The Evolution of Covid-19 in Italy after the Spring of 2020: An Unpredicted Summer Respite Followed by a Second Wave

 ,
, 
 , and
, and 
Abstract
1. Introduction
2. Data Analysis
3. Discussion of Results
3.1. The Summer Mitigation
3.2. The Second Infection Wave: Where Are We Going?
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Oke, J.; Heneghan, C. Global COVID-19 Case Fatality Rates; Nuffield Department of Primary Care Health Sciences: Oxford, UK, 2020; Available online: https://www.cebm.net/global-COVID-19-case-fatality-rates/ (accessed on 23 October 2020).
- De Natale, G.; Ricciardi, V.; De Luca, G.; De Natale, D.; Di Meglio, G.; Ferragamo, A.; Marchitelli, V.; Piccolo, A.; Scala, A.; Somma, R.; et al. The COVID-19 Infection in Italy: A Statistical Study of an Abnormally Severe. Dis. J. Clin. Med. 2020, 9, 1564. [Google Scholar] [CrossRef] [PubMed]
- ISTAT Report, Primi Risultati Sull’indagine di Sieroprevalenza sul Sars-Cov-2. 2020. Available online: https://www.istat.it/it/files/2020/08/ReportPrimiRisultatiIndagineSiero.pdf (accessed on 28 October 2020). (In Italian).
- Reuters. New coronavirus Losing Potency, Top Italian Doctor Says. Thomson Reuters, World News. 31 May 2020. Available online: https://www.reuters.com/article/us-health-coronavirus-italy-virus/new-coronavirus-losing-potency-top-italian-doctor-says-idUSKBN2370OQ (accessed on 23 October 2020).
- Vespignani, A. Il Sole 24 Ore Infodata. 2020. Available online: https://www.infodata.ilsole24ore.com/2020/05/24/covid-19-modeling-italy-quattro-scenari-prevedere-contagio/ (accessed on 1 June 2020).
- Vollmer, M.A.C.; Mishra, S.; Unwin, H.J.T.; Gandy, A.; Mellan, T.A.; Bradley, V.; Zhu, H.; Coupland, H.; Hawryluk, I.; Hutchinson, M.; et al. Report 20: Using Mobility to Estimate the Transmission Intensity of COVID-19 in Italy: A Subnational Analysis with Future Scenarios Technical Report; Imperial College COVID-19 Response Team: London, UK, 2020; Available online: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-20-italy/ (accessed on 28 August 2020).
- Department of Italian Civil Protection Repository. Available online: http://opendatadpc.maps.arcgis.com/apps/opsdashboard/index.html#/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 26 October 2020).
- Wilson, N.; Kvalsvig, A.; Barnard, L.; Baker, M.G. Case-Fatality Risk Estimates for COVID-19 Calculated by Using a Lag Time for Fatality. Emerg. Infect. Dis. 2020, 26, 1339–1441. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, M.R. Theory and Problems of Probability and Statistics; McGraw-Hill: New York, NY, USA, 1992; pp. 116–117. [Google Scholar]
- Geoghegan, J.L.; Holmes, E.C. The phylogenomics of evolving virus virulence. Nat. Rev. Genet. 2018, 19, 756–769. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Li, W.; Xie, J.; Hou, Y.; You, C. Cytokine storm induced by sars-cov-2. Clin. Chim. Acta 2020, 509, 280–287. [Google Scholar] [CrossRef]
- Young, B.E.; Fong, S.W.; Chan, Y.-H.; Mak, T.-M.; Ang, L.W.; Anderson, D.E.; Lee, C.Y.-P.; Amrun, S.N.; Lee, B.; Goh, Y.S.; et al. Effects of a major deletion in the SARS-CoV-2 genome on the severity of infection and the inflammatory response: An observational cohort study. Lancet 2020, 396, 603–611. [Google Scholar] [CrossRef]
- Benedetti, F.; Snyder, G.; Giovanetti, M.; Angeletti, S.; Gallo, R.; Ciccozzi, M.; Zella, D. Emerging of a SARS-CoV-2 viral strain with a deletion in nsp1. J. Transl. Med. 2020, 18, 1–6. [Google Scholar] [CrossRef]
- Fishman, D.N. Seasonality of infectious diseases. Annu. Rev. Public Health 2007, 28, 127–143. [Google Scholar] [CrossRef]
- Iikuni, N.; Nakajima, A.; Inoue, E.; Tanaka, E.; Okamoto, H.; Hara, M.; Tomatsu, T.; Kamatani, N.; Yamanaka, H. What’s in season for rheumatoid arthritis patients? Seasonal fluctuations in disease activity. Rheumatology 2007, 46, 846–848. [Google Scholar] [CrossRef]
- Moltchanova, E.V.; Schreier, N.; Lammi, N.; Karvonen, M. Seasonal variation of diagnosis of Type 1 diabetes mellitus in children worldwide. Diabet. Med. 2009, 26, 673–678. [Google Scholar] [CrossRef]
- Dopico, X.C.; Evangelou, M.; Ferreira, R.C.; Guo, H.; Pekalski, M.L.; Smyth, D.J.; Cooper, N.; Burren, O.S.; Fulford, A.J.; Hennig, B.J.; et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nat. Commun. 2015, 6, 7000. [Google Scholar] [CrossRef]
- Scafetta, N. Distribution of the SARS-CoV-2 Pandemic and Its Monthly Forecast Based on Seasonal Climate Patterns. Int. J. Environ. Res. Public Health 2020, 17, 3493. [Google Scholar] [CrossRef] [PubMed]
- Carleton, T.; Meng, K.C. Causal empirical estimates suggest COVID-19 transmission rates are highly seasonal. medRxiv 2020. [Google Scholar] [CrossRef]
- Cannell, J.J.; Vieth, R.; Umhau, J.C.; Holick, M.F.; Grant, W.B.; Madronich, S.; Garland, C.F.; Giovannucci, E. Epidemic influenza and vitamin D. Epidemiol. Infect. 2006, 134, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Moozhipurath, R.K.; Kraft, L.; Skiera, B. Evidence of protective role of Ultraviolet-B (UVB) radiation in reducing COVID-19 deaths. Sci. Rep. 2020, 10, 17705. [Google Scholar] [CrossRef]
- Ratnesar-Shumate, S.; Williams, G.; Green, B.; Krause, M.; Holland, B.; Wood, S.; Bohannon, J.; Boydston, J.; Freeburger, D.; Hooper, I.; et al. Simulated Sunlight Rapidly Inactivates SARS-CoV-2 on Surfaces. J. Infect. Dis. 2020, 222, 214–222. [Google Scholar] [CrossRef]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef]
- Fountoulakis, I.; Diémoz, H.; Siani, A.-M.; Laschewski, G.; Filippa, G.; Arola, A.; Bais, A.F.; De Backer, H.; Lakkala, K.; Webb, A.R.; et al. Solar UV Irradiance in a Changing Climate: Trends in Europe and the Significance of Spectral Monitoring in Italy. Environments 2020, 7, 1. [Google Scholar] [CrossRef]
- ISS COVID-19 Integrated Surveillance Data in Italy. 2020. Available online: https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-dashboard (accessed on 26 October 2020). (In English).
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Ministero Della Salute, Weekly Monitoring Covid-19, Report 3–9 August. 2020. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp?lingua=italiano&menu=notizie&p=dalministero&id=5021 (accessed on 28 October 2020). (In English)
- Weir, E.K.; Thenappan, T.; Bhargava, M.; Chen, Y. Does vitamin D deficiency increase the severity of COVID-19? Clin. Med. 2020, 20, e107–e108. [Google Scholar] [CrossRef]
- Hernández, J.L.; Nan, D.; Fernandez-Ayala, M.; García-Unzueta, M.; Hernández-Hernández, M.A.; López-Hoyos, M.; Muñoz-Cacho, P.; Olmos, J.M.; Gutiérrez-Cuadra, M.; Ruiz-Cubillán, J.J.; et al. Vitamin D Status in Hospitalized Patients with SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2020, dgaa733. [Google Scholar] [CrossRef]
- INFN, Gruppo di Lavoro CovidStat INFN. 2020. Available online: https://covid19.infn.it/mappa_nazionale/htmlFiles/complexDashboard_2020-10-25.html?theme=classic (accessed on 26 October 2020). (In Italian).
- John Hopking University, Corona Virus Resource Centre. 2020. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 26 October 2020). (In English).
- Ficetola, G.F.; Rubolini, D. Climate affects global patterns of COVID-19 early outbreak dynamics. medRxiv 2020. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
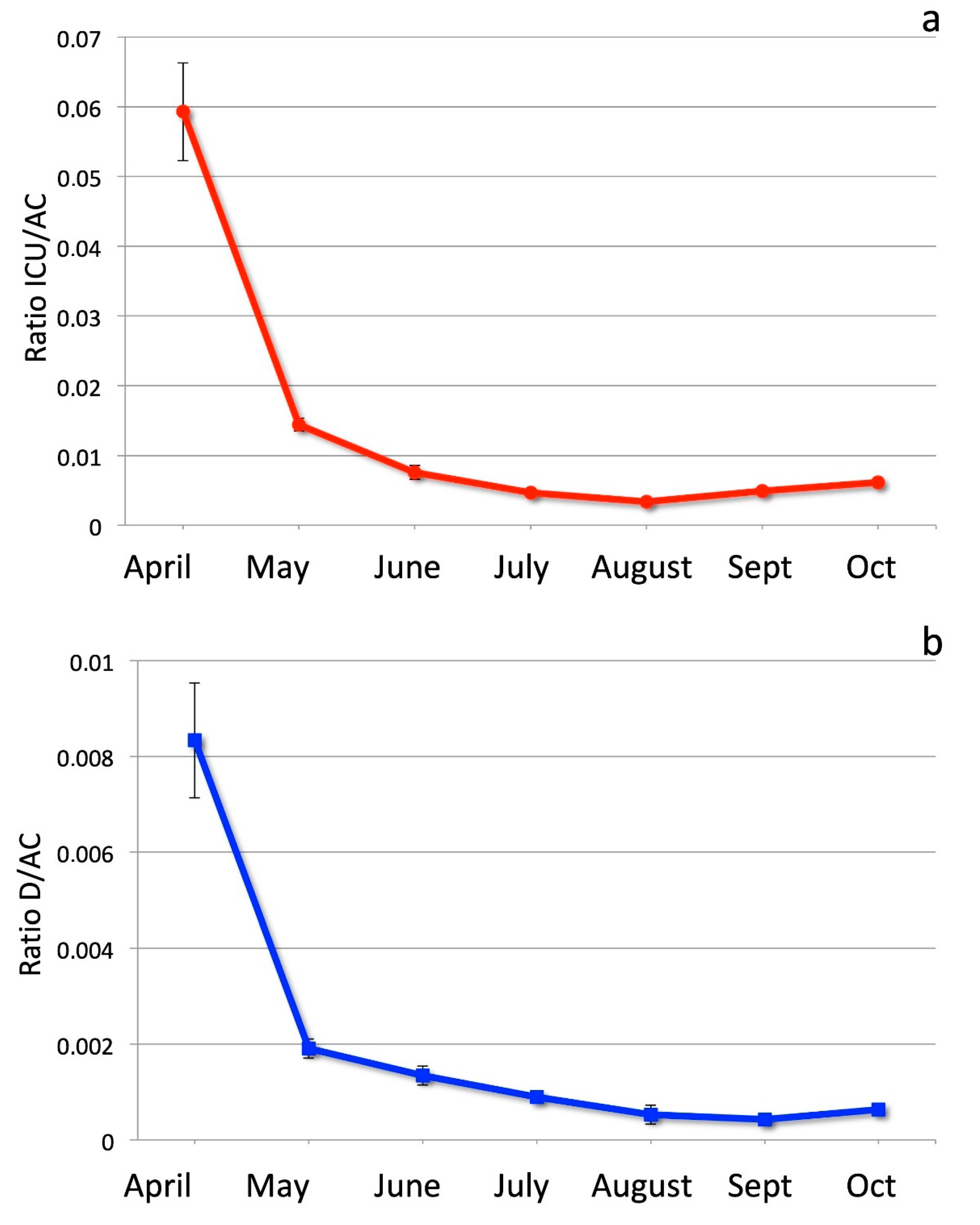
| Month | Ratio ICU/AC | Ratio D/AC |
|---|---|---|
| April | 0.0593 ± 0.0068 | 0.0083 ± 0.0012 |
| May | 0.0144 ± 0.0008 | 0.0019 ± 0.0008 |
| June | 0.0076 ± 0.0016 | 0.0013 ± 0.0002 |
| July | 0.0046 ± 0.0004 | 0.0009 ± 0.0001 |
| August | 0.00334 ± 0.00006 | 0.0005 ± 0.0002 |
| September | 0.0049 ± 0.0006 | 0.00042 ± 0.0001 |
| October | 0.0061 ± 0.0003 | 0.00063 ± 0.0001 |
| Relative Ratio ICU/AC | Relative Ratio D/AC | |
|---|---|---|
| April/May | 4.11 ± 0.54 | 4.37 ± 0.84 |
| April/June | 7.8 ± 1.4 | 6.2 ± 1.3 |
| April/July | 12.7 ± 1.9 | 9.3 ± 1.8 |
| April/August | 17.8 ± 2.1 | 15.8 ± 3.5 |
| April/September | 12.0 ± 2.0 | 19.7 ± −4.0 |
| April/October | 9.7 ± 1.2 | 13.2 ± −3.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Natale, G.; De Natale, L.; Troise, C.; Marchitelli, V.; Coviello, A.; Holmberg, K.G.; Somma, R. The Evolution of Covid-19 in Italy after the Spring of 2020: An Unpredicted Summer Respite Followed by a Second Wave. Int. J. Environ. Res. Public Health 2020, 17, 8708. https://doi.org/10.3390/ijerph17238708
De Natale G, De Natale L, Troise C, Marchitelli V, Coviello A, Holmberg KG, Somma R. The Evolution of Covid-19 in Italy after the Spring of 2020: An Unpredicted Summer Respite Followed by a Second Wave. International Journal of Environmental Research and Public Health. 2020; 17(23):8708. https://doi.org/10.3390/ijerph17238708
Chicago/Turabian StyleDe Natale, Giuseppe, Lorenzo De Natale, Claudia Troise, Vito Marchitelli, Antonio Coviello, Karen G. Holmberg, and Renato Somma. 2020. "The Evolution of Covid-19 in Italy after the Spring of 2020: An Unpredicted Summer Respite Followed by a Second Wave" International Journal of Environmental Research and Public Health 17, no. 23: 8708. https://doi.org/10.3390/ijerph17238708
APA StyleDe Natale, G., De Natale, L., Troise, C., Marchitelli, V., Coviello, A., Holmberg, K. G., & Somma, R. (2020). The Evolution of Covid-19 in Italy after the Spring of 2020: An Unpredicted Summer Respite Followed by a Second Wave. International Journal of Environmental Research and Public Health, 17(23), 8708. https://doi.org/10.3390/ijerph17238708