Workplace Screening Identifies Clinically Significant and Potentially Reversible Kidney Injury in Heat-Exposed Sugarcane Workers

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Parent Study Design
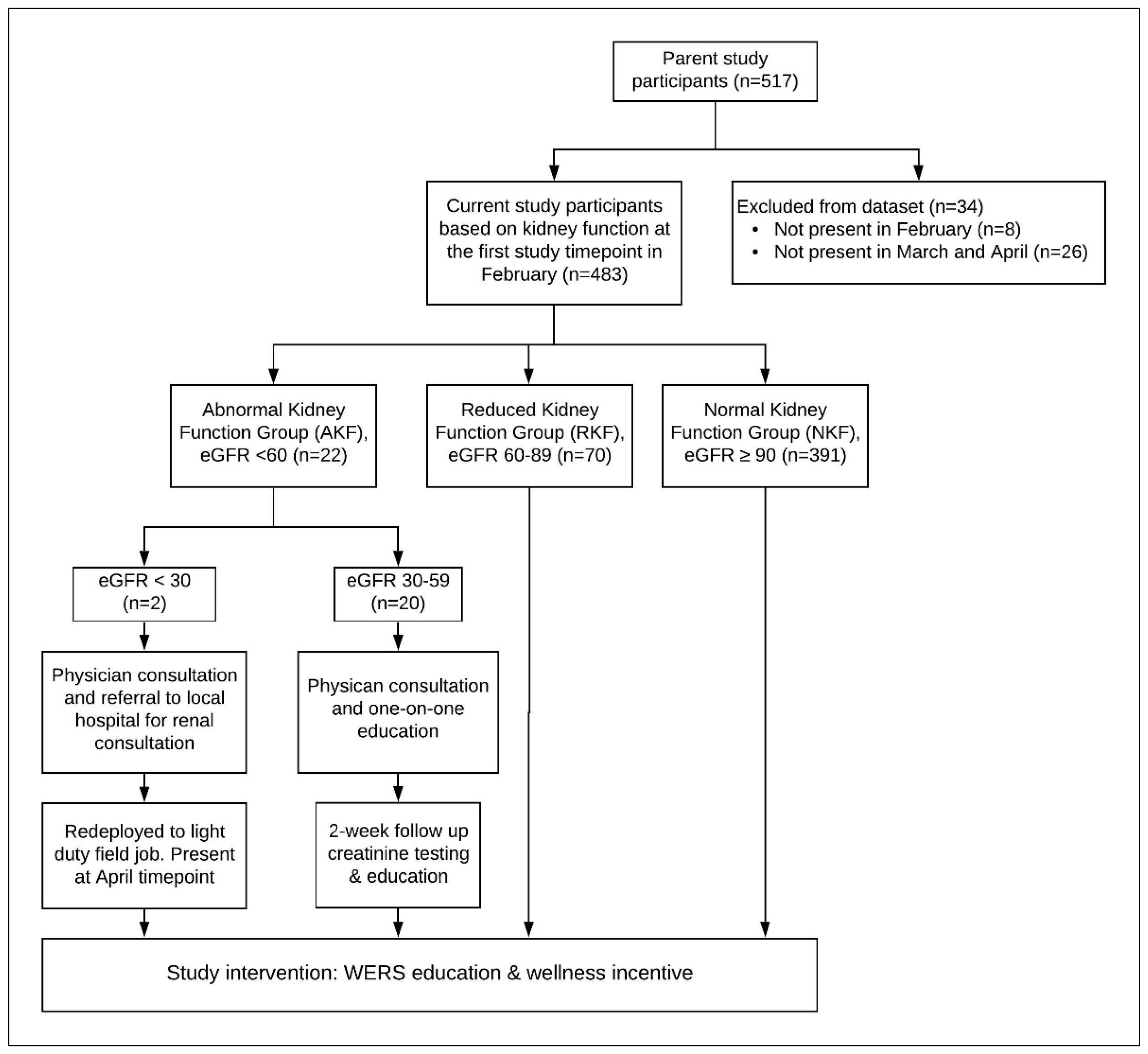
2.2. Current Study Design
2.3. Data Collection
2.4. Additional Interventions and Education for Participants with Abnormal Kidney Function
2.5. Statistical Analysis
3. Results
3.1. Current Study Participants
3.2. Heat Exposure
3.3. Retrospective Assessment: Baseline Harvest Characteristics
3.4. Retrospective Assessment: Change in eGFR from 2012 to 2016
3.5. Prospective Assessment: 2016 Pre-Harvest Characteristics
3.6. Prospective Assessment: Effect of WERS Intervention on Trajectory of Renal Function Decline during the 2016–2017 Harvest Season
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Disclosures
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Workers (n = 517) | Excluded Workers (n = 34) | Included Workers (n = 483) | p Value |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Age, years | 30.6 (8.6) | 28.8 (7.9) | 30.7 (8.7) | 0.21 |
| Number of harvests worked | 2.9 (1.2) | 2.8 (1.4) | 2.9 (1.2) | 0.68 |
| Body mass index (n = 478) | 23.2 (2.5) | 23.8 (2.7) (n = 30) | 23.2 (2.5) (n = 448) | 0.17 |
| Creatinine, mg/dL | 0.90 (0.16) | 0.90 (0.12) (n = 33) | 0.90 (0.17) (n = 483) | 0.96 |
| eGFR, ml/min per 1.73 m2 | 111.1 (16.7) | 113.4 (14.2) (n = 33) | 110.9 (16.8) (n = 483) | 0.41 |
| Race/Ethnicity, n (%), (n = 478) | ||||
| Latino | 145 (30.3%) | 8 (26.7%) | 137 (30.6%) | 0.65 |
| Indigenous | 333 (69.7%) | 22 (73.3%) | 311 (69.4%) | |
| Home residence, n (%) | ||||
| Local (Zona) | 330 (63.8%) | 11 (32.4%) | 319 (66.1%) | <0.0001 |
| Highland (Altiplano) | 187 (36.2%) | 23 (67.7%) | 164 (33.9%) | |
| Job Type, n (%) | ||||
| Cane Cutter | 418 (80.9%) | 32 (94.1%) | 386 (79.9%) | 0.04 |
| Production Worker | 99 (19.2%) | 2 (5.9%) | 97 (20.1%) | |
| Smoking, n (%) (n = 473) | 52 (11.0%) | 4 (13.8%) (n = 29) | 48 (10.2%) (n = 444) | 0.55 ** |
| Mild hypertension *, n (%) (n = 478) | 162 (33.9%) | 8 (26.7%) (n = 30) | 154 (34.4%) (n = 448) | 0.39 |
| Alcohol intake, n (%) (n = 474) | 45 (9.5%) | 4 (13.3%) (n = 30) | 41 (9.2%) (n = 444) | 0.51 ** |
| Water Source, n (%) (n = 477) | ||||
| Municipal | 369 (77.4%) | 24 (80.0%) | 345 (77.2%) | 0.53 |
| Well | 90 (18.9%) | 4 (13.3%) | 86 (19.2%) | |
| Surface Water | 18 (3.8%) | 2 (6.7%) | 16 (3.6%) | |
| Comparison of 2017 February Pre-Shift eGFR for Excluded Workers Missing Both March and April eGFR Values and Included Workers with March and/or April eGFR Values. *** | ||||
| All Workers (n = 509) | Excluded workers (n = 26) | Included Workers (n = 483) | p Value | |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| February eGFR, ml/min per 1.73 m2 | 110.3 (24.7) | 113.1 (30.7) | 110.2 (24.4) | 0.56 |

References
- Glaser, J.; Lemery, J.; Rajagopalan, B.; Diaz, H.F.; García-Trabanino, R.; Taduri, G.; Madero, M.; Amarasinghe, M.; Abraham, G.; Anutrakulchai, S.; et al. Climate change and the emergent epidemic of CKD from heat stress in rural communities: The case for heat stress nephropathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; Gonzalez-Quiroz, M.; Weiss, I.; Glaser, J.; Vindell, J.J.; Stockfelt, L.; Roncal, C.; et al. Heat stress, dehydration, and kidney function in sugarcane cutters in El Salvador—A cross-shift study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Orantes, C.M.; Herrera, R.; Almaguer, M.; Brizuela, E.G.; Hernández, C.E.; Bayarre, H.; Amaya, J.C.; Calero, D.J.; Orellana, P.; Colindres, R.M.; et al. Chronic kidney disease and associated risk factors in the Bajo Lempa region of El Salvador: Nefrolempa study, 2009. MEDICC Rev. 2011, 13, 14–22. [Google Scholar] [PubMed]
- Valdés, R.H.; Orantes, C.M.; Almaguer, M.; Alfonso, P.; Bayarre, H.D.; Leiva, I.M.; Smith, M.J.; Cubias, R.A.; Torres, C.G.; Almendárez, W.O.; et al. Clinical characteristics of chronic kidney disease of nontraditional causes in Salvadoran farming communities. MEDICC Rev. 2014, 16, 39–48. [Google Scholar]
- Nanayakkara, S.; Komiya, T.; Ratnatunga, N.; Senevirathna, S.T.M.L.D.; Harada, K.H.; Hitomi, T.; Gobe, G.; Muso, E.; Abeysekera, T.; Koizumi, A. Tubulointerstitial damage as the major pathological lesion in endemic chronic kidney disease among farmers in North Central Province of Sri Lanka. Environ. Health Prev. Med. 2011, 17, 213–221. [Google Scholar] [CrossRef]
- Abraham, G.; Varughese, S.; Thandavan, T.; Iyengar, A.; Fernando, E.; Naqvi, S.A.J.; Sheriff, R.; Ur-Rashid, H.; Gopalakrishnan, N.; Kafle, R.K.; et al. Chronic kidney disease hotspots in developing countries in South Asia. Clin. Kidney J. 2016, 9, 135–141. [Google Scholar] [CrossRef]
- Wanigasuriya, K. Update on uncertain etiology of chronic kidney disease in Sri Lanka’s north-central dry zone. MEDICC Rev. 2014, 16, 61–65. [Google Scholar]
- Gifford, F.J.; Gifford, R.M.; Eddleston, M.; Dhaun, N. Endemic nephropathy around the world. Kidney Int. Rep. 2017, 2, 282–292. [Google Scholar] [CrossRef]
- Moyce, S.; Joseph, J.; Tancredi, D.; Mitchell, D.; Schenker, M. Cumulative incidence of acute kidney injury in California’s agricultural workers. J. Occup. Environ. Med. 2016, 58, 391–397. [Google Scholar] [CrossRef]
- Johnson, R.J.; Wesseling, C.; Newman, L.S. Epidemic chronic kidney disease in agricultural communities. N. Engl. J. Med. 2019, 380, 1843–1852. [Google Scholar] [CrossRef]
- Fischer, R.S.; Vangala, C.; Truong, L.; Mandayam, S.; Chavarria, D.; Llanes, O.M.G.; Laguna, M.U.F.; Baez, A.G.; Garcia, F.; García-Trabanino, R.; et al. Early detection of acute tubulointerstitial nephritis in the genesis of Mesoamerican nephropathy. Kidney Int. 2018, 93, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Wegman, D.H.; Apelqvist, J.; Bottai, M.; Ekström, U.; García-Trabanino, R.; Glaser, J.; Hogstedt, C.; Jakobsson, K.; Jarquín, E.; Lucas, R.A.; et al. Intervention to diminish dehydration and kidney damage among sugarcane workers. Scand. J. Work. Environ. Health 2017, 44, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Rubio, O.; Amador, J.J.; Kaufman, J.S.; Weiner, D.E.; Parikh, C.R.; Khan, U.; McClean, M.D.; Laws, R.L.; López-Pilarte, D.; Friedman, D.J.; et al. Urine biomarkers of kidney injury among adolescents in Nicaragua, a region affected by an epidemic of chronic kidney disease of unknown aetiology. Nephrol. Dial. Transplant. 2016, 31, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Cerón, A.; Fort, M.P.; Morine, C.M.; Lou-Meda, R. Chronic kidney disease among children in Guatemala. Rev. Panam. Salud Pública 2014, 36, 376–382. [Google Scholar]
- Leibler, J.H.; Ramirez-Rubio, O.; Velázquez, J.J.A.; Pilarte, D.L.; Obeid, W.; Parikh, C.R.; Gadupudi, S.; Scammell, M.K.; Friedman, D.J.; Brooks, D.R. Europe PMC. Available online: https://europepmc.org/article/med/32504218 (accessed on 18 November 2020).
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Rivard, C.J.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J. Heat stress, hydration and uric acid: A cross-sectional study in workers of three occupations in a hotspot of Mesoamerican nephropathy in Nicaragua. BMJ Open 2016, 6, 011034. [Google Scholar] [CrossRef]
- Roncal-Jimenez, C.; Lanaspa, M.A.; Jensen, T.; Sanchezlozada, L.G.; Johnson, R.J. Mechanisms by which dehydration may lead to chronic kidney disease. Ann. Nutr. Metab. 2015, 66, 10–13. [Google Scholar] [CrossRef]
- Jayasumana, C.; Gunatilake, S.; Senanayake, P. Glyphosate, Hard water and nephrotoxic metals: Are they the culprits behind the epidemic of chronic kidney disease of unknown etiology in Sri Lanka? Int. J. Environ. Res. Public Health 2014, 11, 2125–2147. [Google Scholar] [CrossRef]
- Valcke, M.; Levasseur, M.-E.; Da Silva, A.S.; Wesseling, C. Pesticide exposures and chronic kidney disease of unknown etiology: An epidemiologic review. Environ. Health 2017, 16, 49. [Google Scholar] [CrossRef]
- Lucas, R.A.; Bodin, T.; García-Trabanino, R.; Wesseling, C.; Glaser, J.; Weiss, I.; Jarquin, E.; Jakobsson, K.; Wegman, D.H. Heat stress and workload associated with sugarcane cutting—An excessively strenuous occupation! Extreme Physiol. Med. 2015, 4, A23. [Google Scholar] [CrossRef]
- Crowe, J.; Wesseling, C.; Solano, B.R.; Umaña, M.P.; Ramírez, A.R.; Kjellstrom, T.; Morales, D.; Nilsson, M. Heat exposure in sugarcane harvesters in Costa Rica. Am. J. Ind. Med. 2013, 56, 1157–1164. [Google Scholar] [CrossRef]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramirez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, J.M.; et al. Biomarkers of kidney injury among Nicaraguan sugarcane workers. Am. J. Kidney Dis. 2016, 67, 209–217. [Google Scholar] [CrossRef]
- Dally, M.; Butler-Dawson, J.; Krisher, L.; Monaghan, A.; Weitzenkamp, D.; Sorensen, C.; Johnson, R.J.; Carlton, E.J.; Asensio, C.; Tenney, L.; et al. The impact of heat and impaired kidney function on productivity of Guatemalan sugarcane workers. PLoS ONE 2018, 13, 0205181. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Resolution CD52 R10 Chronic Kidney Disease in Agricultural Communities in Central America; Pan American Health Organization: Washington, DC, USA, 2013; Available online: https://www.scielosp.org/article/rpsp/2016.v40n5/294-300/en/ (accessed on 17 November 2020).
- Council of Health Ministers of Central America San Salvador Declaration. MEDICC Review. Available online: http://www.medicc.org/mediccreview/documents/San_Salvador_English_online.pdf (accessed on 18 November 2020).
- Wesseling, C.; Crowe, J.; Hogstedt, C.; Jakobsson, K.; Lucas, R.; Wegman, D. Mesoamerican Nephropathy: Report From the First International Research Workshop On Men; National University of Costa Rica: Heredia, Costa Rica, 2013. [Google Scholar]
- Ramirez-Rubio, O.; McClean, M.D.; Amador, J.J.; Brooks, D.R. An epidemic of chronic kidney disease in Central America: An overview. Postgrad. Med. J. 2013, 89, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Lozier, M.; Turcios-Ruiz, R.M.; Noonan, G.; Ordunez, P. Chronic kidney disease of nontraditional etiology in Central America: A provisional epidemiologic case definition for surveillance and epidemiologic studies. Rev. Panam. Salud Pública 2016, 40, 294–300. [Google Scholar] [PubMed]
- Wesseling, C.; Glaser, J.; Rodríguez-Guzmán, J.; Weiss, I.; Lucas, R.; Peraza, S.; Da Silva, A.S.; Hansson, E.; Johnson, R.J.; Hogstedt, C.; et al. Chronic kidney disease of non-traditional origin in Mesoamerica: A disease primarily driven by occupational heat stress. Rev. Panam. Salud Pública 2020, 4, e125. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; Krisher, L.; Asensio, C.; Cruz, A.; Tenney, L.; Weitzenkamp, D.; Dally, M.; Asturias, E.J.; Newman, L.S. Risk factors for declines in kidney function in sugarcane workers in Guatemala. J. Occup. Environ. Med. 2018, 60, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Bodin, T.; García-Trabanino, R.; Weiss, I.; Jarquín, E.; Glaser, J.; Jakobsson, K.; Lucas, R.A.I.; Wesseling, C.; Hogstedt, C.; Wegman, D.H.; et al. Intervention to reduce heat stress and improve efficiency among sugarcane workers in El Salvador: Phase 1. Occup. Environ. Med. 2016, 73, 409–416. [Google Scholar] [CrossRef]
- Glaser, J.; Hansson, E.; Weiss, I.; Wesseling, C.; Jakobsson, K.; Ekström, U.; Apelqvist, J.; Lucas, R.; Monge, E.A.; Peraza, S.; et al. Preventing kidney injury among sugarcane workers: Promising evidence from enhanced workplace interventions. Occup. Environ. Med. 2020, 77, 527–534. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; Krisher, L.; Yoder, H.; Dally, M.; Sorensen, C.; Johnson, R.J.; Asensio, C.; Cruz, A.; Johnson, E.C.; Carlton, E.J.; et al. Evaluation of heat stress and cumulative incidence of acute kidney injury in sugarcane workers in Guatemala. Int. Arch. Occup. Environ. Health 2019, 92, 977–990. [Google Scholar] [CrossRef]
- Sorensen, C.; Butler-Dawson, J.; Dally, M.; Krisher, L.; Griffin, B.R.; Johnson, R.J.; Lemery, J.; Asensio, C.; Tenney, L.; Newman, L.S.; et al. Risk Factors and mechanisms underlying cross-shift decline in kidney function in Guatemalan sugarcane workers. J. Occup. Environ. Med. 2019, 61, 239–250. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; Dally, M.; Johnson, R.J.; Johnson, E.C.; Krisher, L.; Sánchez-Lozada, L.G.; Griffin, B.R.; Brindley, S.; Newman, L.S. Association of copeptin, a surrogate marker of arginine vasopressin, with decreased kidney function in sugarcane workers in Guatemala. Ann. Nutr. Metab. 2020, 76, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Perrier, E.T.; Bottin, J.H.; Vecchio, M.; Lemetais, G. Criterion values for urine-specific gravity and urine color representing adequate water intake in healthy adults. Eur. J. Clin. Nutr. 2017, 71, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Webb, M.C.; Salandy, S.T.; Beckford, S.E. Monitoring hydration status pre- and post-training among university athletes using urine color and weight loss indicators. J. Am. Coll. Health 2016, 64, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.R.; Butler-Dawson, J.; Dally, M.; Krisher, L.; Cruz, A.; Weitzenkamp, D.; Sorensen, C.; Tenney, L.; Johnson, R.J.; Newman, L.S.; et al. Unadjusted point of care creatinine results overestimate acute kidney injury incidence during field testing in Guatemala. PLoS ONE 2018, 13, 0204614. [Google Scholar] [CrossRef] [PubMed]
- Butler-Dawson, J. PLoS ONE. Available online: https://journals.plos.org/plosone/article/comment?id=10.1371/annotation/35061b06-beee-49a8-881a-d13d5f28546d (accessed on 18 November 2020).
- Levey, A.S.; Stevens, L.A. Estimating GFR Using the CKD Epidemiology collaboration (CKD-EPI) creatinine equation: More accurate GFR estimates, lower CKD prevalence estimates, and better risk predictions. Am. J. Kidney Dis. 2010, 55, 622–627. [Google Scholar] [CrossRef]
- Occupational Safety and Health Administration. Heat Stress; Occupational Safety and Health Administration: Washington, DC, USA, 2017; Section III: Chapter 4. [Google Scholar]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef]
- Crowe, J.; Nilsson, M.; Kjellström, T.; Cerdas, M.; Johnson, R.; Wesseling, C. DiVA Portal. Available online: http://umu.diva-portal.org/smash/record.jsf?pid=diva2%3A745252&dswid=4544 (accessed on 18 November 2020).
- Wesseling, C.; Aragón, A.; Gonzalez-Quiroz, M.; Weiss, I.; Glaser, J.; Bobadilla, N.A.; Harra, T.; Correa-Rotter, R.; Johnson, R.J.; Barregard, L.; et al. Kidney function in sugarcane cutters in Nicaragua—A longitudinal study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2016, 147, 125–132. [Google Scholar] [CrossRef]
- Gonzalez-Quiroz, M.; Smpokou, E.-T.; Silverwood, R.J.; Camacho, A.; Faber, D.; Garcia, B.L.R.; Oomatia, A.; Hill, M.; Glaser, J.; Le Blond, J.; et al. Decline in kidney function among apparently healthy young Adults at risk of Mesoamerican nephropathy. J. Am. Soc. Nephrol. 2018, 29, 2200–2212. [Google Scholar] [CrossRef]
- Wijkström, J.; González-Quiroz, M.; Hernandez, M.; Trujillo, Z.; Hultenby, K.; Ring, A.; Söderberg, M.; Aragón, A.; Elinder, C.G.; Wernerson, A.; et al. Renal morphology, clinical findings, and progression rate in Mesoamerican nephropathy. Am. J. Kidney Dis. 2017, 69, 626–636. [Google Scholar] [CrossRef]
- Li, L.; Astor, B.C.; Lewis, J.; Hu, B.; Appel, L.J.; Lipkowitz, M.S.; Toto, R.D.; Wang, X.; Wright, J.T.; Greene, T.H. Longitudinal Progression Trajectory of GFR Among Patients With CKD. Am. J. Kidney Dis. 2012, 59, 504–512. [Google Scholar] [CrossRef] [PubMed]



| Characteristics | All Workers (n = 483) | AKF Workers (n = 22) | RKF Workers (n = 70) | NKF Workers (n = 391) | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | p Value | |
| Age, years | 28.6 (8.5) | 29.2 (6.7) | 33.5 (8.7) | 27.7 (8.2) | <0.0001 |
| Number of harvests worked | 2.9 (1.2) | 3.5 (1.3) | 3.1 (1.3) | 2.8 (1.2) | 0.01 |
| Body mass index, kg/m2 (n = 320) | 23.1 (2.6) | 23.4 (2.6) (n = 16) | 23.8 (2.7) (n = 49) | 23.0 (2.5) (n = 255) | 0.11 |
| eGFR, ml/min per 1.73 m2 | 112.38 (15.02) | 102.6 (18.4) | 102.2 (17.4) | 114.8 (13.3) | <0.0001 |
| Race/Ethnicity, n (%) (n = 448) | |||||
| Latino | 137 (30.6%) | 3 (15.0%) (n = 20) | 24 (36.4%) (n = 66) | 110 (30.4%) (n = 362) | 0.19 |
| Indigenous | 311 (69.4%) | 17 (85.0%) | 42 (63.6%) | 252 (69.6%) | |
| Home residence, n (%) | |||||
| Local (Zona) | 319 (66.1%) | 19 (86.4%) | 57 (81.4%) | 243 (62.2%) | 0.0009 |
| Highland (Altiplano) | 164 (34.0%) | 3 (13.6%) | 13 (18.6%) | 148 (37.9%) | |
| Job Type, n (%) | |||||
| Cane Cutter | 386 (79.9%) | 19 (86.4%) | 59 (84.3%) | 308 (78.8%) | 0.42 |
| Production Worker | 97 (20.1%) | 3 (13.6%) | 11 (15.7%) | 83 (21.2%) | |
| Mild hypertension ** n (%) (n = 243) | 120 (49.4%) | 8 (57.1%) (n = 14) | 14 (34.2%) (n = 41) | 98 (52.1%) (n = 188) | 0.09 |
| Smoking, n (%) (n = 317) | 29 (9.2%) | 3 (18.8%) (n = 16) | 9 (18.4%) (n = 49) | 17 (6.8%) (n = 252) | 0.01 *** |
| Alcohol intake, n (%) (n = 317) | 22 (6.9%) | 2 (12.5%) (n = 16) | 6 (12.2%) (n = 49) | 14 (5.6%) (n = 252) | 0.11 *** |
| Effect | Estimate (95% CI) | p Value |
|---|---|---|
| NKF (n = 387) | −0.18 (−0.66, 0.29) | 0.451 |
| RKF (n = 70) | −2.02 (−3.03, −1.00) | 0.0001 |
| AKF (n = 22) | −7.52 (−9.04, −6.01) | <0.0001 |
| Group Comparisons | Rate of Yearly Change in eGFR, Between Group Comparisons | |
|---|---|---|
| NKF, n = 387 | Effect (95% CI) | p value |
| RKF, n = 70 | ||
| AKF, n = 22 | ||
| RKF vs. NKF | −1.83 (−2.95, −0.71) | 0.0014 |
| AKF vs. NKF | −7.34 (−8.93, −5.76) | <0.0001 |
| AKF vs. RKF | −5.51 (−7.33, −3.69) | <0.0001 |
| Characteristics | All Workers (n = 483) | AKF Workers (n = 22) | RKF Workers (n = 70) | NKF Workers (n = 391) | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | p Value | |
| Age, years | 30.7 (8.7) | 32.2 (6.5) | 36.0 (8.8) | 29.7 (8.4) | <0.0001 |
| Body mass index, kg/m2 (n = 448) | 23.2 (2.5) | 22.8 (1.5) (n = 20) | 23.5 (2.5) (n = 66) | 23.1 (2.6) (n = 362) | 0.46 |
| Creatinine, mg/dL | 0.90 (0.17) | 1.27 (0.22) | 1.00 (0.17) | 0.86 (0.12) | <0.0001 |
| eGFR, ml/min per 1.73 m2 | 110.9 (16.8) | 77.3 (19.5) | 96.9 (16.4) | 115.4 (12.8) | <0.0001 |
| Mild hypertension *, n (%) (n = 448) | 154 (34.4%) | 5 (25.0%) (n = 20) | 29 (43.9%) (n = 66) | 120 (33.2%) (n = 362) | 0.16 |
| Smoking, n (%) (n = 444) | 48 (10.8%) | 4 (20%) (n = 20) | 6 (9.1%) (n = 66) | 38 (10.6%) (n = 358) | 0.37 |
| Alcohol intake, n (%) (n = 444) | 41 (9.2%) | 3 (15.0%) (n = 20) | 6 (9.1%) (n = 66) | 32 (8.9%) (n = 358) | 0.66 |
| Water Source at Home, n (%), (n = 447) | |||||
| Municipal | 345 (77.2%) | 13 (65.0%) | 55 (84.6%) | 277 (76.5%) | 0.19 ** |
| Well | 86 (19.2%) | 6 (30.0%) | 10 (15.4%) | 70 (19.3%) | |
| Surface Water | 16 (3.6%) | 1 (5.0%) | 0 (0.0%) | 15 (4.1%) | |
| Rate of Change in eGFR | NKF (n = 362) | p Value | RKF (n = 66) | p Value | AKF (n = 20) | p Value |
|---|---|---|---|---|---|---|
| Pre-intervention (August 2016–February 2017), ml/min/1.73m2 (95% CI) | 0.71 (0.41, 1.02) | <0.0001 | −3.36 (−4.08, −2.64) | <0.0001 | −4.37 (−5.68, −3.06) | <0.0001 |
| Post-intervention (February–April 2017), ml/min/1.73m2 (95% CI) | 1.31 (−0.61, 3.23) | 0.181 | 6.05 (1.55, 10.54) | 0.008 | 5.62 (−2.65, 13.89) | 0.183 |
| Difference in monthly rate of eGFR change between pre-intervention and post-intervention (95% CI) | 0.60 (−1.34, 2.54) | 0.548 | 9.41 (4.85, 13.96) | <0.0001 | 9.99 (1.62, 18.36) | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorensen, C.J.; Krisher, L.; Butler-Dawson, J.; Dally, M.; Dexter, L.; Asensio, C.; Cruz, A.; Newman, L.S. Workplace Screening Identifies Clinically Significant and Potentially Reversible Kidney Injury in Heat-Exposed Sugarcane Workers. Int. J. Environ. Res. Public Health 2020, 17, 8552. https://doi.org/10.3390/ijerph17228552
Sorensen CJ, Krisher L, Butler-Dawson J, Dally M, Dexter L, Asensio C, Cruz A, Newman LS. Workplace Screening Identifies Clinically Significant and Potentially Reversible Kidney Injury in Heat-Exposed Sugarcane Workers. International Journal of Environmental Research and Public Health. 2020; 17(22):8552. https://doi.org/10.3390/ijerph17228552
Chicago/Turabian StyleSorensen, Cecilia J., Lyndsay Krisher, Jaime Butler-Dawson, Miranda Dally, Lynn Dexter, Claudia Asensio, Alex Cruz, and Lee S. Newman. 2020. "Workplace Screening Identifies Clinically Significant and Potentially Reversible Kidney Injury in Heat-Exposed Sugarcane Workers" International Journal of Environmental Research and Public Health 17, no. 22: 8552. https://doi.org/10.3390/ijerph17228552
APA StyleSorensen, C. J., Krisher, L., Butler-Dawson, J., Dally, M., Dexter, L., Asensio, C., Cruz, A., & Newman, L. S. (2020). Workplace Screening Identifies Clinically Significant and Potentially Reversible Kidney Injury in Heat-Exposed Sugarcane Workers. International Journal of Environmental Research and Public Health, 17(22), 8552. https://doi.org/10.3390/ijerph17228552