Mental Health and the Association between Asthma and E-cigarette Use among Young Adults in The United States: A Mediation Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Measures
2.2.1. Asthma Status
2.2.2. E-Cigarette Use
2.2.3. Mental Health Functioning
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
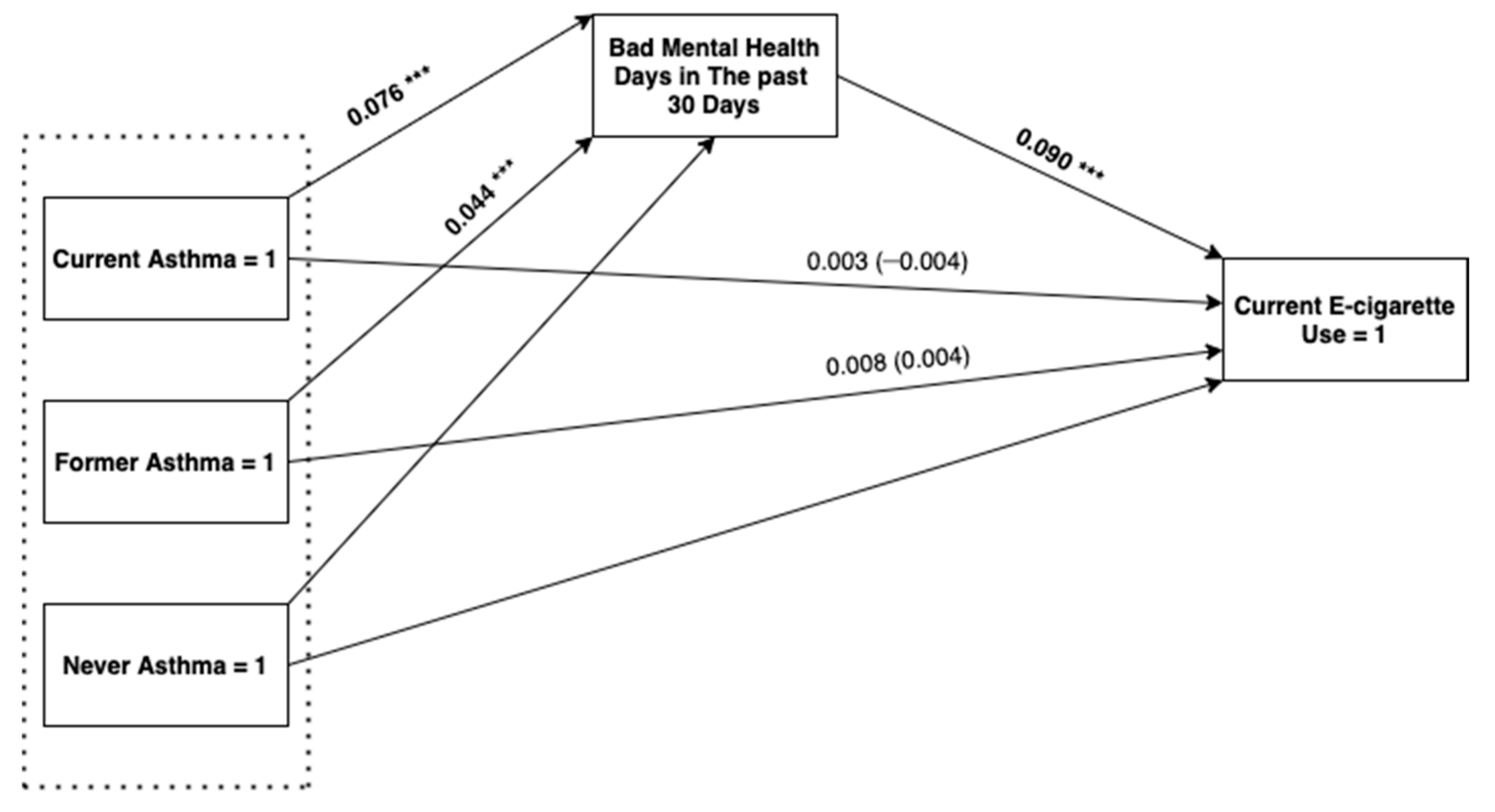
3.2. Indirect Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ebmeier, S.; Thayabaran, D.; Braithwaite, I.; Benamara, C.; Weatherall, M.; Beasley, R. Trends in international asthma mortality: Analysis of data from the WHO Mortality Database from 46 countries (1993–2012). Lancet 2017, 390, 935–945. [Google Scholar] [CrossRef]
- Sadatsafavi, M.; McTaggart-Cowan, H.; Chen, W.; FitzGerald, J.M. Quality of Life and Asthma Symptom Control: Room for Improvement in Care and Measurement. Value Health 2015, 18, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- He, Z.; Feng, J.; Xia, J.; Wu, Q.; Yang, H.; Ma, Q. Frequency of Signs and Symptoms in Persons with Asthma. Respir. Care 2020, 65, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Skaaby, T.; Taylor, A.E.; Jacobsen, R.K.; Paternoster, L.; Thuesen, B.H.; Ahluwalia, T.S.; Larsen, S.C.; Zhou, A.; Wong, A.; Gabrielsen, M.E.; et al. Investigating the causal effect of smoking on hay fever and asthma: A Mendelian randomization meta-analysis in the CARTA consortium. Sci. Rep. 2017, 7, 2224. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Nava, F.; Vazquez-Rodriguez, E.M.; Vazquez-Rodriguez, C.F.; Ruiz, O.C.; Herreros, J.P. Epidemiological profile of smoking and nicotine addiction among asthmatic adolescents. Public Health 2017, 149, 49–56. [Google Scholar] [CrossRef]
- Mitchell, E.A.; Beasley, R.; Keil, U.; Montefort, S.; Odhiambo, J.; ISAAC Phase Three Study Group. The association between tobacco and the risk of asthma, rhinoconjunctivitis and eczema in children and adolescents: Analyses from Phase Three of the ISAAC programme. Thorax 2012, 67, 941–949. [Google Scholar] [CrossRef]
- Tommola, M.; Ilmarinen, P.; Tuomisto, L.E.; Haanpää, J.; Kankaanranta, T.; Niemelä, O.; Kankaanranta, H. The effect of smoking on lung function: A clinical study of adult-onset asthma. Eur. Respir. J. 2016, 48, 1298–1306. [Google Scholar] [CrossRef]
- Wang, T.W.; Gentzke, A.; Sharapova, S.; Cullen, K.A.; Ambrose, B.K.; Jamal, A. Tobacco Product Use Among Middle and High School Students—United States, 2011–2017. Mmwr. Morb. Mortal. Wkly. Rep. 2018, 67, 629–633. [Google Scholar] [CrossRef]
- Singh, T.; Arrazola, R.A.; Corey, C.G.; Husten, C.G.; Neff, L.J.; Homa, D.M.; King, B.A. Tobacco Use Among Middle and High School Students—United States, 2011–2015. Mmwr. Morb. Mortal. Wkly. Rep. 2016, 65, 361–367. [Google Scholar] [CrossRef]
- Dai, H.; Leventhal, A.M. Prevalence of e-Cigarette Use Among Adults in the United States, 2014–2018. JAMA 2019, 322, 1824–1827. [Google Scholar] [CrossRef] [PubMed]
- Krishnan-Sarin, S.; Jackson, A.; Morean, M.; Kong, G.; Bold, K.W.; Camenga, D.R.; Cavallo, D.A.; Simon, P.; Wu, R. E-cigarette devices used by high-school youth. Drug Alcohol Depend. 2019, 194, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Mirbolouk, M.; Charkhchi, P.; Kianoush, S.; Uddin, S.M.I.; Orimoloye, O.A.; Jaber, R.; Bhatnagar, A.; Benjamin, E.J.; Hall, M.E.; DeFilippis, A.P.; et al. Prevalence and Distribution of E-Cigarette Use Among U.S. Adults: Behavioral Risk Factor Surveillance System, 2016. Ann. Intern. Med. 2018, 169, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.F.; Atuegwu, N.C.; Oncken, C.; Mead, E.L.; Mortensen, E.M. Association between Electronic Cigarette Use and Asthma in Never-Smokers. Ann. Am. Thorac. Soc. 2019, 16, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Bernat, D. E-Cigarette Use Among Florida Youth With and Without Asthma. Am. J. Prev. Med. 2016, 51, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, R.J.; Wills, T.A.; Tam, E.; Pagano, I.; Choi, K. E-cigarette use and asthma in a multiethnic sample of adolescents. Prev. Med. 2017, 105, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.; Faulkner, G.E.J.; Boak, A.; Hamilton, H.A.; Mann, R.E.; Irving, H.M.; To, T.; Canadian Respiratory Research Network. Looking beyond cigarettes: Are Ontario adolescents with asthma less likely to smoke e-cigarettes, marijuana, waterpipes or tobacco cigarettes? Respir. Med. 2016, 120, 10–15. [Google Scholar] [CrossRef]
- Fedele, D.A.; Barnett, T.E.; Dekevich, D.; Gibson-Young, L.M.; Martinasek, M.; Jagger, M.A. Prevalence of and beliefs about electronic cigarettes and hookah among high school students with asthma. Ann. Epidemiol. 2016, 26, 865–869. [Google Scholar] [CrossRef]
- Eltorai, A.E.; Choi, A.R.; Eltorai, A.S. Impact of Electronic Cigarettes on Various Organ Systems. Respir. Care 2019, 64, 328–336. [Google Scholar] [CrossRef]
- Palmer, R.; Young, S.; Hopfer, C.; Corley, R.; Stallings, M.; Crowley, T.; Hewitt, J. Developmental epidemiology of drug use and abuse in adolescence and young adulthood: Evidence of generalized risk. Drug Alcohol Depend. 2009, 102, 78–87. [Google Scholar] [CrossRef]
- Sussman, S.; Arnett, J.J. Emerging adulthood: Developmental period facilitative of the addictions. Eval. Health Prof. 2014, 37, 147–155. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health & Human Services. Surgeon General Releases Advisory on E-Cigarette Epidemic among Youth. Available online: https://www.hhs.gov/about/news/2018/12/18/surgeon-general-releases-advisory-e-cigarette-epidemic-among-youth.html (accessed on 19 October 2018).
- Jones, S.E.; King, B.A.; Leroy, Z. Trends in the use of cigarettes, cigars, and marijuana among students with and without asthma, 2003–2017. J. Asthma 2019, 57, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Thirion-Romero, I.; Perez-Padilla, R.; Zabert, G.; Barrientos-Gutierrez, I. Respiratory impact of electronic cigarettes and “low-risk” tobacco. Rev. De Investig. Clínica. 2019, 71, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Coakley, R.D.; Ghio, A.J.; Muhlebach, M.S.; Esther, C.R., Jr.; Alexis, N.E.; Tarran, R. Chronic E-Cigarette Use Increases Neutrophil Elastase and Matrix Metalloprotease Levels in the Lung. Am. J. Respir. Crit. Care Med. 2019, 200, 1392–1401. [Google Scholar] [CrossRef] [PubMed]
- Hedman, L.; Backman, H.; Stridsman, C.; Bosson, J.A.; Lundbäck, M.; Lindberg, A.; Rönmark, E.; Ekerljung, L. Association of Electronic Cigarette Use With Smoking Habits, Demographic Factors, and Respiratory Symptoms. JAMA Netw. Open 2018, 1, e180789. [Google Scholar] [CrossRef]
- Wills, T.A.; Pagano, I.; Williams, R.J.; Tam, E.K. E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend. 2019, 194, 363–370. [Google Scholar] [CrossRef]
- Hiemstra, P.S.; Bals, R. Effects of E-Cigarette Use on Human Lung Tissue. On Harm Reduction and Causing Harm. Am. J. Respir. Crit. Care Med. 2018, 198, 6–7. [Google Scholar] [CrossRef]
- Bradford, L.E.; Rebuli, M.E.; Ring, B.J.; Jaspers, I.; Clement, K.C.; Loughlin, C.E. Danger in the vapor? ECMO for adolescents with status asthmaticus after vaping. J. Asthma. 2020, 57, 1168–1172. [Google Scholar] [CrossRef]
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Majeskie, M.R.; Fiore, M.C. Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychol. Rev. 2004, 111, 33–51. [Google Scholar] [CrossRef]
- Pilipenko, N.; Karekla, M.; Georgiou, A.; Feldman, J. Impact of psychiatric illness upon asthma patients’ health care utilization and illness control. Are all psychiatric comorbidities created equal? Psychol. Health Med. 2016, 21, 787–799. [Google Scholar] [CrossRef]
- Bardach, N.S.; Neel, C.; Kleinman, L.C.; McCulloch, C.E.; Thombley, R.; Zima, B.T.; Grupp-Phelan, J.; Coker, T.R.; Cabana, M.D. Depression, Anxiety, and Emergency Department Use for Asthma. Pediatrics 2019, 144, e20190856. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; de Jonge, P.; Lim, C.C.W.; Aguilar-Gaxiola, S.; Bruffaerts, R.; Caldas-de-Almeida, J.M.; Liu, Z.; O’Neill, S.; Stein, D.J.; Viana, M.C.; et al. Association between mental disorders and subsequent adult onset asthma. J. Psychiatr. Res. 2014, 59, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Stickley, A.; Singh, F.; Koyanagi, A. Self-reported asthma diagnosis and mental health: Findings from the Collaborative Psychiatric Epidemiology Surveys. Psychiatry Res. 2019, 271, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Labor, M.; Labor, S.; Jurić, I.; Fijačko, V.; Grle, S.P.; Plavec, D. Mood disorders in adult asthma phenotypes. J. Asthma 2018, 55, 57–65. [Google Scholar] [CrossRef]
- Pierannunzi, C.; Hu, S.S.; Balluz, L. A systematic review of publications assessing reliability and validity of the Behavioral Risk Factor Surveillance System (BRFSS), 2004–2011. BMC Med. Res. Methodol. 2013, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Stata. Stata Structural Equation Modeling Reference Manual Release 13; Stata Press: College Station, TX, USA, 2017. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Mikosz, C.A.; Danielson, M.; Anderson, K.N.; Pollack, L.A.; Currie, D.W.; Njai, R.; Evans, M.E.; Goodman, A.B.; Twentyman, E.; Wiltz, J.L.; et al. Characteristics of Patients Experiencing Rehospitalization or Death After Hospital Discharge in a Nationwide Outbreak of E-cigarette, or Vaping, Product Use: Associated Lung Injury—United States, 2019. Mmwr. Morb. Mortal. Wkly. Rep. 2020, 68, 1183–1188. [Google Scholar] [CrossRef]
- Schier, J.G.; Meiman, J.G.; Layden, J.; Mikosz, C.A.; VanFrank, B.; King, B.A.; Salvatore, P.P.; Weissman, D.N.; Thomas, J.; Melstrom, P.C.; et al. Severe Pulmonary Disease Associated with Electronic-Cigarette-Product Use—Interim Guidance. Mmwr. Morb. Mortal. Wkly. Rep. 2019, 68, 787–790. [Google Scholar] [CrossRef]
- Perrine, C.G.; Pickens, C.M.; Boehmer, T.K.; King, B.A.; Jones, C.M.; DeSisto, C.L.; Duca, L.M.; Lekiachvili, A.; Kenemer, B.; Shamout, M.; et al. Characteristics of a Multistate Outbreak of Lung Injury Associated with E-cigarette Use, or Vaping—United States, 2019. Mmwr. Morb. Mortal. Wkly. Rep. 2019, 68, 860–864. [Google Scholar] [CrossRef]
- Whiteford, H.A.; Ferrari, A.J.; Degenhardt, L.; Feigin, V.; Vos, T. The global burden of mental, neurological and substance use disorders: An analysis from the Global Burden of Disease Study 2010. PLoS ONE 2015, 10, e0116820. [Google Scholar] [CrossRef]
- Riehm, K.E.; Young, A.S.; Feder, K.A.; Krawczyk, N.; Tormohlen, K.N.; Pacek, L.R.; Mojtabai, R.; Crum, R.M. Mental Health Problems and Initiation of E-cigarette and Combustible Cigarette Use. Pediatrics 2019, 144, e20182935. [Google Scholar] [CrossRef]
- Lechner, W.V.; Janssen, T.; Kahler, C.W.; Audrain-McGovern, J.; Leventhal, A.M. Bi-directional associations of electronic and combustible cigarette use onset patterns with depressive symptoms in adolescents. Prev. Med. 2017, 96, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Kassel, J.D.; Evatt, D.P.; Greenstein, J.E.; Wardle, M.C.; Yates, M.C.; Veilleux, J.C. The acute effects of nicotine on positive and negative affect in adolescent smokers. J. Abnorm. Psychol. 2007, 116, 543. [Google Scholar] [CrossRef] [PubMed]
- Lappan, S.; Thorne, C.B.; Long, D.; Hendricks, P.S. Longitudinal and reciprocal relationships between psychological well-being and smoking. Nicotine Tob. Res. 2020, 22, 18–23. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. “Effect size estimates: Current use, calculations, and interpretation”: Correction to Fritz et al., (2011). J. Exp. Psychol. Gen. 2012, 141, 2. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Asthma = Never, Weighted %/Mean (SD) | Asthma = Former, Weighted %/Mean (SD) | Asthma = Current, Weighted %/Mean (SD) | F Ratio/t-Value, p-Value |
|---|---|---|---|---|
| E-cigarette use | 419.8, 0.015 | |||
| No current use | 90.42 | 86.91 | 90.10 | |
| Current use | 9.58 | 13.09 | 9.90 | |
| Bad mental health days in the past 30 days | 3.83 (0.17) | 4.18 (0.85) | 6.85 (0.42) | 56.41, <0.001 |
| Sex | 6162.40, <0.001 | |||
| Male | 51.86 | 64.40 | 37.55 | |
| Female | 48.14 | 35.60 | 62.45 | |
| Educational attainment | 16.07.1, <0.001 | |||
| Did not graduate high school | 10.90 | 9.11 | 15.27 | |
| Graduated high school | 38.15 | 40.46 | 35.96 | |
| Attended college or technical school | 39.04 | 39.53 | 38.37 | |
| Graduated from college or technical school | 11.91 | 10.90 | 10.40 | |
| Race | 2052.1, <0.001 | |||
| White | 67.58 | 69.79 | 69.12 | |
| Black | 14.51 | 13.78 | 18.78 | |
| Asian | 10.17 | 9.55 | 5.01 | |
| American Indian/ Alaskan Native | 1.89 | 1.68 | 2.54 | |
| Other | 5.85 | 5.20 | 4.55 | |
| Smoking status | 1488.0, <0.001 | |||
| Never smoker | 81.75 | 76.96 | 81.08 | |
| Former smoker | 6.37 | 6.11 | 6.36 | |
| Current someday smoker | 6.65 | 9.84 | 7.12 | |
| Current every day smoker | 5.22 | 7.09 | 5.45 | |
| COPD | 5841.18, <0.001 | |||
| No | 98.91 | 96.78 | 93.88 | |
| Yes | 1.09 | 3.22 | 6.12 | |
| Diabetes | 215.44, 0.090 | |||
| No | 99.01 | 98.54 | 98.30 | |
| Yes | 0.99 | 1.46 | 1.70 | |
| Chronic kidney disease | 777.10, 0.012 | |||
| No | 99.25 | 98.10 | 98.20 | |
| Yes | 0.75 | 1.90 | 1.80 | |
| Arthritis | 4622.37, <0.001 | |||
| No | 97.73 | 95.68 | 91.82 | |
| Yes | 2.27 | 4.32 | 8.18 | |
| Skin cancer | 1412.07, <0.001 | |||
| No | 99.73 | 99.40 | 98.48 | |
| Yes | 0.27 | 0.59 | 1.52 | |
| Other cancers | 580.96, <0.001 | |||
| No | 99.51 | 99.39 | 98.54 | |
| Yes | 0.49 | 0.61 | 1.46 | |
| WeightedN= 26,017,419 | WeightedN = 2,503,503 | WeightedN = 3,200,681 |
| Variable | Current E-Cigarette Use | |
|---|---|---|
| aOR | 95%CI | |
| Current asthma | 1.001 | 0.784, 1.278 |
| Former asthma | 1.069 | 0.786, 1.455 |
| Bad mental health days in the past 30 days | 1.020 | 1.011, 1.028 |
| Smoking status | ||
| Never smoker | Ref | Ref |
| Former smoker | 5.053 | 3.995, 6.393 |
| Current someday smoker | 3.996 | 3.176, 5.027 |
| Current every day smoker | 5.465 | 4.219, 7.079 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alanazi, A.M.M.; Alqahtani, M.M.; Pavela, G.; Ford, E.W.; Leventhal, A.M.; Hendricks, P.S. Mental Health and the Association between Asthma and E-cigarette Use among Young Adults in The United States: A Mediation Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8799. https://doi.org/10.3390/ijerph17238799
Alanazi AMM, Alqahtani MM, Pavela G, Ford EW, Leventhal AM, Hendricks PS. Mental Health and the Association between Asthma and E-cigarette Use among Young Adults in The United States: A Mediation Analysis. International Journal of Environmental Research and Public Health. 2020; 17(23):8799. https://doi.org/10.3390/ijerph17238799
Chicago/Turabian StyleAlanazi, Abdullah M. M., Mohammed M. Alqahtani, Gregory Pavela, Eric W. Ford, Adam M. Leventhal, and Peter S. Hendricks. 2020. "Mental Health and the Association between Asthma and E-cigarette Use among Young Adults in The United States: A Mediation Analysis" International Journal of Environmental Research and Public Health 17, no. 23: 8799. https://doi.org/10.3390/ijerph17238799
APA StyleAlanazi, A. M. M., Alqahtani, M. M., Pavela, G., Ford, E. W., Leventhal, A. M., & Hendricks, P. S. (2020). Mental Health and the Association between Asthma and E-cigarette Use among Young Adults in The United States: A Mediation Analysis. International Journal of Environmental Research and Public Health, 17(23), 8799. https://doi.org/10.3390/ijerph17238799