Effectiveness of a Group-Based Progressive Strength Training in Primary Care to Improve the Recurrence of Low Back Pain Exacerbations and Function: A Randomised Trial

 ,
,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Material and Methods
2.1. Participants
2.2. Procedures
2.2.1. Randomization and Allocation
2.2.2. Intervention Group
2.2.3. Control Group
2.3. Outcomes
2.3.1. LBP Exacerbation Episodes
2.3.2. LBP Intensity
2.3.3. Widespread Pain Sites
2.3.4. Analgesics
2.3.5. Disability
2.3.6. Isometric Lumbar Extension
2.3.7. Handgrip Strength
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Hart, L.G.; Deyo, R.A.; Cherkin, D.C. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine (Phila Pa 1976) 1995, 20, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Stanton, T.R.; Henschke, N.; Maher, C.G.; Refshauge, K.M.; Latimer, J.; McAuley, J.H. After an Episode of Acute Low Back Pain, Recurrence Is Unpredictable and Not as Common as Previously Thought. Spine (Phila. Pa. 1976) 2008, 33, 2923–2928. [Google Scholar] [CrossRef] [PubMed]
- Viniol, A.; Jegan, N.; Brugger, M.; Leonhardt, C.; Barth, J.; Baum, E.; Becker, A.; Strauch, K. Even worse-Risk factors and protective factors for transition from chronic localized low back pain to chronic widespread pain in general practice. Spine (Phila. Pa. 1976) 2015, 40, E890–E899. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Parreira, P.; Heymans, M.W.; van Tulder, M.W.; Esmail, R.; Koes, B.W.; Poquet, N.; Lin, C.-W.C.; Maher, C.G. Back Schools for chronic non-specific low back pain. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Delitto, A.; Sciences, R.; George, S.Z.; Health, B.; Van Dillen, L.; Surgery, O.; Whitman, J.M.; Physical, M.; Fellowship, T.; Motion, E.I.; et al. Low Back Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2012, 42, 1–81. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Suetta, C.; Magnusson, S.P.; Rosted, A.; Aagaard, P.; Jakobsen, A.K.; Larsen, L.H.; Duus, B.; Kjaer, M. Resistance training in the early postoperative phase reduces hospitalization and leads to muscle hypertrophy in elderly hip surgery patients-A controlled, randomized study. J. Am. Geriatr. Soc. 2004, 52, 2016–2022. [Google Scholar] [CrossRef]
- Iversen, V.M.; Vasseljen, O.; Mork, P.J.; Gismervik, S.; Bertheussen, G.F.; Salvesen, Ø.; Fimland, M.S. Resistance band training or general exercise in multidisciplinary rehabilitation of low back pain? A randomized trial. Scand. J. Med. Sci. Sports 2018, 28, 2074–2083. [Google Scholar] [CrossRef]
- Jakobsen, M.D.; Sundstrup, E.; Brandt, M.; Jay, K.; Aagaard, P.; Andersen, L.L. Effect of workplace- versus home-based physical exercise on musculoskeletal pain among healthcare workers: A cluster randomized controlled trial. Scand. J. Work. Environ. Health 2015, 41, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.; Bruce-Low, S.; Smith, D. A reappraisal of the deconditioning hypothesis in low back pain: Review of evidence from a triumvirate of research methods on specific lumbar extensor deconditioning. Curr. Med. Res. Opin. 2014, 30, 865–911. [Google Scholar] [CrossRef] [PubMed]
- Goubert, D.; Van Oosterwijck, J.; Meeus, M.; Danneels, L. Structural Changes of Lumbar Muscles in Non-Specific Low Back Pain. Pain Phys. 2016, 19, E985–E1000. [Google Scholar]
- Leinonen, V.; Kankaanpää, M.; Airaksinen, O.; Hänninen, O. Back and hip extensor activities during trunk flexion/extension: Effects of low back pain and rehabilitation. Arch. Phys. Med. Rehabil. 2000, 81, 32–37. [Google Scholar] [CrossRef]
- Amabile, A.H.; Bolte, J.H.; Richter, S.D. Atrophy of gluteus maximus among women with a history of chronic low back pain. PLoS ONE 2017, 12, e0177008. [Google Scholar] [CrossRef] [PubMed]
- Jeong, U.-C.; Sim, J.-H.; Kim, C.-Y.; Hwang-Bo, G.; Nam, C.-W. The effects of gluteus muscle strengthening exercise and lumbar stabilization exercise on lumbar muscle strength and balance in chronic low back pain patients. J. Phys. Ther. Sci. 2015, 27, 3813–3816. [Google Scholar] [CrossRef] [PubMed]
- Durmus, D.; Unal, M.; Kuru, O. How effective is a modified exercise program on its own or with back school in chronic low back pain? A randomized-controlled clinical trial. J. Back Musculoskelet. Rehabil. 2014, 27, 553–561. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Steffens, D.; Maher, C.G.; Pereira, L.S.M.; Stevens, M.L.; Oliveira, V.C.; Chapple, M.; Teixeira-Salmela, L.F.; Hancock, M.J. Prevention of Low Back Pain. JAMA Intern. Med. 2016, 176, 199. [Google Scholar] [CrossRef]
- Jenkins, N.D.M.; Miramonti, A.A.; Hill, E.C.; Smith, C.M.; Cochrane-Snyman, K.C.; Housh, T.J.; Cramer, J.T. Greater neural adaptations following high- vs. low-load resistance training. Front. Physiol. 2017, 8, 331. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Peterson, M.D.; Ogborn, D.; Contreras, B.; Sonmez, G.T. Effects of low- vs. High-load resistance training on muscle strength and hypertrophy in well-trained men. J. Strength Cond. Res. 2015, 29, 2954–2963. [Google Scholar] [CrossRef] [PubMed]
- Ratamess, N.A.; Alvar, B.A.; Evetoch, T.K.; Housh, T.J.; Kibler, W.B.; Kraemer, W.J.; Triplett, N.T. Progression Models in Resistance Training for Healthy Adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Iversen, V.M.; Mork, P.J.; Vasseljen, O.; Bergquist, R.; Fimland, M.S. Multiple-joint exercises using elastic resistance bands vs. conventional resistance-training equipment: A cross-over study. Eur. J. Sport Sci. 2017, 17, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.C.; McGill, S.M. Effect of Long-term Isometric Training on Core/Torso Stifness. J. Strength Cond. Res. 2015, 29, 1515–1526. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, J.; Casaña, J.; Martín, F.; Jakobsen, M.D.; Colado, J.C.; Andersen, L.L. Progression of Core Stability Exercises Based on the Extent of Muscle Activity. Am. J. Phys. Med. Rehabil. 2017, 96, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Soukup, M.G.; Glomsröd, B.; Lönn, J.H.; Bö, K.; Larsen, S. The effect of a Mensendieck exercise program as secondary prophylaxis for recurrent low back pain: A randomized, controlled trial with 12-month follow-up. Spine (Phila. Pa. 1976) 1999, 24, 1585–1592. [Google Scholar] [CrossRef]
- Farrar, J.T.; Troxel, A.B.; Stott, C.; Duncombe, P.; Jensen, M.P. Validity, reliability, and clinical importance of change in a 0-10 numeric rating scale measure of spasticity: A post hoc analysis of a randomized, double-blind, placebo-controlled trial. Clin. Ther. 2008, 30, 974–985. [Google Scholar] [CrossRef]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Davidson, M.; Keating, J.L. A comparison of five low back disability questionnaires: Reliability and responsiveness. Phys. Ther. 2002, 82, 8–24. [Google Scholar] [CrossRef]
- Demoulin, C.; Vanderthommen, M.; Duysens, C.; Crielaard, J.M. Spinal muscle evaluation using the Sorensen test: A critical appraisal of the literature. Jt. Bone Spine 2006, 73, 43–50. [Google Scholar] [CrossRef]
- Denteneer, L.; Van Daele, U.; Truijen, S.; De Hertogh, W.; Meirte, J.; Stassijns, G. Reliability of physical functioning tests in patients with low back pain: A systematic review. Spine J. 2018, 18, 190–207. [Google Scholar] [CrossRef] [PubMed]
- España-Romero, V.; Ortega, F.B.; Vicente-Rodríguez, G.; Artero, E.G.; Rey, J.P.; Ruiz, J.R. Elbow position affects handgrip strength in adolescents: Validity and reliability of jamar, dynex, and TKK dynamometers. J. Strength Cond. Res. 2010, 24, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, J.; Beaton, D.E.; Hogg-Johnson, S.; Bordeleau, L.J.; Goodwin, P.J. Three methods for minimally important difference: No relationship was found with the net proportion of patients improving. J. Clin. Epidemiol. 2007, 60, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Luoto, S.; Heliövaara, M.; Hurri, H.; Alaranta, H. Static back endurance and the risk of low-back pain. Clin. Biomech. 1995, 10, 323–324. [Google Scholar] [CrossRef]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Welch, N.; Moran, K.; Antony, J.; Richter, C.; Marshall, B.; Coyle, J.; Falvey, E.; Franklyn-Miller, A. The effects of a free-weight-based resistance training intervention on pain, squat biomechanics and MRI-defined lumbar fat infiltration and functional cross-sectional area in those with chronic low back. BMJ Open Sport Exerc. Med. 2015, 1, e000050. [Google Scholar] [CrossRef]
- Steiger, F.; Wirth, B.; De Bruin, E.D.; Mannion, A.F. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur. Spine J. 2012, 21, 575–598. [Google Scholar] [CrossRef]
- Mannion, A.F.; Junge, A.; Taimela, S.; Müntener, M.; Lorenzo, K.; Dvorak, J. Active therapy for chronic low back pain: Part 3. Factors influencing self-rated disability and its change following therapy. Spine (Phila. Pa. 1976) 2001, 26, 920–929. [Google Scholar] [CrossRef]
- Andersen, L.L.; Christensen, K.B.; Holtermann, A.; Poulsen, O.M.; Sjøgaard, G.; Pedersen, M.T.; Hansen, E.A. Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: A one-year randomized controlled trial. Man. Ther. 2010, 15, 100–104. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Graven-Nielsen, T. Muscle Pain: Sensory Implications and Interaction With Motor Control. Clin. J. Pain 2008, 24, 291–298. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Frequency | 3 days per week for 8 weeks. |
| Schedule | Sessions were performed at the same time of the day (i.e., during the morning) and were separated by 48 h (i.e., Monday, Wednesday, Friday). |
| Location | Sport facility in a primary care center. |
| Supervision | Sessions were supervised by a physical therapist, neither involved in the randomization nor in data collection. |
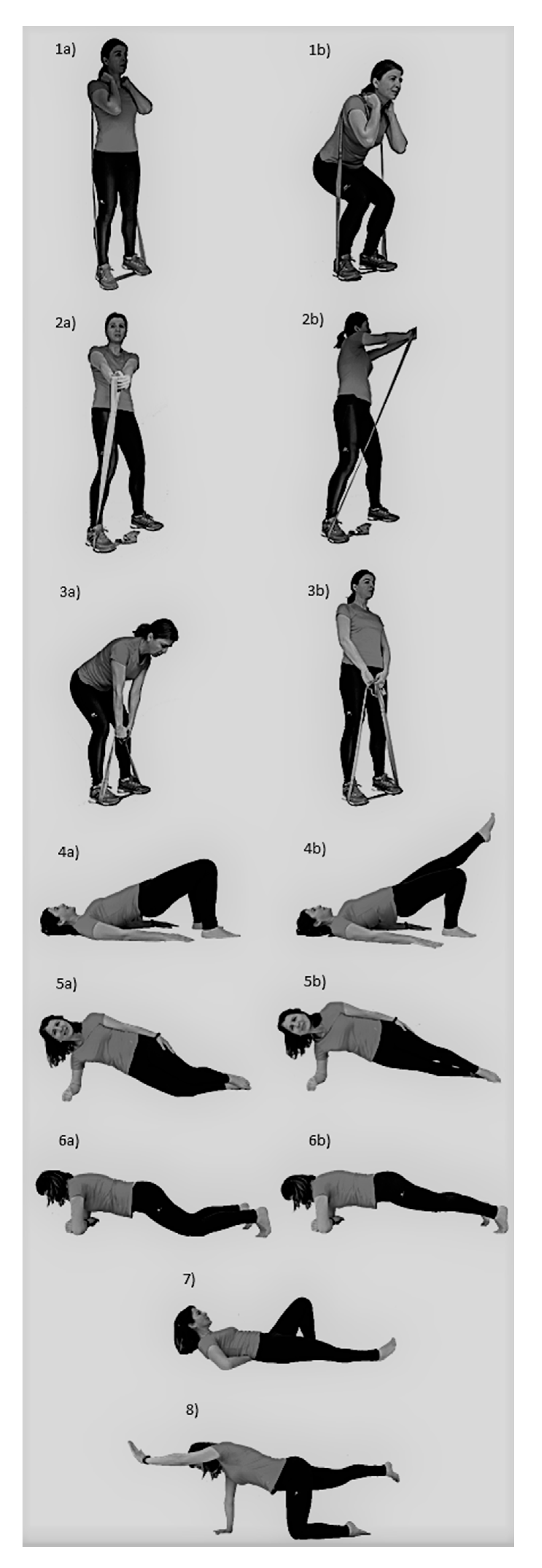
| Exercise order | In each session, the dynamic exercises were performed in a different order and in a circuit manner, switching from one exercise to the next so that the muscles were fatigued alternately and without rest between exercises. Secondly, five isometric plank exercises were performed. |
| Dynamic exercises | A warm up set was performed before each specific exercise by using light resistance to easily perform 10 repetitions without fatigue. Intensity progressively increased each two weeks, from 20 repetition-maximum (RM) to 10 RM (i.e., 20 RM, 15 RM, 12 RM, 10 RM). To achieve adequate exercise intensity during dynamic exercises, the elastic bands were pre stretched to approximately 50% of the initial length (initial length, 1.9 m) and then different bands were used/added when needed to reach the desirable intensity. For this purpose, red, blue, black, silver, and gold elastic band colors were available (TheraBand CLX, The Hygenic Corporation, Akron, OH, USA), alone or combined in parallel. Three sets of each exercise were performed. In these exercises, movement velocity was performed at a rate of approximately 1.5 s for concentric and 1.5 s for eccentric phases. In cases of pain, the intensity was reduced to the previous step or range of motion was restricted until pain decreased. |
| Isometric exercises | Intensity progression was based on reducing the base of support or focusing on activating the abdominal muscles. This progression was performed when subjects were able to do the basic exercise with the proper technique and during the required volume. In addition, training volume and thus total time under tension increased during the isometric exercises by progressively increasing the number of repetitions each two weeks: (1) 15 reps of 5 s (75 s total); (2) 20 reps of 5 s (100 s total); (3) 25 reps of 5 s (125 s total); (4) 30 reps of 5 s (150 s total). If subjects were not able to complete the exercise progression during the desired time due to pain, they had to return to the basic exercise. |
| n | Episodes | % | Relative Risk (95% Confidence Interval) | Chi-Square | p-value | Mean Days until First Recurrence Episode | |
|---|---|---|---|---|---|---|---|
| Control | 30 | 10 | 33.3 | 4 (1.2–13.2) | 5.2 | 0.02 | 57.8 |
| Intervention | 36 | 3 | 8.3 | 62.7 |
| Control | Intervention | Between-group Difference at Post | p-Value (Post) | Effect Size | % Change Control Group | % Change Intervention Group | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | ||||||||||
| Mean | SD | Mean | SD | Lower | Upper | ||||||
| Isometric Lumbar extension pre (s) | 25.97 | 29.93 | 34.61 | 28.6 | 42.8 | −61.4 | −24.1 | <0.001 | 1.50 | 14.25 | 128.26 |
| Isometric Lumbar extension post (s) | 29.67 | 28.06 | 79 | 58.19 | |||||||
| LBP intensity pre | 6.3 | 2 | 6.2 | 2 | 0.8 | −0.4 | 1.9 | 0.193 | 0.36 | −19.05 | −30.65 |
| LBP intensity post | 5.1 | 3 | 4.3 | 2 | |||||||
| Number of pain sites pre | 3.2 | 2.2 | 4.4 | 2.5 | 1 | 0.1 | 1.7 | 0.030 | 0.42 | −7.41 | −54.95 |
| Number of pain sites post | 3.0 | 2.4 | 2.0 | 2.4 | |||||||
| Analgesics pre (days/week) | 4.23 | 2.69 | 3.69 | 2.57 | 0.5 | −0.5 | 1.5 | 0.339 | 0.19 | −21.75 | −33.33 |
| Analgesics post (days/week) | 3.31 | 2.97 | 2.46 | 2.67 | |||||||
| Handgrip left hand pre (Kg) | 32.36 | 10.51 | 27.51 | 10.35 | 3.1 | −5.7 | −0.4 | 0.024 | 0.29 | 3.68 | 22.72 |
| Handgrip left hand post (Kg) | 33.55 | 10.6 | 33.76 | 12.39 | |||||||
| Handgrip right hand pre (Kg) | 31.73 | 10.28 | 28.3 | 10.65 | 1.4 | −3.9 | 1.1 | 0.259 | 0.14 | 3.47 | 13.25 |
| Handgrip right hand post (Kg) | 32.83 | 11.54 | 32.05 | 11.82 | |||||||
| Disability pre | 10.2 | 5.52 | 7.75 | 5.08 | 1.6 | −0.3 | 3.5 | 0.107 | 0.29 | −22.55 | −35.87 |
| Disability post | 7.9 | 5.35 | 4.97 | 4.2 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calatayud, J.; Guzmán-González, B.; Andersen, L.L.; Cruz-Montecinos, C.; Morell, M.T.; Roldán, R.; Ezzatvar, Y.; Casaña, J. Effectiveness of a Group-Based Progressive Strength Training in Primary Care to Improve the Recurrence of Low Back Pain Exacerbations and Function: A Randomised Trial. Int. J. Environ. Res. Public Health 2020, 17, 8326. https://doi.org/10.3390/ijerph17228326
Calatayud J, Guzmán-González B, Andersen LL, Cruz-Montecinos C, Morell MT, Roldán R, Ezzatvar Y, Casaña J. Effectiveness of a Group-Based Progressive Strength Training in Primary Care to Improve the Recurrence of Low Back Pain Exacerbations and Function: A Randomised Trial. International Journal of Environmental Research and Public Health. 2020; 17(22):8326. https://doi.org/10.3390/ijerph17228326
Chicago/Turabian StyleCalatayud, Joaquín, Benjamín Guzmán-González, Lars L. Andersen, Carlos Cruz-Montecinos, María Teresa Morell, Ricardo Roldán, Yasmín Ezzatvar, and José Casaña. 2020. "Effectiveness of a Group-Based Progressive Strength Training in Primary Care to Improve the Recurrence of Low Back Pain Exacerbations and Function: A Randomised Trial" International Journal of Environmental Research and Public Health 17, no. 22: 8326. https://doi.org/10.3390/ijerph17228326
APA StyleCalatayud, J., Guzmán-González, B., Andersen, L. L., Cruz-Montecinos, C., Morell, M. T., Roldán, R., Ezzatvar, Y., & Casaña, J. (2020). Effectiveness of a Group-Based Progressive Strength Training in Primary Care to Improve the Recurrence of Low Back Pain Exacerbations and Function: A Randomised Trial. International Journal of Environmental Research and Public Health, 17(22), 8326. https://doi.org/10.3390/ijerph17228326