Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures and Outcome
2.3. Analysis
3. Results
3.1. Profile of Women Having a High Risk of Depression
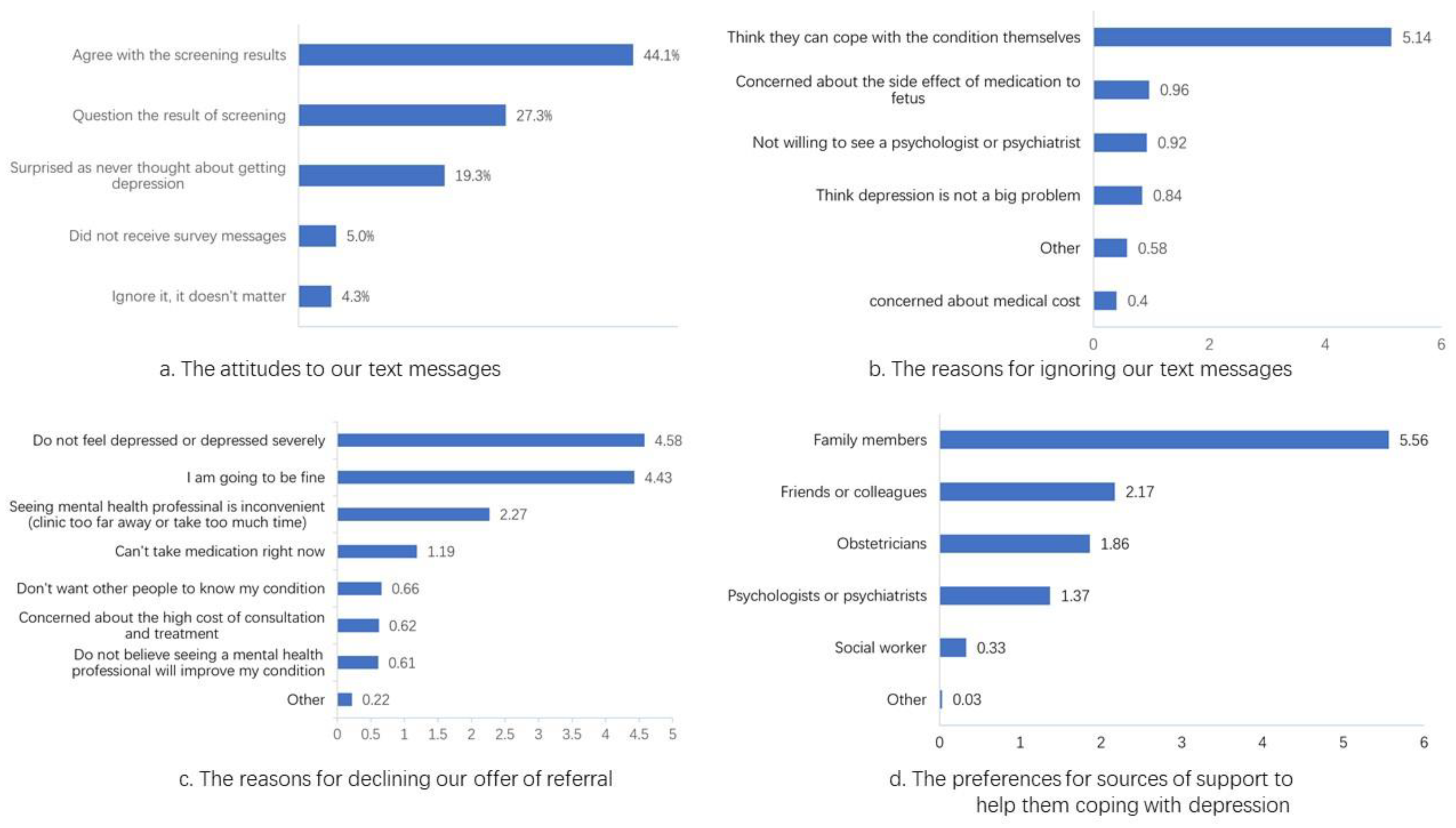
3.2. Responses to Referral
3.3. Reasons for not Accepting Referrals
3.4. Preference for Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| EPDS Scores | High-Risk Women (n = 248) | Other Women in Cohort (n = 878) |
|---|---|---|
| Half year after delivery | ||
| >12.5 | 42 (34.43%) | 19 (5.85%) |
| <12.5 | 80 (65.57%) | 306 (94.15%) |
| missing | 126 (50.80%) | 553 (63.98%) |
| One year after delivery | ||
| >12.5 | 26 (23.42%) | 11 (3.48%) |
| <12.5 | 85 (76.58%) | 305 (96.52%) |
| missing | 137 (55.24%) | 562 (64.00%) |
References
- General Office of the National Health Commission. Notice of the General Office of the National Health Commission on Exploring the Implementation of Special Services for the Prevention and Treatment of Depression and Senile Dementia. Available online: http://www.nhc.gov.cn/jkj/s7914/202009/a63d8f82eb53451f97217bef0962b98f.shtml (accessed on 3 October 2020).
- Fisher, J.; Mello, M.C.D.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: A systematic review. Bull. World Health Organ. 2012, 90, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Nisar, A.; Yin, J.; Waqas, A.; Bai, X.; Wang, D.; Rahman, A.; Li, X. Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 1022–1037. [Google Scholar] [CrossRef] [PubMed]
- Plant, D.T.; Pariante, C.M.; Sharp, D.; Pawlby, S. Maternal depression during pregnancy and offspring depression in adulthood: Role of child maltreatment. Br. J. Psychiatry 2015, 207, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Corman, H.; Curtis, M.A.; Noonan, K.; Reichman, N.E. Maternal depression as a risk factor for children’s inadequate housing conditions. Soc. Sci. Med. 2016, 149, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Davalos, D.B.; Yadon, C.A.; Tregellas, H.C. Untreated prenatal maternal depression and the potential risks to offspring: A review. Arch. Women’s Ment. Health 2012, 15, 1–14. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Mental Health. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance: Updated Edition; British Psychological Society: Leicester, UK, 2014. [Google Scholar]
- American College of Obstetricians and Gynecologists. Screening for depression during and after pregnancy. Committee Opinion No. 453. Obstet. Gynecol. 2010, 115, 394–395. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for depression in adults: US Preventive Services Task Force recommendation statement. JAMA-J. Am. Med Assoc. 2016, 315, 380–387. [Google Scholar] [CrossRef]
- Austin, M.-P.; Highet, N. Guidelines Expert Advisory Committee. Clinical practice guidelines for depression and related disorders—anxiety, bipolar disorder and puerperal psychosis—In the perinatal period. In A Guideline for Primary Care Health Professionals; Beyondblue: The National Depression Initiative: Melbourne, Australia, 2013. [Google Scholar]
- Myers, E.; Aubuchon-Endsley, N.; Bastian, L.; Gierisch, J.; Kemper, A.; Swamy, G. Efficacy and Safety of Screening for Postpartum Depression; Comparative Effectiveness Review No. 106; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013.
- Hickie, I. Beyondblue: The national depression initiative. Australas. Psychiatry 2001, 9, 147–150. [Google Scholar] [CrossRef]
- Byatt, N.; Levin, L.L.; Ziedonis, D.; Simas, T.A.M.; Allison, J. Enhancing participation in depression care in outpatient perinatal care settings: A systematic review. Obstet. Gynecol. 2015, 126, 1048. [Google Scholar] [CrossRef]
- Xue, W.Q.; Cheng, K.K.; Xu, D.; Jin, X.; Gong, W.J. Uptake of referrals for women with positive perinatal depression screening results and the effectiveness of interventions to increase uptake: A systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2020, 29, e143. [Google Scholar] [CrossRef]
- Zhang, Y. Population Growth Slowed and Urbanization Continued to Improve. Available online: http://www.stats.gov.cn/tjsj/zxfb/202001/t20200119_1723767.html (accessed on 3 October 2020).
- Ming, G.; Zhihui, W.; Xiaohong, F. Application value of the 9-question depression scale from the patient health questionnaire in the screening of postpartum depression. China Mod. Med. 2019, 26, 104–106. [Google Scholar]
- Wong, J.; Fisher, J. The role of traditional confinement practices in determining postpartum depression in women in Chinese cultures: A systematic review of the English language evidence. J. Affect. Disord. 2009, 116, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, E.; Katie, F.K.L.; Chun, L.S.; Ha, S.W. “Doing the month”: An exploration of postpartum practices in Chinese women. Health Care Women Int. 1997, 18, 301–313. [Google Scholar] [CrossRef] [PubMed]
- XIE, R.H.; Yang, J.; Liao, S.; Xie, H.; Walker, M.; Wen, S.W. Prenatal family support, postnatal family support and postpartum depression. Aust. N. Z. J. Obstet. Gynaecol. 2010, 50, 340–345. [Google Scholar] [CrossRef]
- Yu, M.; Li, H.; Xu, D.R.; Wu, Y.; Liu, H.; Gong, W. Trajectories of perinatal depressive symptoms from early pregnancy to six weeks postpartum and their risk factors-a longitudinal study. J Affect Disord 2020, 275, 149–156. [Google Scholar] [CrossRef]
- Fabbris, L. Measurement scales for scoring or ranking sets of interrelated items. In Survey Data Collection and Integration; Springer: Berlin/Heidelberg, Germany, 2013; pp. 21–43. [Google Scholar]
- Wenjuanxing. Rule of Points for Sorting Questions. Available online: https://www.wjx.cn/help/help.aspx?helpid=43 (accessed on 3 October 2020).
- Guo, X.; Wang, Y.; Chen, J. Study on the efficacy of the Edinburgh postnatal depression scale in puerperas in Chengdu. Chin. J. Pract. Nurs. 2009, 25, 4–6. [Google Scholar]
- Lee, D.T.; Yip, S.K.; Chiu, H.F.; Leung, T.Y.; Chan, K.P.; Chau, I.O.; Leung, H.C.; Chung, T.K. Detecting postnatal depression in Chinese women. Validation of the Chinese version of the Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1998, 172, 433–437. [Google Scholar] [CrossRef]
- Zhang, H.-M.; Xu, Y.; Li, Y.-Y.; Wu, A.-Q. The Infuences Caused by Life Events, Social Support, Personality Agent and Antepartum Mental Stale on the Postpartum Depression. Chin. J. Prev. Control Chronic Non-Commun. Dis. 2007, 15, 321–325. [Google Scholar]
- Zhang, L.; Li, Y.-H.; Bu, Y.-G.; Guan, H.; Liao, P.-P. Dynamic observation of female perinatal depression and study on the related factors. Matern. Child Health Care China 2015, 30, 2393–2397. [Google Scholar]
- Zhong, B.-L.; Cui, J.; Chen, H.-H.; Zhang, J.-F.; Xu, H.-M.; Fan, Y.-P.; Wang, P.-H.; Zhou, L. Investigation of Postpartum Depression Among Medical Staff From 21 Maternal and Child Care Ceters in Wuhan: A Cross-Sectional Survey. Chin. J. Obstet. Gynecol. Pediatr. 2011, 7, 12–15. [Google Scholar]
- National Health Commission of China. Yearbook of China Health Statistics; Peking Union Medical College Press: Beijing, China, 2019.
- Goodman, J.H.; Tyer-Viola, L. Detection, treatment, and referral of perinatal depression and anxiety by obstetrical providers. J. Womens Health 2010, 19, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.M.; Flynn, H.A.; Blow, F.C.; Barry, K.L. Depressive symptoms among pregnant women screened in obstetrics settings. J. Womens Health 2003, 12, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Bauer, N.S.; Ofner, S.; Pottenger, A.; Carroll, A.E.; Downs, S.M. Follow-up of Mothers with Suspected Postpartum Depression from Pediatrics Clinics. Front. Pediatr. 2017, 5, 212. [Google Scholar] [CrossRef] [PubMed]
- Honikman, S.; van Heyningen, T.; Field, S.; Baron, E.; Tomlinson, M. Stepped care for maternal mental health: A case study of the perinatal mental health project in South Africa. PLoS Med. 2012, 9, e1001222. [Google Scholar] [CrossRef]
- Kim, J.J.; La Porte, L.M.; Corcoran, M.; Magasi, S.; Batza, J.; Silver, R.K. Barriers to mental health treatment among obstetric patients at risk for depression. Am. J. Obstet. Gynecol. 2010, 202, 312.e1–312.e5. [Google Scholar] [CrossRef]
- Milgrom, J.; Holt, C.J.; Gemmill, A.W.; Ericksen, J.; Leigh, B.; Buist, A.; Schembri, C. Treating postnatal depressive symptoms in primary care: A randomised controlled trial of GP management, with and without adjunctive counselling. BMC Psychiatry 2011, 11, 95. [Google Scholar] [CrossRef]
- Miller, L.S.; Boyd, B.J.; Chernov, A.J. Improving the identification and treatment of postpartum depression in a managed care organization. J. Clin. Outcomes Manag. 2004, 11, 157–161. [Google Scholar]
- Miller, L.; Shade, M.; Vasireddy, V. Beyond screening: Assessment of perinatal depression in a perinatal care setting. Arch. Womens Ment. Health 2009, 12, 329–334. [Google Scholar] [CrossRef]
- Trost, M.J.; Molas-Torreblanca, K.; Man, C.; Casillas, E.; Sapir, H.; Schrager, S.M. Screening for maternal postpartum depression during infant hospitalizations. J. Hosp. Med. 2016, 11, 840–846. [Google Scholar] [CrossRef]
- Chen, H.; Wang, J.; Ch’ng, Y.C.; Mingoo, R.; Lee, T.; Ong, J. Identifying mothers with postpartum depression early: Integrating perinatal mental health care into the obstetric setting. ISRN Obstet. Gynecol. 2011, 2011, 309189. [Google Scholar] [CrossRef]
- Robinson, S.; Young, J. Screening for depression and anxiety in the post-natal period: Acceptance or rejection of a subsequent treatment offer. Aust. N. Z. J. Psychiatry 1982, 16, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.T.; Pun, P.K.K. Analysis of positive Edinburgh depression scale referrals to a consultation liaison psychiatry service in a two-year period. Int. J. Ment. Health Nurs. 2007, 16, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Rowan, P.; Greisinger, A.; Brehm, B.; Smith, F.; McReynolds, E. Outcomes from implementing systematic antepartum depression screening in obstetrics. Arch. Women’s Ment. Health 2012, 15, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Price, S.K.; Coles, D.C.; Wingold, T. Integrating Behavioral Health Risk Assessment into Centralized Intake for Maternal and Child Health Services. Health Soc. Work 2017, 42, 231–240. [Google Scholar] [CrossRef]
- Reay, R.; Matthey, S.; Ellwood, D.; Scott, M. Long-term outcomes of participants in a perinatal depression early detection program. J. Affect. Disord. 2011, 129, 94–103. [Google Scholar] [CrossRef]
- Lei, X.; Liu, L.; Li, D. The depression of chinese and the reflection related to their society and culture. Chin. Gen. Pract. 2004, 7, 315–317. [Google Scholar]
- Chen, A.W.; Kazanjian, A.; Wong, H. Why do Chinese Canadians not consult mental health services: Health status, language or culture? Transcult. Psychiatry 2009, 46, 623–641. [Google Scholar] [CrossRef]
- Kung, W.W. Cultural and practical barriers to seeking mental health treatment for Chinese Americans. J. Community Psychol. 2004, 32, 27–43. [Google Scholar] [CrossRef]
- Tabora, B.L.; Flaskerud, J.H. Mental Health Beliefs, Practices, and Knowledge of Chinese American Immigrant Women. Issues Ment. Health Nurs. 1997, 18, 173–189. [Google Scholar] [CrossRef]
- Ying, Y.-W.; Miller, L.S. Help-seeking behavior and attitude of Chinese Americans regarding psychological problems. Am. J. Community Psychol. 1992, 20, 549–556. [Google Scholar] [CrossRef]
- Byatt, N.; Simas, T.A.; Lundquist, R.S.; Johnson, J.V.; Ziedonis, D.M. Strategies for improving perinatal depression treatment in North American outpatient obstetric settings. J. Psychosom. Obstet. Gynaecol. 2012, 33, 143–161. [Google Scholar] [CrossRef] [PubMed]
- Abe-Kim, J.; Takeuchi, D.; Hwang, W.-C. Predictors of help seeking for emotional distress among Chinese Americans: Family matters. J. Consult. Clin. Psychol. 2002, 70, 1186. [Google Scholar] [CrossRef]
- Liu, Y.Q.; Petrini, M.; Maloni, J.A. “Doing the month”: Postpartum practices in Chinese women. Nurs. Health Sci. 2015, 17, 5–14. [Google Scholar] [CrossRef]
- Ding, G.; Yu, J.; Vinturache, A.; Gu, H.; Lu, M. Therapeutic Effects of the Traditional “Doing the Month” Practices on Postpartum Depression in China. Am. J. Psychiatry 2018, 175, 1071–1072. [Google Scholar] [CrossRef]


| Variable | High Risk Women (n = 248) | Other Women in Cohort (n = 878) | p |
|---|---|---|---|
| Age (years) | 0.905 | ||
| <25 | 37 (15.04%) | 120 (13.89%) | |
| 25–30 | 139 (56.50%) | 480 (55.56%) | |
| 30–35 | 51 (20.73%) | 188 (21.76%) | |
| >35 | 19 (7.72%) | 76 (8.80%) | |
| Average | 28.28 | 28.83 | |
| Missing | 2 | 14 | |
| Parity | 0.806 | ||
| Primiparas | 64 (25.91%) | 229 (26.97%) | |
| Multiparas | 183 (74.09%) | 620 (73.03%) | |
| Missing | 1 | 29 | |
| Education | 0.891 | ||
| Middle school graduate or less | 31 (12.60%) | 96 (11.03%) | |
| High school | 58 (23.58%) | 200 (22.99%) | |
| College degree | 136 (55.28%) | 501 (57.59%) | |
| Graduate or professional degree | 21 (8.54%) | 73 (8.39%) | |
| Missing | 2 | 8 | |
| Jobs | 0.900 | ||
| Government workers | 51 (21.07%) | 185 (21.46%) | |
| Enterprise managers | 43 (17.77%) | 151 (17.52%) | |
| Private business owner | 31 (12.81%) | 136 (15.78%) | |
| Workers/Farmers | 11 (4.55%) | 39 (4.52%) | |
| Unemployed (due to disease or other reasons) | 66 (27.27%) | 214 (24.83%) | |
| Others | 40 (16.53%) | 137 (15.89%) | |
| Missing | 6 | 16 | |
| Income per month | 0.471 | ||
| 0 | 69 (28.28%) | 236 (27.73%) | |
| ¥1–2000 | 12 (4.92%) | 53 (6.23%) | |
| ¥2001–5000 | 122 (50.00%) | 389 (45.71%) | |
| Over ¥5001 | 41 (16.80%) | 173 (20.33%) | |
| Missing | 4 | 27 | |
| Depression history | 0.005 ** | ||
| No | 164 (93.18%) | 609 (97.91%) | |
| Yes | 12 (6.82%) | 13 (2.09%) | |
| Missing | 72 | 256 | |
| Living Situation | 0.233 | ||
| Nuclear family | 87 (35.80%) | 375 (43.20%) | |
| Nuclear family and parents in law | 91 (37.45%) | 296 (34.10%) | |
| Nuclear family and parents | 40 (16.46%) | 107 (12.33%) | |
| Living alone | 20 (8.23%) | 71 (8.18%) | |
| Else | 5 (2.06%) | 19 (2.19%) | |
| Missing | 5 | 10 | |
| Relationship with spouse | <0.001 *** | ||
| Satisfied | 174 (71.90%) | 731 (84.12%) | |
| Somewhat satisfied | 65 (26.86%) | 136 (15.56%) | |
| Dissatisfied | 2 (1.24%) | 2 (0.23%) | |
| Missing | 7 | 9 | |
| Family’s wishes about child’s sex | 0.041 * | ||
| Boy | 44 (18.11%) | 106 (12.24%) | |
| Girl | 32 (13.17%) | 103 (11.89%) | |
| Does not matter | 167 (68.72%) | 657 (75.87%) | |
| Missing | 5 | 12 | |
| Willingness to do the month | 0.018 * | ||
| Yes | 207 (85.19%) | 786 (90.66%) | |
| No | 36 (14.81%) | 81 (9.34%) | |
| Missing | 5 | 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, W.; Jin, X.; Cheng, K.K.; Caine, E.D.; Lehman, R.; Xu, D. Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. Int. J. Environ. Res. Public Health 2020, 17, 8686. https://doi.org/10.3390/ijerph17228686
Gong W, Jin X, Cheng KK, Caine ED, Lehman R, Xu D. Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. International Journal of Environmental Research and Public Health. 2020; 17(22):8686. https://doi.org/10.3390/ijerph17228686
Chicago/Turabian StyleGong, Wenjie, Xin Jin, Kar Keung Cheng, Eric D. Caine, Richard Lehman, and Dong (Roman) Xu. 2020. "Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression" International Journal of Environmental Research and Public Health 17, no. 22: 8686. https://doi.org/10.3390/ijerph17228686
APA StyleGong, W., Jin, X., Cheng, K. K., Caine, E. D., Lehman, R., & Xu, D. (2020). Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. International Journal of Environmental Research and Public Health, 17(22), 8686. https://doi.org/10.3390/ijerph17228686