0.08 a (0.05) | 0.16 (0.04) |
| Weight | 1.10 | 1.05 | 10.20 * | 77.52 (1.45) | 76.88 (1.41) | 76.81 (1.42) | 77.07 (1.38) |
| BMI | 1.64 | 0.18 | 11.60 * | 30.41 (0.52) | 30.11 (0.50) | 30.18 (0.52) | 30.24 (0.50) |
| HbA1C | 3.25 | 3.03 | 2.29 | 5.71 (0.10) | 5.67 (0.08) | 5.34 (0.22) | 5.57 (0.09) |
| Total cholesterol mg/dL | 7.91 ** | 0.51 | 0.80 | 187.07 b (3.05) | 176.33 a (3.81) | - | 181.62 (2.91) |
| HDL-mg/dL | 2.58 | 5.40 | 1.36 | 51.30 (1.49) | 47.98 (1.66) | - | 49.61 (1.20) |
| LDL-mg/dL | 7.49 ** | 2.47 | 1.36 | 111.55 b (2.84) | 97.58 a (4.22) | - | 104.33 (2.68) |
| TG-mg/dL | 0.45 | 0.54 | 9.09 * | 123.20 (5.97) | 118.36 (7.76) | - | 12.75 (5.94) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbaria, N.; Nubani-Husseini, M.; Barakat, R.A.; Leiter, E.; Greenberg, K.L.; Karjawally, M.; Keidar, O.; Donchin, M.; Zwas, D.R. Two-Phase Evaluation of a Community-Based Lifestyle Intervention for Palestinian Women in East Jerusalem: A Quasi-Experimental Study Followed by Dissemination. Int. J. Environ. Res. Public Health 2020, 17, 9184. https://doi.org/10.3390/ijerph17249184
Agbaria N, Nubani-Husseini M, Barakat RA, Leiter E, Greenberg KL, Karjawally M, Keidar O, Donchin M, Zwas DR. Two-Phase Evaluation of a Community-Based Lifestyle Intervention for Palestinian Women in East Jerusalem: A Quasi-Experimental Study Followed by Dissemination. International Journal of Environmental Research and Public Health. 2020; 17(24):9184. https://doi.org/10.3390/ijerph17249184
Chicago/Turabian StyleAgbaria, Nisreen, Maha Nubani-Husseini, Raghda A. Barakat, Elisheva Leiter, Keren L. Greenberg, Mayada Karjawally, Osnat Keidar, Milka Donchin, and Donna R. Zwas. 2020. "Two-Phase Evaluation of a Community-Based Lifestyle Intervention for Palestinian Women in East Jerusalem: A Quasi-Experimental Study Followed by Dissemination" International Journal of Environmental Research and Public Health 17, no. 24: 9184. https://doi.org/10.3390/ijerph17249184
APA StyleAgbaria, N., Nubani-Husseini, M., Barakat, R. A., Leiter, E., Greenberg, K. L., Karjawally, M., Keidar, O., Donchin, M., & Zwas, D. R. (2020). Two-Phase Evaluation of a Community-Based Lifestyle Intervention for Palestinian Women in East Jerusalem: A Quasi-Experimental Study Followed by Dissemination. International Journal of Environmental Research and Public Health, 17(24), 9184. https://doi.org/10.3390/ijerph17249184