South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Data Collection and Procedure
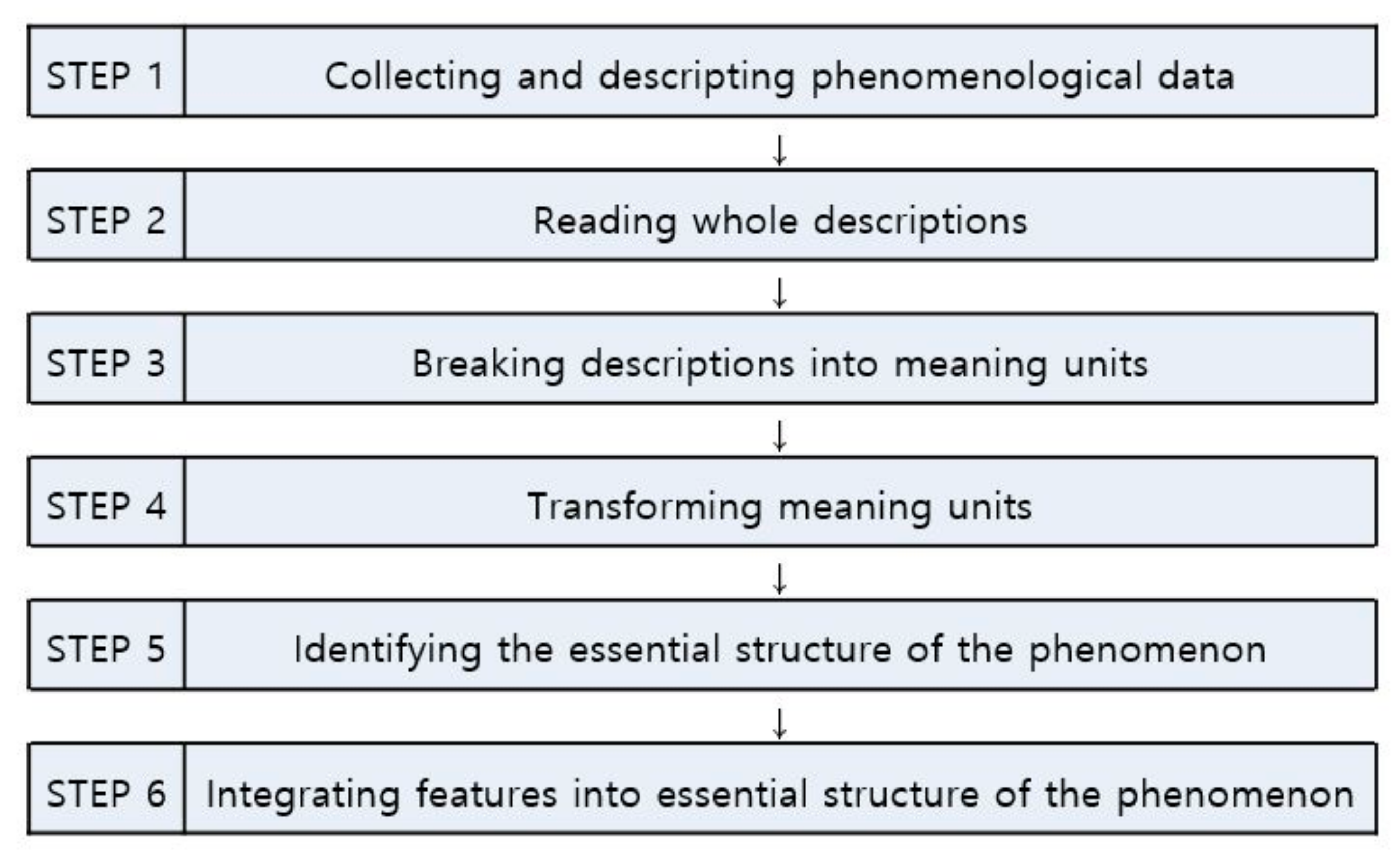
2.4. Data Analysis
2.5. Rigor
2.6. Ethical Considerations
3. Results
3.1. Pushed into the Battlefield without Any Preparation
3.1.1. Unavoidable Duty
Because our hospital is a public hospital, I suspected that we would care for infected patients once an infectious disease outbreak occurs. However, when the mayor announced that our hospital would be officially designated as a COVID-19 hospital, I got scared since I had never done it before.Feeling of being sent to a battlefield? Feeling a sense of unavoidable duty since the country was facing a major crisis.
3.1.2. Limited Preparation Time
It was like a dream to see all that happen in a few days. I took a few days off and went to work, and I was immediately placed in a situation caring for COVID-19 patients.Once I saw a senior nurse wearing PPE and I immediately put on PPE, looking at myself in the mirror. Then I went straight into the isolation unit. Everything was so urgent that I was embarrassed and anxious. I even doubted myself if I was wearing the PPE properly
3.1.3. Fear of an Unknown Enemy
It was really scary before entering the isolation unit for the first time while wearing PPE. Even though I had a mask and goggles on, will those protect me… Is it safe to breathe…There was no treatment, and I didn’t even know the route of transmission at first… I was so scared that it felt like entering hell.
3.2. Struggling on the Frontline
3.2.1. Constantly Changing Guidelines That Lack Details
The guidelines kept changing, and that was somewhat confusing. Even when the infection control office told us the guidelines, there were many ambiguities as we worked in the field, so we kept asking questions…The guidelines kept changing. It made us anxious, and we kept thinking, “Is this right?” even though we were following the guidelines.
3.2.2. Discomfort Due to Personal Protective Equipment
First of all, just doing my work while wearing PPE was hot and difficult. When wearing an N95 mask, it was really difficult to breathe, and I even felt dizzy at times.When I wore goggles, they would fog up, and I couldn’t see. And then, as it got foggier, drops of water would drip down inside the goggles. I could only do my work by looking through the drip mark. And I had to wear three layers of gloves and put in an IV line. My hands became ungainly, and it took much longer than usual. I felt like a beginner nurse with everything being new.
3.2.3. Unfamiliar Work
Once the patient is admitted, the nurse has to take care of everything. Tidying up personal belongings and taking vital signs are basic stuff, but the nurses were responsible for everything, even feeding, putting away trays after eating, and cleaning the room. The number of trash cans that I personally had to take care of was over ten.Because we had to be the caregiver, guardian, and nurse, I had to be hands-on for even the smallest things. That made it difficult. It’s not something I’m used to doing…
3.2.4. A Series of Unexpected Situations
The number of confirmed cases, infection control instructions guidelines… Everything happened without warning. That’s what made us crazy. But even in that situation, we had to do our best. patients are rushed in all at once, we are completely out of our minds…We reduced the number of nurses on duty since the number of patients decreased, but because several patients were admitted suddenly, I went to work in the early morning and got off work at night… Patients were admitted suddenly, and the charge nurse had to come to work on a scheduled off-day.
3.3. Altered Daily Life
3.3.1. Reinforced Infection Policies within the Hospital
We used to eat together with our masks off. After that [a nurse became infected], we stopped eating all together and were split up into teams to eat, separated from each other, and facing the wall. It’s necessary to prevent infection, but the great pleasure of talking over meals is gone.After a colleague nurse was confirmed as having COVID-19, the hospital is testing [healthcare professionals] once a month for COVID-19. Tomorrow’s the test day. I’m always nervous until the results come back.
3.3.2. Becoming Sensitive to Even Minor Symptoms
I had a severe cold. I didn’t have any fever at first, but my throat was hurting so much. I was anxious. Was it because the shield had ripped [while caring for infected patients]? I kept thinking about it. I kept coughing the next day. I was convinced that I became infected and spent the whole day crying.I had a headache and mild fever. Did I get COVID-19? I was worried, and since I have a child at home, I went to my mom’s house and slept there.
3.3.3. Voluntarily Restricting Social Activities
Because I need to be careful… I used to work out, but I don’t go to the gym any more… I used to enjoy getting together with people, but I can’t do it anymore, which makes me realize how precious my daily life was.When I go home now, I wash my hands right away. I touch my child, but no kisses…
3.3.4. Cohort Isolation after the Confirmed Diagnosis of a Colleague
After hearing the news about a nurse being confirmed as having COVID-19, it made me think that COVID-19 isn’t just someone else’s concern.About 90 people who worked together or came in contact with the nurse diagnosed with COVID-19 were classified as the “red group” and were placed in isolation at the hospital for 14 days.
3.4. Low Morale
3.4.1. My Labor Is Not Being Properly Recognized
Doctors and clinical pathologists do not go into the isolation unit often, and they come right back out once their work is done. Nurses, on the other hand, perform not only their nursing work but also have to assist those people [doctors and clinical pathologists] when they come in and tidy up after they leave… So, nurses spend much more time in the isolation unit and have more work to do.I haven’t received any bonuses yet. I’ve heard many rumors about bonuses, some saying that doctors are going to get more bonuses. Nurses have the toughest time, but when I hear rumors like that, it is really disheartening and frustrating.
3.4.2. Being Treated Like a Virus
I can’t tell others about working at this hospital because when I asked the taxi driver to take me to the hospital, he asked me if I worked there, and then he told me to get out. They don’t even deliver food to the hospital. I wasn’t infected with COVID-19, and I didn’t do anything wrong, but I had to stay at home. Because people don’t want contact with me.My child goes to preschool. I told the teacher at preschool that I won’t be sending my child there for a while, just in case my child might get infected because of me. The teacher seemed relieved and happy when I mentioned that.
3.4.3. Strict Social Standards
When a nurse was diagnosed with COVID-19, it was from taking care of patients. However, she became a target of criticism, questioning whether she took off her PPE properly. Seeing that made me really angry. If I were put in that position, I would quit….When I read the news, there were comments about why do healthcare professionals who deal with confirmed patients go out to eat or go to the gym… Honestly, we can go out to eat. We really get hurt when we see malicious comments like that.
3.5. Unexpectedly Long War
3.5.1. Despair with No End in Sight
The number of confirmed cases has been on the rise again as people have gone to nightclubs, anti-government protests, and religious gatherings without following the government’s guidelines for infection control. They don’t even have a screening test for fear of being criticized when confirmed, and they infect people around them. Being anxious about no end in sight. Will this ever end? Everyone is so tired and crazed. Nobody thought this would last this long…
3.5.2. Tired Body and Mind
How long do I have to work like this?… They call it the corona blues. I think that applies to me.In the beginning, we had the personnel to take shifts, so the time spent in the isolation unit was short. Back then, I felt refreshed after showering, but that’s not the case now. I’m taking a lot of analgesics due to headaches.
3.5.3. Concerns about General Nursing Competency
In my two years of nursing experience, I spent seven months exclusively caring for COVID-19 patients. It’s because when a COVID-19 patient becomes seriously ill, that patient is transferred to another hospital. Actually, nursing while wearing PPE involves just the basics… I’m gaining experience, but…Would I be able to do my work properly when I go back to the ward I was working in? I think I will be confused from not working there for so long.
3.6. Ambivalence toward Patients
3.6.1. Having a Bias
In the beginning, there were many patients who were members of a religious cult. Maybe that’s the reason for thinking, “They’re somewhat weird”…The government emphasized no mass gatherings, and anyone who’s been to a mass gathering should get tested… They didn’t cooperate… Because that is how I viewed them, I couldn’t really sympathize with them like other patients…
3.6.2. Becoming Angry at Uncooperative Attitudes
The patients wanted to eat outside food, so they had food delivered to the hospital lobby and asked us to go get it for them… We told them not to, but they kept doing it…When a patient requests something, it takes time for us to put on PPE, so we can’t go in right away. Some patients become angry that we came a bit late, and one even threw a blood pressure meter at us.
3.6.3. Feelings of Pity
Among the isolated patients, there were some who could not accept the confirmed diagnosis and cried about needing to go home. When I saw that, I thought about how that could happen to me or to my mom or family.After being admitted to the isolation unit, [they were] just sitting there crying without eating, crying while talking to family…There are many patients like that. It makes me sad.
3.6.4. Solidarity with the Patients
When the test result came back negative for the first time after being admitted, I was so happy and cried together with the patients.There is something different than regular patients because of the thought that we provided care under the dangers of an unknown infectious disease and overcame it together.
3.7. Forces That Keep Me Going
3.7.1. Concerns from Family and Friends
My family worries about me a lot and calls me often to take care of my health.My friends know I work in a COVID-19-designated hospital. They always call me to cheer me up and tell me that I’m really cool.
3.7.2. Patients Showing Their Appreciation
The patient said, “If I didn’t get infected, you wouldn’t have to do this… So much trouble for you.”Unlike regular patients, they [COVID-19 patients] have been pushed to the brink from an extreme situation. I think that’s why they lean on us and depend on us. So, they express their gratitude a lot. Even after being discharged, they sent text messages saying they will not forget how grateful they were during their stay.
3.7.3. Public Support
I was so grateful that people gave recognition to our struggles through the “Thank You Challenge.” Not only food, but since we have to wash frequently, people have given shampoo and cosmetics to us. It felt great, and I was proud whenever we received donated goods…I got emotional when reading letters written by kindergarteners with messy writing that said, “Dear nurse… You are working really hard. Thank you very much for treating corona patients.”
3.7.4. Strengthened Camaraderie
Before, I was criticized for mistakes… Now, everything is new for everyone. Even if I am not proficient at something, they say it’s okay, just do it carefully… It’s an atmosphere of everyone encouraging each other. I feel it’s more so because we are overcoming a difficult situation together.Before, patients or guardians would come by the nurses’ station, so that the nurses couldn’t talk about personal matters. Now, the patients are in the isolation unit, and we have time to talk amongst ourselves. So we talk to each other to relieve stress and become closer to each other.
3.8. Giving Meaning to My Work
3.8.1. Calling to Do the Work Expected of Me
Because it is a public institution, I always think that if something happens in the city, I’ll be put to work. Even if there is another infectious disease outbreak, I will do it again. It’s my job.You can think of it as if I prevent the spread of the virus by treating these patients, then that is something I’m doing to protect my family. It’s just how you view it. Since it’s work assigned to me, I’ll do my best. That’s how I think…
3.8.2. Opportunity for a New Experience
Caring for COVID-19 patients… It’s not something you can do just because you want to. I experienced infectious disease patient care, which other nurses could not. I am thankful.Because there were nurses from various wards, many nurses had much more experience than me. I learned a lot from watching those nurses carry on with their work. I thought that my competencies could be upgraded a level…
3.8.3. Pride as a Committed COVID-19 Nurse
The work that I’m doing is truly helping someone else. I am contributing during this national disaster situation. I am there at this historical moment…In the beginning, there were a lot of broadcasts with touching stories about the occupation of nursing. The feeling of others looking at us differently? Because of being COVID-19 hospital nurses… there is a sense that everyone is looking at us somewhat differently.
3.9. Taking Another Step in One’s Growth
3.9.1. Providing Real Nursing
I didn’t need to feed them since nursing assistants or family caregivers normally help them with their meals. However, I double checked to make sure there is no risk of aspiration while being fed. Since I’ve been changing their positions, I think about what could be done to reduce bedsores…Before, I didn’t think I looked after the patient’s mood. But now, those things come into view. You notice their changes in expression, and the voice of the patient when his or her neighbor in the next bed is discharged. They feel depressed. That’s why we came up with the idea of getting song requests from the patients and playing those songs. Young patients even dance inside the room and really liked it.
3.9.2. Broadening Perspectives
We need to train new nurses on donning and doffing PPE like in real-life situations, and we also need stress and depression management for nurses, since caring for COVID-19 patients is becoming long-term.Additional staffing is needed the most. We also need symptom assessment by telephone to minimize contact with the patients and a system to enable drug administration and treatments to take place according to mealtimes.
3.9.3. Confidence in Caring for Infected Patients
Now, there is a lot less fear. After caring for infected patients for seven months, I believe I’ve gained a certain level of competency in caring for infected patients, and I can do the job when such an infectious disease outbreak occurs again.It’s not like Wonder Woman or Superman, but the thought that I can be helpful when another infectious disease outbreak occurs since I’ve gained experience in caring for infected patients. I also have the feeling of wanting to experience it.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline?gclid=Cj0KCQjwk8b7BRCaARIsAARRTL4vhFybBt3a370bdeWavaZ4DmxtOQshDMzdML3nKeGKa9GXWJTkkFsaAkppEALw_wcB#event-72 (accessed on 23 September 2020).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: http://www.who.int (accessed on 24 November 2020).
- Gavi. How does Covid-19 Compare to Past Pandemics? Available online: https://www.gavi.org/vaccineswork/how-does-covid-19-compare-past-pandemics (accessed on 23 September 2020).
- Haleem, A.; Javaid, M.; Vaishya, R. Effects of COVID-19 pandemic in daily life. Curr. Med. Res. Pract. 2020, 10, 78–79. [Google Scholar] [CrossRef]
- Campos, J.A.D.B.; Martins, B.G.; Campos, L.A.; Marôco, J.; Saadiq, R.A.; Ruano, R. Early Psychological Impact of the COVID-19 Pandemic in Brazil: A National Survey. J. Clin. Med. 2020, 9, 2976. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Passos, L.; Prazeres, F.; Teixeira, A.; Martins, C. Impact on mental health due to COVID-19 pandemic: Cross-sectional study in Portugal and Brazil. Int. J. Environ. Res. Public Health 2020, 17, 6794. [Google Scholar] [CrossRef] [PubMed]
- Maciaszek, J.; Ciulkowicz, M.; Misiak, B.; Szczesniak, D.; Luc, D.; Wieczorek, T.; Fila-Witecka, K.; Gawlowski, P.; Rymaszewska, J. Mental Health of Medical and Non-Medical Professionals during the Peak of the COVID-19 Pandemic: A Cross-Sectional Nationwide Study. J. Clin. Med. 2020, 9, 2527. [Google Scholar] [CrossRef]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental Health survey of 230 medical staff in a tertiary infectious disease hospital for COVID-19. Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, 192–195. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Liao, C.; Wang, N.; Qin, M.; Huang, H. Work stress among Chinese nurses to support Wuhan in fighting against COVID-19 epidemic. J. Nurs. Manag. 2020, 28, 1002–1009. [Google Scholar] [CrossRef]
- An, Y.; Yang, Y.; Wang, A.; Li, Y.; Zhang, Q.; Cheung, T.; Ungvari, G.S.; Qin, M.Z.; An, F.R.; Xiang, Y.T. Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J. Affect. Disord. 2020, 276, 312–315. [Google Scholar] [CrossRef]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y. Work stress, perceived social support, self-efficacy and burnout among Chinese registered nurses. J. Nurs. Manag. 2019, 27, 1445–1453. [Google Scholar] [CrossRef]
- Labrague, L.J.; de los Santos, J.A.A. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among front line nurses. J. Nurs. Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef]
- Naushad, V.A.; Bierens, J.J.L.M.; Nishan, K.P.; Firjeeth, C.P.; Mohammad, O.H.; Maliyakkal, A.M.; Chali Hadan, S.; Schreiber, M.D. A systematic review of the impact of disaster on the mental health of medical responders. Prehospital Disaster Med. 2019, 34, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Han, B.; Jiang, R.; Huang, Y.; Ma, C.; Wen, J.; Zhang, T.; Wang, Y.; Chen, H.; Ma, Y. Mental Health Status of Doctors and Nurses During COVID-19 Epidemic in China. Lancet 2020. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, 790–798. [Google Scholar] [CrossRef]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef]
- Tan, R.; Yu, T.; Luo, K.; Teng, F.; Liu, Y.; Luo, J.; Hu, D. Experience of clinical first-line nurses treating patients with COVID-19: A qualitative study. J. Nurs. Manag. 2020, 28, 1381–1390. [Google Scholar] [CrossRef]
- Pan, Y.; Guan, H. Imaging changes in patients with 2019-nCov. Eur. Radiol. 2020, 30, 3612–3613. [Google Scholar] [CrossRef]
- The Wall Street Journal. How South Korea Successfully Managed Coronavirus. Available online: https://www.wsj.com/articles/lessons-from-south-korea-on-how-to-manage-covid-11601044329 (accessed on 28 September 2020).
- Giorgi, A. The descriptive phenomenological psychological method. J. Phenomenol. Psychol. 2012, 43, 3–12. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Kim, Y.J. Nurses’ experiences of care for patients with Middle East Respiratory Syndrome-coronavirus in South Korea. Am. J. Infect. Control 2018, 46, 781–787. [Google Scholar] [CrossRef]
- Nasiri, A.; Balouchi, A.; Rezaie-Keikhaie, K.; Bouya, S.; Sheyback, M.; Rawajfah, O.A. Knowledge, attitude, practice, and clinical recommendation toward infection control and prevention standards among nurses: A systematic review. Am. J. Infect. Control 2019, 47, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Chughtai, A.A.; Chen, X.; Macintyre, C.R. Risk of self-contamination during doffing of personal protective equipment. Am. J. Infect. Control 2018, 46, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- McLaws, M.; Chughtai, A.A.; Salmon, S.; MacIntyre, C.R. A highly precautionary doffing sequence for health care workers after caring for wet Ebola patients to further reduce occupational acquisition of Ebola. Am. J. Infect. Control 2016, 44, 740–744. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Infection Prevention and Control of Epidemic-and Pandemic-Prone Acute Respiratory Infections in Health Care. Available online: https://www.who.int/csr/bioriskreduction/infection_control/publication/en/ (accessed on 21 November 2020).
- Lam, K.K.; Hung, S.Y.M. Perceptions of emergency nurses during the human swine influenza outbreak: A qualitative study. Int. Emerg. Nurs. 2013, 21, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.L.; Seo, E.J.; Seo, Y.S.; Dee, V.; Hong, E.H. Effects of Middle East Respiratory Syndrome Coronavirus on post-traumatic stress disorder and burnout among registered nurses in South Korea. Int. J. Healthc. 2018, 4, 27–33. [Google Scholar] [CrossRef][Green Version]
- Ishimaru, T.; Wada, K.; Hoang, H.T.X.; Bui, A.T.M.; Nguyen, H.D. Nurses’ willingness to care for patients infected with HIV or Hepatitis B/C in Vietnam. Environ. Health Prev. Med. 2017, 22. [Google Scholar] [CrossRef]
- Sheng, Q.; Zhang, X.; Wang, X.; Chunfeng, C. The influence of experiences of involvement in the COVID-19 rescue task on the professional identity among Chinese nurses: A qualitative study. J. Nurs. Manag. 2020, 28, 1662–1669. [Google Scholar] [CrossRef]
- Kackin, O.; Ciydem, E.; Aci, O.S.; Kutlu, F.Y. Experiences and psychosocial problems of nurses caring for patients diagnosed with COVID-19 in Turkey: A qualitative study. Int. J. Soc. Psychiatry 2020, 28, 1662–1669. [Google Scholar] [CrossRef]
- Jung, W.S.; Cho, H.K. Punishment When Refused to Attend School of Child with Medical Staff Parents Caring MERS-CoV Infection Patients. The Kyunghyang Shinmun. 2 June 2015. Available online: http://news.khan.co.kr/kh_news/khan_art_view.html?artid=201506212253315&code=940100 (accessed on 30 September 2020).
- Hlongwane, N.; Madiba, S. Navigating life with HIV as an older adult in South African communities: A phenomenological study. Int. J. Environ. Res. Public Health 2020, 17, 5797. [Google Scholar] [CrossRef]
- Zeligman, M.; Barden, S.; Hagedorn, W.B. Posttraumatic growth and HIV: A study on associations of stigma and social support. J. Couns. Dev. 2016, 94, 141–149. [Google Scholar] [CrossRef]
- Calhoun, L.G.; Tedeschi, R.G. The foundations of posttraumatic growth: New considerations. Psychol. Inq. 2004, 15, 93–102. [Google Scholar] [CrossRef]
- Furlotte, C.; Schwartz, K. Mental health experiences of older adults living with HIV: Uncertainty, stigma, and approaches to resilience. Can. J. Aging 2017, 36, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, S.H.A.; Morgan, B.J.; Parshall, M.B. Resilience, stress, stigma, and barriers to mental healthcare in U.S. Air Force nursing personnel. Nurs. Res. 2016, 65, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Waluyo, A.; Culbert, G.J.; Levy, J.; Norr, K.F. Understanding HIV-related stigma among Indonesian nurses. J. Assoc. Nurses Aids Care 2015, 26, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Francisco, D.H.; Duarte-Clíments, G.; del Rosario-Melián, J.M.; Gómez-Salgado, J.; Romero-Martín, M.; Sánchez-Gómez, M.B. Influence of workload on primary care nurses’ health and burnout, patients’ safety, and quality of care: Integrative Review. Healthcare 2020, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Wessely, S.; Wykes, T. Potential mental health consequences for workers in the Ebola Regions of West Africa- a les-son for all challenging environments. J. Ment. Health 2015, 24, 1–3. [Google Scholar] [CrossRef]
- Shaban, R.Z.; Nahidi, S.; Sotomayor-Castillo, C.; Li, C.; Gilroy, N.; O’Sullivan, M.V.N.; Sorrell, T.C.; White, E.; Hackett, K.; Bag, S. SARS-CoV-2 infection and COVID-19: The lived experience and perceptions of patients in isolation and care in an Australian healthcare setting. Am. J. Infect. Control 2020, 1–6. [Google Scholar] [CrossRef]
- Gammon, J.; Hunt, J. The stigmatisation of source isolation: A literature review. J. Res. Nurs. 2019, 24, 677–693. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Song, Y.J.; Ki, M.; Min, J.A.; Cho, J.; Chae, J.H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, 016048. [Google Scholar] [CrossRef]
- Calhoun, L.G.; Tedeschi, R.G. Posttraumatic Growth in Clinical Practice; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Benner, P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice; Addison-Wesley: Menlo Park, CA, USA, 1984. [Google Scholar]


{kind=link}
| Themes | Subthemes |
|---|---|
| Pushed onto the Battlefield without Any Preparation | Unavoidable Duty |
| Limited Preparation Time | |
| Fear of an Unknown Enemy | |
| Struggling on the Frontline | Constantly Changing Guidelines that Lack Details |
| Discomfort Due to Personal Protective Equipment | |
| Unfamiliar Work | |
| A Series of Unexpected Situations | |
| Altered Daily Life | Reinforced Infection Policies Within the Hospital |
| Becoming Sensitive to Even Minor Symptoms | |
| Voluntarily Restricting Social Activities | |
| Cohort Isolation after the Confirmed Diagnosis of a Colleague | |
| Low Morale | My Labor Is Not Being Properly Recognized |
| Being Treated Like a Virus | |
| Strict Social Standards | |
| Unexpectedly Long War | Despair with No End in Sight |
| Tired Body and Mind | |
| Concerns about General Nursing Competency | |
| Ambivalence Toward Patients | Having a Bias |
| Becoming Angry at Uncooperative Attitudes | |
| Feelings of Pity | |
| Solidarity with the Patients | |
| Forces That Keep Me Going | Concerns from Family and Friends |
| Patients Showing Their Appreciation | |
| Public Support | |
| Strengthened Camaraderie | |
| Giving Meaning to My Work | Called to Do the Work Expected of Me |
| Opportunity for a New Experience | |
| Pride as a Committed COVID-19 Nurse | |
| Taking Another Step in One’s Growth | Providing Real Nursing |
| Broadening Perspectives | |
| Confidence in Caring for Infected Patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Lee, H.-J. South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9015. https://doi.org/10.3390/ijerph17239015
Lee N, Lee H-J. South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(23):9015. https://doi.org/10.3390/ijerph17239015
Chicago/Turabian StyleLee, Nayoon, and Hyun-Ju Lee. 2020. "South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic" International Journal of Environmental Research and Public Health 17, no. 23: 9015. https://doi.org/10.3390/ijerph17239015
APA StyleLee, N., & Lee, H.-J. (2020). South Korean Nurses’ Experiences with Patient Care at a COVID-19-Designated Hospital: Growth after the Frontline Battle against an Infectious Disease Pandemic. International Journal of Environmental Research and Public Health, 17(23), 9015. https://doi.org/10.3390/ijerph17239015