Lupus Erythematosus Quality of Life Questionnaire (LEQoL): Development and Psychometric Properties



Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Data Collection
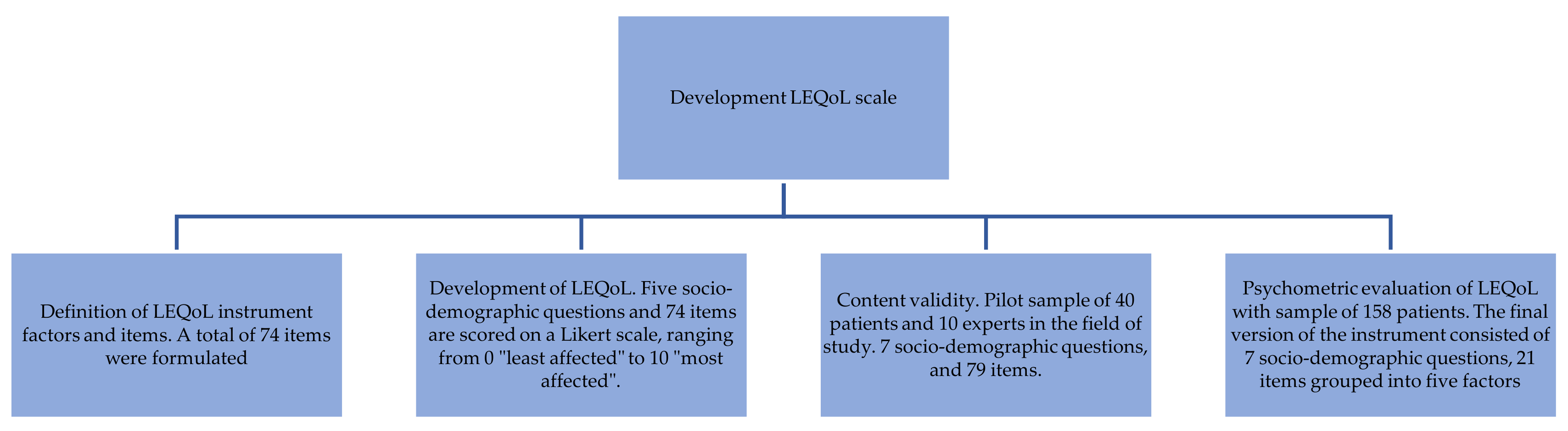
2.1.1. (Phase 1) Definition of Quality of Life of Patients with Lupus Erythematosus Instrument (LEQoL) Factors and Items
2.1.2. (Phase 2) Development of LEQoL
2.1.3. (Phase 3) Content Validity
2.1.4. (Phase 4) Psychometric Evaluation of LEQoL
2.2. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Psychometric Evaluation of the Scale in the Final Sample of Patients
3.2.1. Validity Analysis
3.2.2. Exploratory Factorial Analysis (EFA)
3.2.3. Confirmatory Factorial Analysis (CFA)
3.2.4. Item Analysis
3.2.5. Reliability Analysis
3.3. Quality of Life Level in the Sample of Patients
3.4. Percentiles of LEQoL Interpretation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Spanish Version | English Version |
|---|---|
| Factor Físico ¿En qué medida le afecta el cansancio con la pérdida de fuerzas para seguir realizando una tarea? (11) ¿Cuánto le afecta el cansancio al tiempo que le dedica a su trabajo/estudios al día? (12) ¿Cuánta ayuda necesita para realizar tareas del día a día, por ejemplo, cocinar, mover una mesa o subir escaleras? (13) ¿Valorándolo de 0 a 10, el dolor le impide hacer alguna actividad cotidiana de las que haría normalmente, como por ejemplo, hacer deporte, ir a trabajar, ir a estudiar…? (14) ¿En qué medida afecta su enfermedad a que sienta dolor en alguna parte de su cuerpo? (24) ¿Se siente muy, muy cansado en algún momento del día? (26) | Physical Factor To what extent does fatigue affect the loss of strength to carry out a task? (11) How much does fatigue affect your work/study time each day? (12) How much help do you need to perform day-to-day tasks, such as cooking, moving a table or climbing stairs? (13) On a scale from 0 to 10, does pain prevent you from doing any of the normal daily activities you would normally do, such as sports, going to work, or going to school? (14) To what extent does your illness affect your ability to feel pain in any part of your body? (24) Do you feel very, very tired at any point during the day? (26) |
| Factor apariencia ¿Dedica mucho tiempo en disimular sus problemas físicos causados por su enfermedad? (43) ¿Si ha ganado o perdido peso, cuánto le afecta en su imagen? (44) ¿En qué medida le importa lo que piensen los demás de su aspecto físico? (45) ¿En qué medida le afecta a usted su apariencia física? (46) ¿Cuánto podría influirle su enfermedad para que se quedara en casa sin salir por su apariencia física? (48) | Appearance factor Do you spend a lot of time covering up physical problems caused by your illness? (43) If you have gained or lost weight, how much does it affect your image? (44) To what extent do you care what others think about your physical appearance? (45) To what extent does your physical appearance affect you? (46) How much could your illness influence you to stay home without leaving because of your physical appearance? (48) |
| Factor emociones ¿Podría decirme de 0 a 10 cuánta culpa tiene su enfermedad en que se sienta enfadado? (29a) ¿Podría decirme de 0 a 10 cuánta culpa tiene su enfermedad en que se sienta resentido? (29b) ¿Podría decirme de 0 a 10 cuánta culpa tiene su enfermedad en que se sienta triste? (29c) ¿Podría decirme de 0 a 10 cuánta culpa tiene su enfermedad en que se sienta ansioso? (29d) | Emotional factors Can you tell me from 0 to 10 how much your illness has made you feel angry? (29a) Could you tell me from 0 to 10 how much your illness has caused you to feel resentful? (29b) Can you tell me from 0 to 10 how much your illness has made you feel sad? (29c) Can you tell me from 0 to 10 how much your illness has made you feel anxious? (29d) |
| Factor cognición ¿Cree que afecta a su concentración? ¿En qué medida? (39) ¿En qué medida cree que su enfermedad afecta a su memoria? (40) ¿Tiene que hacer las cosas más lentamente a causa de su enfermedad? ¿En qué medida? (42) | Cognition factor Do you think your illness affects your concentration? To what extent? (39) To what extent do you think your illness affects your memory? (40) Do you have to do things more slowly because of your illness? To what extent? (42) |
| Factor relaciones ¿Cuánto influye su enfermedad a la hora de relacionarse con su pareja? (62) ¿Cuánto influye su enfermedad a la hora de relacionarse con los miembros de su familia? (63) ¿Tiene problemas con su pareja, amigos o familiares a causa de su enfermedad? ¿En qué medida? (66) | Relationship factor How much does your illness influence your relationship with your partner? (62) How much does your illness influence your relationship with family members? (63) Do you have problems with your partner, friends or family because of your illness? To what extent? (66) |
References
- Walling, H.W.; Sontheimer, R.D. Cutaneous lupus erythematosus. Am. J. Clin. Dermatol. 2009, 10, 365–381. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R.; Khamastha, M.; Huges, G. The Euro Lupus Project: Epidemiology of systemic lupus erythematosus in Europe. Lupus 2009, 18, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Gronhagen, C.; Nyberg, F. Cutaneous Lupus erithematosus: An update. Indian Dermatol. 2014, 5, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Roper, G.F.K. Lupus Awareness Survey for the Lupus Foundation of America [Executive Summary Report]; GfK Roper Public Affairs & Corporate Communications: Washington, DC, USA, 2012. [Google Scholar]
- Rees, F.; Doherty, M.; Grainge, M.J.; Lanyon, P.; Zhang, W. The worldwide incidence and prevalence of systemic lupus erythematosus: A systematic review of epidemiological studies. Rheumatology 2017, 56, 1945–1961. [Google Scholar] [CrossRef]
- Wolfe, F.; Michaud, K.; Li, T.; Katz, R.S. Chronic Conditions and Health Problems in Rheumatic Diseases: Comparisons with Rheumatoid Arthritis, Noninflammatory Rheumatic Disorders, Systemic Lupus Erythematosus, and Fibromyalgia. J. Rheumatol. 2010, 37, 305–315. [Google Scholar] [CrossRef]
- Compas, B.E.; Jaser, S.S.; Dunn, M.J.; Rodriguez, E.M. Coping with Chronic Illness in Childhood and Adolescence. Annu. Rev. Clin. Psychol. 2012, 8, 455–480. [Google Scholar] [CrossRef]
- Krasselt, M.; Baerwald, C. Sex, Symptom Severity, and Quality of Life in Rheumatology. Clin. Rev. Allergy Immunol. 2019, 56, 346–361. [Google Scholar] [CrossRef]
- Cervera, R.; Rúa-Figueroa, I.; Gil-Aguado, A.; Sabio, J.; Pallarés, L.; Hernández-Pastor, L.; Iglesias, M. Direct cost of management and treatment of active systemic lupus erythematosus and its flares in Spain: The LUCIE Study. Rev. Clin. Esp. 2013, 213, 127–137. [Google Scholar] [CrossRef]
- Schulman-Green, D.; Jaser, S.; Martin, F.; Alonzo, A.; Grey, M.; McCorkle, R.; Redeker, N.S.; Reynolds, N.; Whittemore, R. Processes of Self-Management in Chronic Illness. J. Nurs. Sch. 2012, 44, 136–144. [Google Scholar] [CrossRef]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Aberer, E. Epidemiologic, socioeconomic and psychosocial aspects in lupus erythematosus. Lupus 2010, 19, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- McElhone, K.; Abbott, J.; Teh, L.-S. A review of health related quality of life in systemic lupus erythematosus. Lupus 2006, 15, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Meenaskshi, J.; Pickard, A.; Wilke, C.; Lin, H.; Khandelwal, S.; Rodby, R. Development and validation of a US Lupus Specific Patient Reported Outcome Measure. Arthritis Rheum. 2007, 56, 59–69. [Google Scholar]
- Wahie, S.; McColl, E.; Reynolds, N.; Meggitt, S. Measuring disease activity and damage in discoid lupus erythematosus. Br. J. Dermatol. 2010, 162, 1030–1037. [Google Scholar] [CrossRef]
- Laschinger, H.K.S.; Hall, L.M.; Pedersen, C.; Almost, J. A Psychometric Analysis of the Patient Satisfaction with Nursing Care Quality Questionnaire. J. Nurs. Care Qual. 2005, 20, 220–230. [Google Scholar] [CrossRef]
- Wagner, D.; Bear, M. Patient satisfaction with nursing care: A concept analysis within a nursing framework. J. Adv. Nurs. 2009, 265, 692–701. [Google Scholar] [CrossRef]
- Whitehead, D. Health education, behavioural change and social psychology: Nursing’s contribution to health promotion? J. Adv. Nurs. 2001, 34, 822–832. [Google Scholar] [CrossRef]
- Pender, N.; Murdaugh, C.; Parsons, M. Health Promotion in Nursing Practice, 6th ed.; Prentice-Hall Health: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Leino-Kilpi, H.; Johansson, K.; Heikkinen, K.; Kaljonen, A.; Virtanen, H.; Salanterä, S. Patient Education and Health-related Quality of Life. J. Nurs. Care Qual. 2005, 20, 307–316. [Google Scholar] [CrossRef]
- Warrington, D.; Cholowski, K.; Peters, D. Effectiveness of home-based cardiac rehabilitation for special needs patients. J. Adv. Nurs. 2003, 41, 121–129. [Google Scholar] [CrossRef]
- Bombardier, C.; Gladman, D.D.; Urowitz, M.B.; Caron, D.; Chang, C.H.; Austin, A.; Bell, A.; Bloch, D.A.; Corey, P.N.; Decker, J.L.; et al. Derivation of the sledai. A disease activity index for lupus patients. Arthritis Rheum. 1992, 35, 630–640. [Google Scholar] [CrossRef]
- Albrecht, J.; Werth, V. Development of the CLASI as an outcome instrument for cutaneous lupus erythematosus. Dermatol. Ther. 2007, 20, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.; Khan, G. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Grootscholten, C.; Ligtenberg, G.; Derksen, R.H.W.M.; Schreurs, K.M.G.; De Glas-Vos, J.W.; Hagen, E.C.; Bake, A.W.L.V.D.W.; Huizinga, T.W.J.; Hoogen, F.H.J.V.D.; Bijl, M.; et al. Health-related quality of life in patients with systemic lupus erythematosus: Development and validation of a lupus specific symptom checklist. Qual. Life Res. 2003, 12, 635–644. [Google Scholar] [CrossRef]
- Moorthy, L.; Peterson, M.G.E.; Baratelli, M.; Harrison, M.J.; Onel, K.B.; Chalom, E.C.; Haines, K.; Hashkes, P.J.; Lehman, T.J.A. Multicenter validation of a new quality of life measure in pediatric lupus. Arthritis Rheum. 2007, 57, 1165–1173. [Google Scholar] [CrossRef]
- Leong, K.P.; Kong, K.O.; Thong, B.Y.H.; Koh, E.T.; Lian, T.Y.; Teh, C.L.; Cheng, Y.K.; Chng, H.H.; Badsha, H.; Law, W.G.; et al. Development and preliminary validation of a systemic lupus erythematosus-specific quality-of-life instrument (SLEQOL). Rheumatology 2005, 44, 1267–1276. [Google Scholar] [CrossRef]
- Doward, L.C.; McKenna, S.P.; Whalley, D.; Tennant, A.; Griffiths, B.; Emery, P.; Veale, D.J. The development of the L-QoL: A quality-of-life instrument specific to systemic lupus erythematosus. Ann. Rheum. Dis. 2009, 68, 196–200. [Google Scholar] [CrossRef]
- Chren, M.-M.; Lasek, R.J.; Flocke, S.A.; Zyzanski, S.J. Improved Discriminative and Evaluative Capability of a Refined Version of Skindex, a Quality-of-Life Instrument for Patients with Skin Diseases. Arch. Dermatol. 1997, 133, 1433–1440. [Google Scholar] [CrossRef]
- García-Riaño, D.; Ibáñez, E. Quality of life for the physically ill. Psiquiatr. Fac. 1992, 19, 148–161. (In Spanish) [Google Scholar]
- Thumboo, J.; Strand, V. Health-related quality of life in patients with systemic lupus erythematosus: An update. Ann. Acad. Med. 2007, 36, 115–122. [Google Scholar]
- Touma, Z.; Gladman, D.D.; Ibañez, M.; Urowitz, M.B. Is There an Advantage Over SF-36 with a Quality of Life Measure That Is Specific to Systemic Lupus Erythematosus? J. Rheumatol. 2011, 38, 1898–1905. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.P.; Wan, G.J.; Daly, R.P.; Topf, L.; Connolly-Strong, E.; Bostic, R.; Reed, M.L. Patient-reported flare frequency is associated with diminished quality of life and family role functioning in systemic lupus erythematosus. Qual. Life Res. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ogunsanya, M.E.; Cho, S.K.; Hudson, A.; Chong, B.F. Factors associated with quality of life in cutaneous lupus erythematosus using the Revised Wilson and Cleary Model. Lupus 2020, 29, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Li, M.; Liu, L.; Wang, Z.; Wang, Y.; Zhao, J.; Tian, X.; Li, M.; Zeng, X. Relationship between disease activity, organ damage and health-related quality of life in patients with systemic lupus erythematosus: A systemic review and meta-analysis. Autoimmun. Rev. 2020, 102691. [Google Scholar] [CrossRef]
- Pequeno, N.P.F.; Cabral, N.L.D.A.; Marchioni, D.M.; Lima, S.C.V.C.; Lyra, C.D.O. Quality of life assessment instruments for adults: A systematic review of population-based studies. Health Qual. Life Outcomes 2020, 18, 1–13. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Lynn, M.R. Determination and Quantification of Content Validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 21.0; IBM Corp.: Armonk, NY, USA, 2012. [Google Scholar]
- Fornell, C.; Larcker, D. Evaluating structural equations models with unobservable variables and measurement error. J. Mark Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Bentler, P.M. EQS 6 Structural Equations Modeling Software; Multivariate Software: Encino, CA, USA, 2004. [Google Scholar]
- Satorra, A.; Bentler, P.M. Corrections to Test Statistics and Standard Errors in Covariance Structure Analysis. In Latent Variables Analysis: Applications for Developmental Research; Von Eye, A., Clogg, C.C., Eds.; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts Applications and Programming, 2nd ed.; Routledge: New York, NY, USA, 2009. [Google Scholar]
- Maccallum, R.C.; Austin, J.T. Applications of Structural Equation Modeling in Psychological Research. Annu. Rev. Psychol. 2000, 51, 201–226. [Google Scholar] [CrossRef]
- Browne, M.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K., Long, J., Eds.; Sage Publications: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Henson, R.K.; Roberts, J.K. Use of Exploratory Factor Analysis in Published Research. Educ. Psychol. Meas. 2006, 66, 393–416. [Google Scholar] [CrossRef]
- Hair, J.; Anderson, R.; Tatham, R.; Black, W. Análisis Multivariante; Pearson Prentice Hall: Madrid, Spain, 2007. [Google Scholar]
- Nunnally, J. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- García de Yébennes, M.; Rodríguez, F.; Carmona, L. Validation of questionnaires. Reum. Clín 2008, 5, 171–177. (In Spanish) [Google Scholar] [CrossRef]
- Klein, R.; Moghadam-Kia, S.; Taylor, L.; Coley, C.; Okawa, J.; LoMonico, J.; Chren, M.-M.; Werth, V.P. Quality of life in cutaneous lupus erythematosus. J. Am. Acad. Dermatol. 2011, 64, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Jolly, M. How does quality of life of patients with systemic lupus erythematosus compare with that of other common chronic illnesses? J. Rheumatol. 2005, 32, 1706–1708. [Google Scholar] [PubMed]
- Ng, P.; Chan, W. Group Psychosocial Program for Enhancing Psychological Well-Being of People with Systemic Lupus Erythematosus. J. Soc. Work Disabil. Rehabil. 2007, 6, 75–87. [Google Scholar] [CrossRef] [PubMed]

| Characteristics (N = 158) | N | % |
|---|---|---|
| Gender | ||
| Women | 142 | 90 |
| Men | 16 | 10 |
| Lupus erythematosus type | ||
| Systemic | 115 | 73 |
| Cutaneous | 43 | 27 |
| Time to diagnosis | ||
| 0 to 3 months | 24 | 15 |
| 3 to 6 months | 10 | 6 |
| 6 to 9 months | 7 | 4 |
| 9 to 12 months | 3 | 2 |
| More than 12 months | 61 | 39 |
| They do not know/they do not remember | 53 | 34 |
| Complete Questionnaire (α = 0.92) | M | SD | rjx | α-x | A | K |
|---|---|---|---|---|---|---|
| Physical α = 0.92; CR = 0.92; AVE = 0.66 | ||||||
| LEQoL 11 | 7.12 | 3.29 | 0.67 | 0.91 | −1.24 | 0.22 |
| LEQoL 12 | 6.39 | 3.34 | 0.63 | 0.91 | −0.90 | 0.50 |
| LEQoL 13 | 7.13 | 3.35 | 0.62 | 0.91 | −1.28 | 0.19 |
| LEQoL 14 | 3.87 | 3.54 | 0.60 | 0.91 | 0.15 | −1.50 |
| LEQoL 24 | 6.51 | 3.51 | 0.59 | 0.91 | −0.84 | −0.73 |
| LEQoL 26 | 5.65 | 3.71 | 0.62 | 0.91 | −0.45 | −1.30 |
| Emotions α = 0.91; CR = 0.89; AVE = 0.61 | ||||||
| LEQoL 29a | 5.75 | 3.18 | 0.58 | 0.91 | −0.54 | −0.87 |
| LEQoL 29b | 5.16 | 3.27 | 0.55 | 0.91 | −0.26 | −1.09 |
| LEQoL 29c | 6.27 | 3.04 | 0.64 | 0.91 | −0.62 | −0.57 |
| LEQoL 29d | 6.06 | 3.14 | 0.66 | 0.91 | −0.60 | −0.69 |
| Cognition α = 0.89; CR = 0.91; AVE = 0.71 | ||||||
| LEQoL 39 | 5.27 | 3.70 | 0.56 | 0.91 | −0.39 | −1.37 |
| LEQoL 40 | 5.37 | 3.71 | 0.60 | 0.91 | −0.35 | −1.41 |
| LEQoL 42 | 4.73 | 3.56 | 0.62 | 0.91 | −0.12 | −1.43 |
| Appearance α = 0.88; CR = 0.90; AVE = 0.75 | ||||||
| LEQoL 43 | 4.68 | 3.73 | 0.53 | 0.91 | −0.02 | −1.48 |
| LEQoL 44 | 3.47 | 3.79 | 0.52 | 0.91 | 0.57 | −1.24 |
| LEQoL 45 | 3.57 | 3.49 | 0.52 | 0.91 | 0.47 | −1.13 |
| LEQoL 46 | 5.02 | 3.68 | 0.53 | 0.91 | −0.14 | −1.40 |
| LEQoL 48 | 5.66 | 3.46 | 0.52 | 0.91 | −0.47 | −1.09 |
| Relationships α = 0.82; CR = 0.83; AVE = 0.63 | ||||||
| LEQoL 62 | 2.65 | 3.42 | 0.46 | 0.92 | 0.90 | −0.68 |
| LEQoL 63 | 2.76 | 3.44 | 0.43 | 0.92 | 0.82 | −0.82 |
| LEQoL 66 | 2.03 | 2.96 | 0.35 | 0.92 | 1.30 | 0.42 |
| Both Types of Lupus | Systemic | Cutaneous | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | M | SD | M | SD | M | SD | U | p | d | MAX | MIN |
| Physical | 6.1 | 2.93 | 6.65 | 2.52 | 4.67 | 3.44 | 1674.50 | 0.00 * | 0.65 | 10 | 0 |
| Appearance | 4.5 | 2.98 | 4.71 | 2.79 | 4.07 | 3.45 | 2096.00 | 0.14 | 10 | 0 | |
| Emotion | 5.8 | 2.78 | 5.86 | 2.51 | 5.78 | 3.42 | 2306.50 | 0.51 | 10 | 0 | |
| Cognition | 5.2 | 3.2 | 5.78 | 2.92 | 3.65 | 3.72 | 1636.50 | 0.00 * | 0.63 | 10 | 0 |
| Relationships | 2.4 | 2.78 | 2.95 | 2.87 | 1.20 | 2.06 | 1450.50 | 0.00 * | 0.70 | 10 | 0 |
| Factors | Systemic | Cutaneous | Total (Max. 20) | C 10 | C 20 | C 25 | C 30 | C 40 | C 50 | C 60 | C 70 | C 75 | C 80 | C 90 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F1 | 6.65 | 4.67 | 11.32 | 0 | 3.63 | 4.3 | 5.3 | 6.5 | 7 | 7.6 | 8 | 8.1 | 8.3 | 9.3 |
| F2 | 4.71 | 4.07 | 8.78 | 0 | 1.6 | 2 | 2.8 | 3.5 | 4.6 | 5.2 | 6 | 6.6 | 7.4 | 8.8 |
| F3 | 5.82 | 5.78 | 11.6 | 1.5 | 3.5 | 4.25 | 4.6 | 5 | 6 | 6.7 | 7.7 | 8.2 | 8.7 | 9.25 |
| F4 | 5.78 | 3.65 | 9.35 | 0 | 1.5 | 2.3 | 2.9 | 5 | 6.1 | 7 | 7.6 | 8 | 8.3 | 9.03 |
| F5 | 2.95 | 1.20 | 4.13 | 0 | 0 | 0 | 0 | 0.53 | 1.5 | 2.6 | 3.6 | 4.6 | 5 | 7 |
| Total (Max. 50) | 25.91 | 19.37 | 45.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellano-Rioja, E.; Giménez-Espert, M.d.C.; Soto-Rubio, A. Lupus Erythematosus Quality of Life Questionnaire (LEQoL): Development and Psychometric Properties. Int. J. Environ. Res. Public Health 2020, 17, 8642. https://doi.org/10.3390/ijerph17228642
Castellano-Rioja E, Giménez-Espert MdC, Soto-Rubio A. Lupus Erythematosus Quality of Life Questionnaire (LEQoL): Development and Psychometric Properties. International Journal of Environmental Research and Public Health. 2020; 17(22):8642. https://doi.org/10.3390/ijerph17228642
Chicago/Turabian StyleCastellano-Rioja, Elena, María del Carmen Giménez-Espert, and Ana Soto-Rubio. 2020. "Lupus Erythematosus Quality of Life Questionnaire (LEQoL): Development and Psychometric Properties" International Journal of Environmental Research and Public Health 17, no. 22: 8642. https://doi.org/10.3390/ijerph17228642
APA StyleCastellano-Rioja, E., Giménez-Espert, M. d. C., & Soto-Rubio, A. (2020). Lupus Erythematosus Quality of Life Questionnaire (LEQoL): Development and Psychometric Properties. International Journal of Environmental Research and Public Health, 17(22), 8642. https://doi.org/10.3390/ijerph17228642