A Review of Selected Studies on the Factors Associated with the Nutrition Status of Children Under the Age of Five Years in South Africa

Abstract
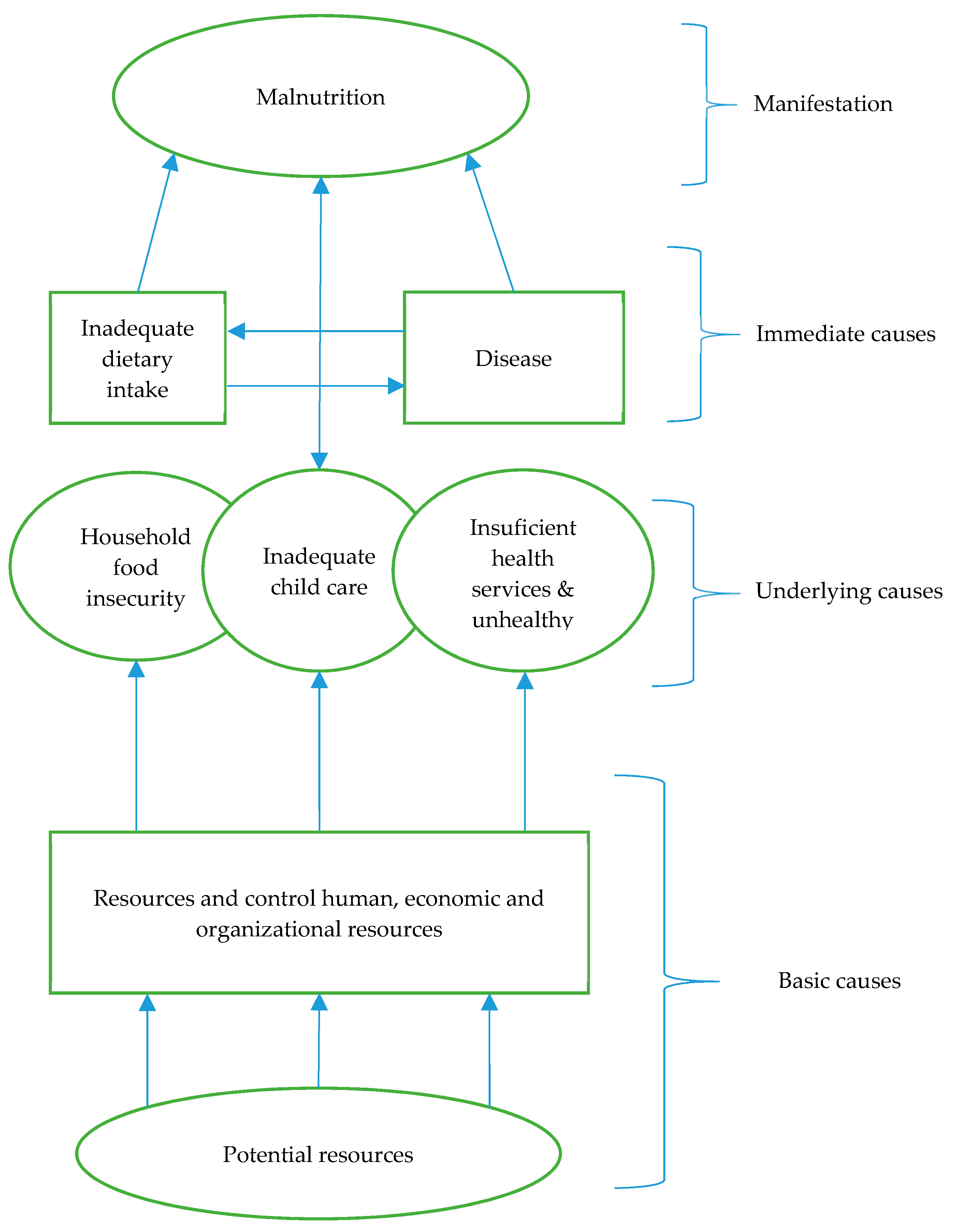
1. Introduction
2. Materials and Methods
2.1. The Inclusion and Eligibility Criteria
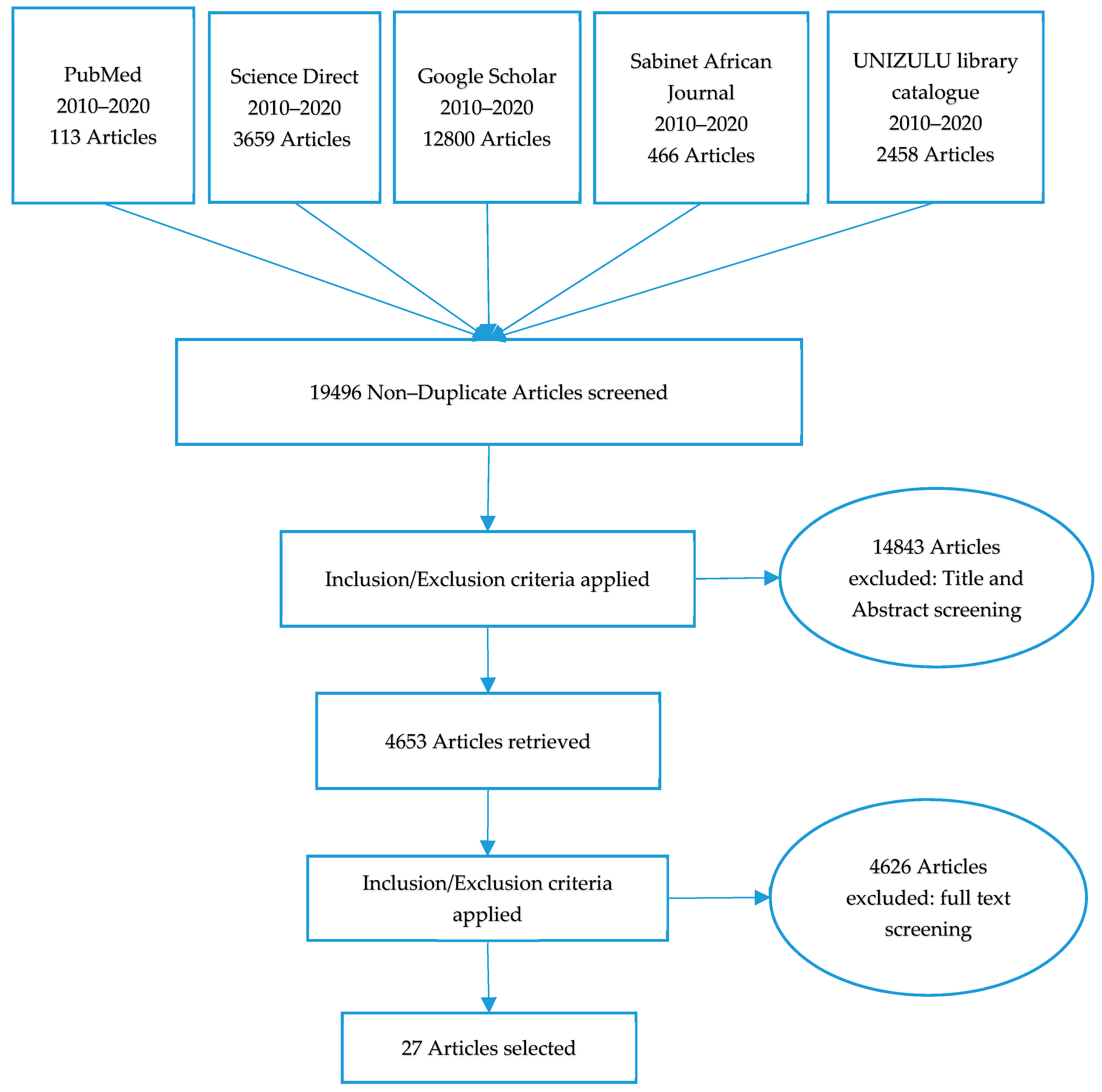
2.2. Search Strategy
2.3. Data Extraction and Analysis
3. Results
3.1. Description of the Methodological Design of Selected Studies
3.2. Geographical Distribution of the Reviewed Studies by Province
3.3. Geographical Classification of the Reviewed Studies (Rural or Urban)
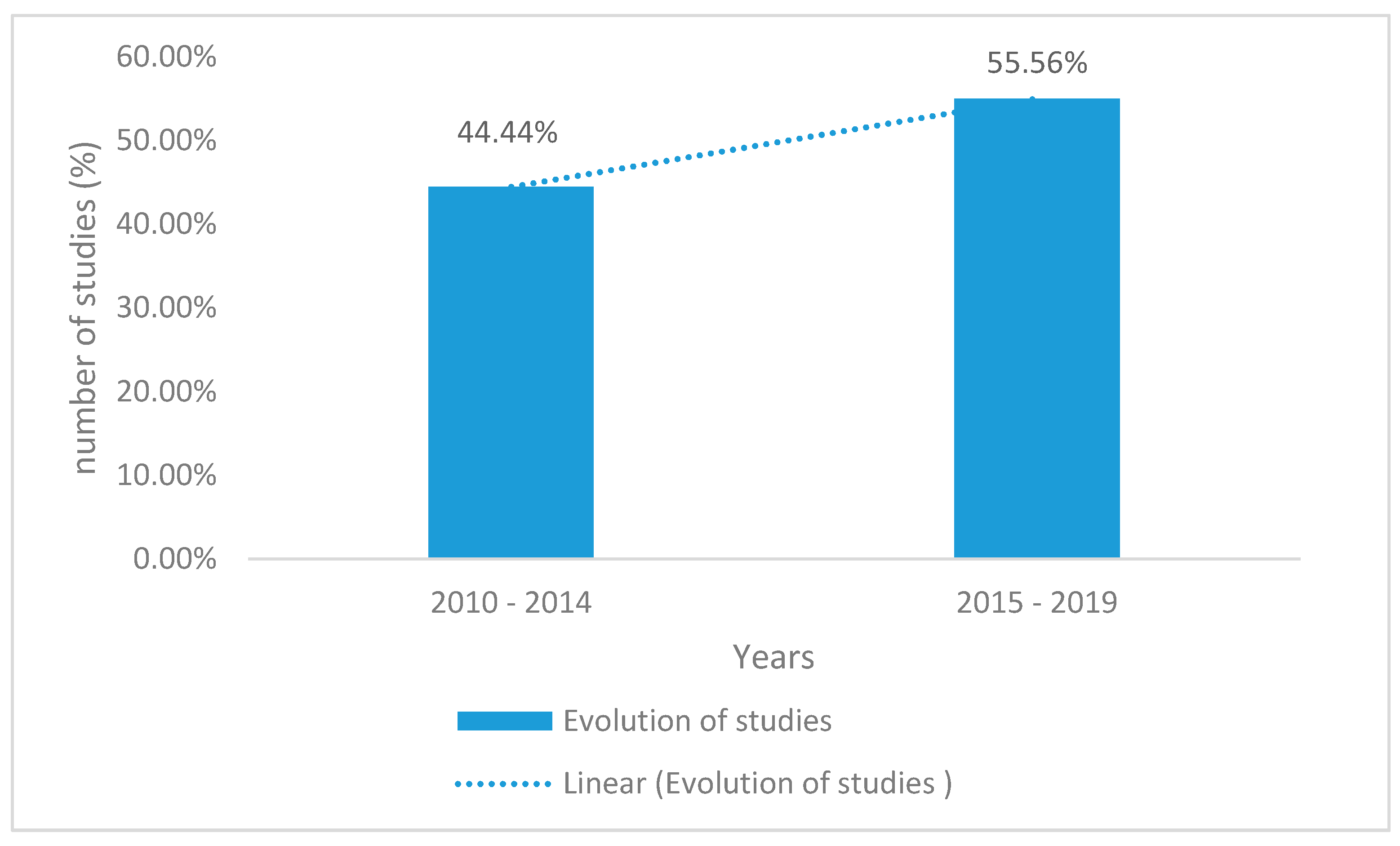
3.4. The Evolution of the Number of Studies on Child Nutritional Status in South Africa
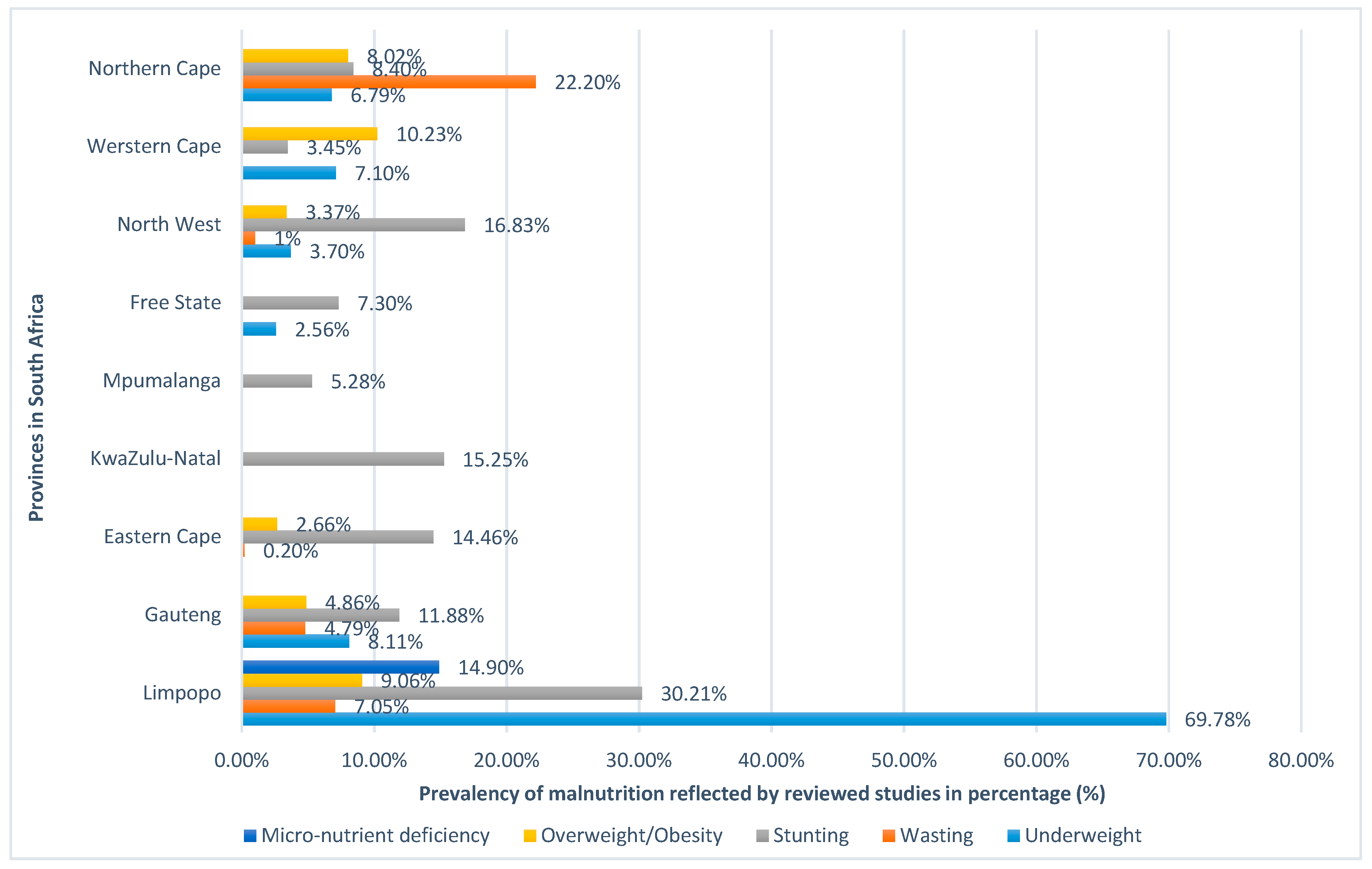
3.5. The Prevalence of Child Malnutrition in South Africa as Depicted by the Selected Studies
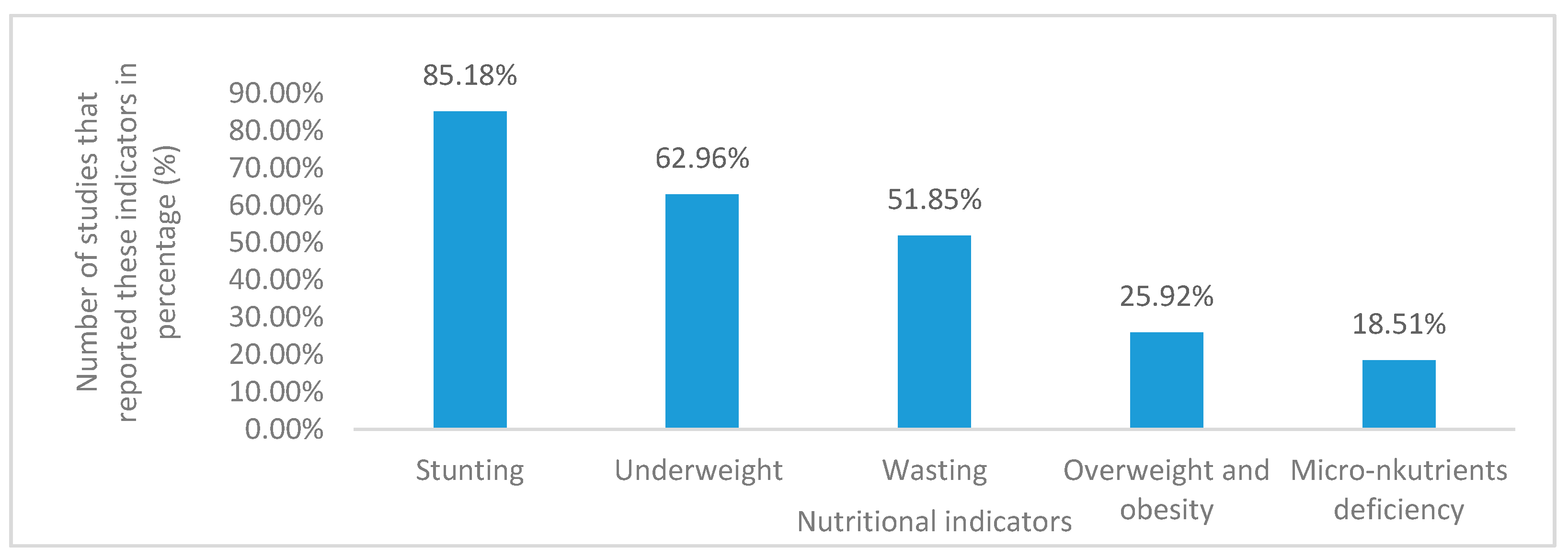
3.6. Nutritional Status Indicators in Children
3.7. Factors Influencing the Nutritional Status of Children
4. Discussion
4.1. Geographical Classification of the Reviewed Studies
4.2. Evolution of the Number of Studies on Child Nutritional Status in South Africa
4.3. The Prevalence of Child Malnutrition in South Africa
4.3.1. The Prevalence of Child Stunting in South Africa
4.3.2. The Prevalence of Underweight Children in South Africa
4.3.3. The Prevalence of Child Wasting in South Africa
4.3.4. The Prevalence of Overweightness and Obese Children in South Africa
4.3.5. The Prevalence of Micronutrient Deficiency of Children in South Africa
4.4. Factors Affecting the Nutritional Status of Children in South Africa
4.4.1. Food Insecurity
4.4.2. Household Income
4.4.3. Caregiver’s Level of Education
4.4.4. Household Unemployment
4.4.5. The Child’s Dietary Intake
4.4.6. Child Illness
4.4.7. Consumption of a Monotonous Diet
4.4.8. Poor Access to Water and Sanitation
4.4.9. Poor Weaning Practices
4.4.10. Gender and Age of the Child
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Isanaka, S.; Barnhart, D.A.; McDonald, C.M.; Ackatia-Armah, R.S.; Kupka, R.; Doumbia, S.; Brown, K.F.; Menzies, N.A. Cost-effectiveness of community-based screening and treatment of moderate acute malnutrition in Mali. BMJ J. 2019, 4, e001227. [Google Scholar] [CrossRef]
- dos Santos, N.A.; de Freitas, P.H.; Galdino, L.; dos Santos, B.; de Almeida, N.L.; Monteiro, T.; Frendes, P.; Andrade, M.J. Malnutrition and development of basic visual functions. Avidscience 2018, 4, 184–194. [Google Scholar]
- World Health Organisation. Available online: https://www.who.int/en/news-room/fact-sheets/detail/malnutrition (accessed on 27 July 2020).
- Mohammed, S.H.; Habtewold, T.D.; Muhammad, F.; Esmaillzadeh, A. The contribution of dietary and non-dietary factors to socioeconomic inequality in childhood anemia in Ethiopia: A regression-based decomposition analysis. BMC 2019, 12, 1–5. [Google Scholar]
- Akombi, B.J.; Agho, K.E.; Merom, D.; Renzaho, A.M.; Hall, J.J. Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006–2016). PLoS ONE 2017, 12, e0177338. [Google Scholar] [CrossRef]
- Beresford, A.; Berry, M.E.; Mann, L. Liberation movements and stalled democratic transitions: Reproducing power in Rwanda and South Africa through productive liminality. Democratisation 2018, 25, 1–20. [Google Scholar]
- Otterbach, S.; Rogan, M. Exploring spatial differences in the risk of child stunting: Evidence from a South African national panel survey. J. Rural Stud. 2019, 65, 65–78. [Google Scholar]
- Ndaguba, E.A. Community Economic Development Strategic Framework for Poverty Alleviation in Local Government in a Rural South Africa. Ph.D. Thesis, North-West University, Potchefstroom, South Africa, 2020. [Google Scholar]
- Statistics South Africa. Available online: www.statssa.gov.za/publications/P03101/P031012018.pdf (accessed on 3 October 2020).
- Monday, S.; Elijah, K.; Victor, M. Factors influencing malnutrition among under five children at kitwe teaching hospital, Zambia. Int. J. Curr. Res. 2018, 1, 9–18. [Google Scholar]
- World Bank. Available online: Documents.worldbank.org/curated/pt/... (accessed on 1 December 2019).
- Chakona, G.; Shackleton, C.M. Household food insecurity along an agro-ecological gradient influences children’s nutritional status in South Africa. Front. Nutr. 2018, 4. [Google Scholar] [CrossRef]
- Ilifa Labantwana. Available online: https://ilifalabantwana.co.za/sa-early-childhood-review-2019/ (accessed on 17 July 2020).
- Keding, G. Nutrition transition in rural Tanzania and Kenya. Hidden Hunger 2016, 115, 68–87. [Google Scholar]
- Modjadji, P.; Madiba, P. Childhood undernutrition and its predictors in a rural health and demographic surveillance system site in South Africa. Int. J. Environ. Res. Public Health 2019, 16, 3021. [Google Scholar] [CrossRef]
- Felixperspective. Available online: https://felixperspective.wordpress.com/2016/02/17/malnutrition-in-developed-countries/ (accessed on 30 November 2019).
- Caballero, B.; Vorkoper, S.; Anand, N.; Rivera, J.A. Preventing childhood obesity in Latin America: An agenda for regional research and strategic partnerships. Obes. Rev. 2017, 18, 3–6. [Google Scholar] [CrossRef]
- Aizawa, T. Ex-ante Inequality of Opportunity in Child Malnutrition: New evidence from ten developing countries in Asia. Econ. Hum. Biol. 2019, 35, 144–161. [Google Scholar] [CrossRef] [PubMed]
- Muse, T.B.; Wanjo, M.I.; Bala, E.T.; Desta, H.O. Assessment of prevalence and factors associated with malnutrition among under-five children in West Shoa Zone, Oromia Region, Ethiopia. Am. J. Health Res. 2019, 7, 59–66. [Google Scholar] [CrossRef]
- Tasnim, T. Determinants of malnutrition in children under five years in Developing Countries: A systematic review. Indian J. Public Health Res. Dev. 2018, 9, 333–338. [Google Scholar] [CrossRef]
- Oluwalana, E.O.; Shittu, A.M.; Olaomi, O.O. Determinants of nutritional status of pre-school children of farming households in southern parts of Nigeria. In Proceedings of the 18th Annual National Conference of the Nigerian Association of Agricultural Economists, Abeokuta, Nigeria, 16–19 October 2017. [Google Scholar]
- Action Against Hunger. Available online: https://actionagainsthunger.ca/what-is-acute-malnutrition/underlying-causes-of-malnutrition/ (accessed on 28 November 2019).
- Bernstein, L. The global problem of malnutrition. Nutr. Food Sci. 2017, 10, 2575–7091. [Google Scholar] [CrossRef]
- Ravindranath, D.; Trani, J.F.; Iannotti, L. Nutrition among children of migrant construction workers in Ahmedabad. Int. J. Equity Health 2019, 18, 143. [Google Scholar] [CrossRef]
- Slemming, W. Early Life Risks and Child Development. Ph.D. Thesis, University of Witwatersrand, Johannesburg, South Africa, 2017. [Google Scholar]
- Ntshebe, O. Three Papers on Households and Child Health in Botswana. Ph.D. Thesis, University of Southampton, Southampton, Botswana, 2017. [Google Scholar]
- Kazembe, L.N.; Nickanor, N. Spatial modelling of the relationship between socio-economic disadvantage and child health in Namibia. Spat. Demogr. 2017, 5, 1–24. [Google Scholar] [CrossRef]
- Schoeman, S.; Faber, M.; Adams, V.; Smuts, C.; Ford-Ngomane, N.; Laubscher, J.; Dhansay, M. Adverse social, nutrition and health conditions in rural districts of KwaZulu-Natal and the Eastern Cape provinces, South Africa. S. Afr. J. Clin. Nutr. 2013, 23. [Google Scholar] [CrossRef]
- Ntila, S.; Siwela, M.; Kolanisi, U.; Abdelgadir, H.; Ndhlala, A. An assessment of the food and nutrition security status of weaned 7–12 months old children in rural and peri-urban communities of Gauteng and Limpopo Provinces, South Africa. Int. J. Environ. Res. Public Health 2017, 14, 1004. [Google Scholar] [CrossRef]
- Madiba, S.; Chelule, P.K.; Mokgatle, M.M. Attending informal preschools and daycare centers is a risk factor for underweight, stunting and wasting in children under the age of five years in underprivileged communities in South Africa. Int. J. Environ. Res. Public Health 2019, 16, 2589. [Google Scholar] [CrossRef]
- MAL-ED Network investigators. Childhood stunting in relation to the pre-and postnatal environment during the first 2 years of life: The MAL-ED longitudinal birth cohort study. PLoS Med. 2017, 14. [Google Scholar] [CrossRef]
- Mushaphi, L.F.; Dannhauser, A.; Walsh, C.; Mbhenyane, X.; Van Rooyen, F. Effect of a nutrition education programme on nutritional status of children aged 3–5 years in Limpopo Province, South Africa. S. Afr. J. Child. Health 2015, 9, 98–102. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W. Exploring the paradox: Double burden of malnutrition in rural South Africa. J. Glob. Health 2013, 6, 19249. [Google Scholar] [CrossRef]
- De Lange, J.C. Factors Contributing to Malnutrition in Children 0-60 Months Admitted to Hospitals in the Northern Cape. Ph.D. Thesis, University of the Free State, Bloemfontein, South Africa, 2010. [Google Scholar]
- McLaren, S.; Steenkamp, L.; Feeley, A.; Nyarko, J.; Venter, D. Food insecurity, social welfare and low birth weight: Implications for childhood malnutrition in an urban Eastern Cape Province township. S. Afr. J. Child. Health 2018, 12, 95–99. [Google Scholar]
- Mahlangu, N.; Chelule, P. Food Security, Malnutrition and Health Status of Children under Five Years, Attending Rosslyn Mobile Clinic in Soshanguve Township, Gauteng Province, South Africa. Ph.D. Thesis, Sefako Makgatho Health Sciences University, Gauteng, South Africa, 2018. [Google Scholar]
- le Roux, I.M.; le Roux, K.; Comulada, W.S.; Greco, E.M.; Desmond, K.A.; Mbewu, N.; Rotheram-Borus, M.J. Home visits by neighborhood Mentor Mothers provide timely recovery from childhood malnutrition in South Africa: Results from a randomised controlled trial. J. Nutr. 2010, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Mandiwana, T.; Mahopo, T.; Nesamvuni, C.D. Household food access and nutritional status of 2–5 years old children residing in Vhembe district, Limpopo Province, South Africa. Afr. J. Phys. Health Educ. Recreat. Danc. 2015, 2, 273–279. [Google Scholar]
- Mushaphi, L.F. Impact of a Nutrition Education Programme on the Nutritional Status of Children Aged 3 to 5 Years and the Nutritional Practices and Knowledge of Their Caregivers in Rural Limpopo Province, South Africa. Ph.D. Thesis, University of the Free State, Bloemfontein, South Africa, 2011. [Google Scholar]
- Mabweazara, S.; Rivalani, D.; Tsolekile, L.; Leach, L.; Puoane, T. Nutritional knowledge amongst an adult South African sample of low socioeconomic status: Health. Afr. J. Phys. Act. Health Sci. 2018, 24, 638–648. [Google Scholar]
- Motadi, S.A.; Mbhenyane, X.G.; Mbhatsani, H.V.; Mabapa, N.S.; Mamabolo, R.L. Prevalence of iron and zinc deficiencies among pre-school children ages 3 to 5 y in Vhembe district, Limpopo province, South Africa. J. Nutr. 2015, 31, 452–458. [Google Scholar] [CrossRef]
- Matsungo, T.M.; Kruger, H.S.; Faber, M.; Rothman, M.; Smuts, C.M. The prevalence and factors associated with stunting among infants aged 6 months in a peri-urban South African community. Public Health Nutr. 2017, 20, 3209–3218. [Google Scholar] [CrossRef]
- Schoeman, S.; Smuts, C.; Faber, M.; Van Stuijvenberg, M.; Oelofse, A.; Laubscher, J.; Benade, A.J.; Dhansay, M.A. Primary health care facility infrastructure and services and the nutritional status of children 0 to 71 months old and their caregivers attending these facilities in four rural districts in the Eastern Cape and KwaZulu-Natal provinces, South Africa. S. Afr. J. Clin. Nutr. 2010, 23. [Google Scholar] [CrossRef]
- Lesiapeto, M.S.; Smuts, C.M.; Hanekom, S.M.; Du Plessis, J.; Faber, M. Risk factors of poor anthropometric status in children under five years of age living in rural districts of the Eastern Cape and KwaZulu-Natal provinces, South Africa. S. Afr. J. Clin. Nutr. 2010, 23. [Google Scholar] [CrossRef]
- Dukhi, N.; Sartorius, B.; Taylor, M. Stunting in children (0–59 months): What is the current trend in South Africa? Early Child. Dev. Care 2017, 187, 1874–1886. [Google Scholar] [CrossRef]
- Casale, D.; Desmond, C.; Richter, L. The association between stunting and psychosocial development among pre-school children: A study using the South African Birth to Twenty cohort data. Child. Care Health Dev. 2014, 40, 900–1000. [Google Scholar] [CrossRef]
- Selepe, B.M. The Impact of Home Gardens on Dietary Diversity, Nutrient Intake and Nutritional Status of Pre-school Children in a Home Garden Project in Eatonside, the Vaal Triangle, Johannesburg, South Africa. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2010. [Google Scholar]
- Kekana, M.J. The Nutritional Status of Children Less than 5 Years Receiving Child Support Grant in Mogalakwena Municipality, Waterberg District, Limpopo Province, South Africa. Ph.D. Thesis, University of Venda, Limpopo, South Africa, 2018. [Google Scholar]
- Nyati, L.H.; Pettifor, J.M.; Norris, S.A. The prevalence of malnutrition and growth percentiles for urban South African children. BMC Public Health 2019, 19, 492. [Google Scholar] [CrossRef] [PubMed]
- Koetaan, D.; Smith, A.; Liebenberg, A.; Brits, M.; Halkas, C.; Van Lill, M.; Joubert, G. The prevalence of underweight in children aged 5 years and younger attending primary health care clinics in the Mangaung area, Free State. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–5. [Google Scholar] [CrossRef]
- Phooko, D.A. The Relationship between Employment Status of the Mother, Household Hunger and Nutritional Status of Children in Sekhukhune District, Limpopo Province 2016. Ph.D. Thesis, University of Venda, Limpopo, South Africa, 2016. [Google Scholar]
- Battersby, J. Cities, planning and urban food poverty in Africa. In The Routledge Companion to Planning in the Global South; Routledge: London, UK, 2017; pp. 204–214. [Google Scholar]
- Zhou, S.; Ye, B.; Fu, P.; Li, S.; Yuan, P.; Yang, L.; Zhan, X.; Chao, F.; Zhang, S.; Wang, M.Q.; et al. Double Burden of malnutrition: Examining the growth profile and coexistence of undernutrition, overweight. J. Obes. 2020, 2020. [Google Scholar] [CrossRef]
- Garg, S. Impact of overpopulation on land use pattern. In Environmental and Agricultural Informatics: Concepts, Methodologies, Tools, and Applications; IGIGl: Haryana, India, 2020; pp. 1517–1534. [Google Scholar]
- Dodman, D.; Leck, H.; Rusca, M.; Colenbrander, S. African urbanisation and urbanism: Implications for risk accumulation and reduction. Int. J. Disaster Risk Reduct. 2017, 26, 7–15. [Google Scholar] [CrossRef]
- Muhammad, A.I.; Yunusa, I.; Bolori, M.T.; Ezeanyika, L.U.S.; Walla, H.A.; Gidado, Z.M. Malnutrition among children under 5 does not correlate with higher socio economic status of parents in rural communities. OALib J. 2017, 4, 1–15. [Google Scholar] [CrossRef]
- Pérez-Moreno, S.; Blanco-Arana, M.C.; Bárcena-Martín, E. Economic cycles and child mortality: A cross-national study of the least developed countries. Econ. Hum. Biol. 2016, 22, 14–23. [Google Scholar] [CrossRef]
- Small Business and Marketing Advice. Available online: https://brandongaille.com/15-cross-sectional-study-advantages-and-disadvantages/ (accessed on 28 January 2020).
- Future of Working. Available online: https://futureofworking.com/11-advantages-and-disadvantages-of-longitudinal-studies/ (accessed on 16 May 2020).
- Bobat, R. (Ed.) Clinical manifestations. In HIV Infection in Children and Adolescents; Springer: Gewerbestr, Switzerland, 2020; pp. 23–30. [Google Scholar]
- Szatmari, P.; Chawarska, K.; Dawson, G.; Georgiades, S.; Landa, R.; Lord, C.; Messsinder, D.S.; Thurm, A.; Halladay, A. Prospective longitudinal studies of infant siblings of children with autism: Lessons learned and future directions. Am. Acad. Child. Adolesc. Psychiatry 2016, 55, 179–187. [Google Scholar] [CrossRef]
- Khalid, H.; Gill, S.; Fox, A.M. Planning global aid for nutrition-specific and nutrition-sensitive interventions and proportion of stunted children across low-and middle-income countries: Does aid matter? Health Policy Plan. 2019, 34, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Centre for Disease Control and Prevention. Available online: https://www.cdc.gov/nutrition/micronutrient-malnutrition/micronutrients/index.html (accessed on 12 April 2020).
- Jeyakumar, A.; Nikam, S.; Nayak, S. Prevalence and risk factors of undernutrition among children less than 2 years in urban Slums of Pune, Maharashtra, India. Ecol. Food Nutr. 2019, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Battersby, J. MDGs to SDGs–new goals, same gaps: The continued absence of urban food security in the post-2015 global development agenda. Afr. Geogr. Rev. 2017, 36, 115–129. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Kahn, K.; Pettifor, J.M.; Tollman, S.M.; Dunger, D.B.; Gómez-Olivé, X.F.; Norris, S.A. The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children. BMC Public Health 2010, 10, 158. [Google Scholar] [CrossRef]
- Skoufias, E.; Vinha, K.; Sato, R. Stunting in Sub-Saharan African Countries. In All Hands on Deck, 2nd ed.; Skoufias, E., Vinha, K., Eds.; World Bank Vietnam: North Kivu Region, The Republic of Congo, 2019; Volume 10, pp. 45–55. [Google Scholar]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Ugboma, Z.; Agho, K.E. Stunting and severe stunting among infants in India: The role of delayed introduction of complementary foods and community and household factors. Glob. Health Action 2019, 12, 1638020. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Park, H.S. Relationship between underweight, bone mineral density and skeletal muscle index in premenopausal Korean women. Int. J. Clin. Pract. 2016, 70, 462–468. [Google Scholar] [CrossRef]
- Agho, K.E.; Akombi, B.J.; Ferdous, A.J.; Mbugua, I.; Kamara, J.K. Childhood undernutrition in three disadvantaged East African Districts: A multinomial analysis. BMC Pediatr. 2019, 19, 118. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Ba, D.M.; Ericson, J.E.; Na, M.; Gao, X.; Chinchilli, V.M. Pooled analysis of global, regional and country-level prevalence of childhood stunting, wasting and underweight in 62 low-and middle-income countries, 2006–2018. Regional country-level prevalence of childhood stunting, wasting underweight. Soc. Sci. Res. Netw. 2019, 62, 2006–2018. [Google Scholar]
- Emerson, E.; Savage, A.; Llewellyn, G. Prevalence of underweight, wasting and stunting among young children with a significant cognitive delay in 47 low-income and middle-income countries. J. Intellect. Disabil. Res. 2020, 64, 93–102. [Google Scholar] [CrossRef]
- World Health Organisation. Available online: https://www.who.int/topics/malnutrition/en/ (accessed on 20 June 2020).
- United Nation International Children Emergency Fund. Available online: https://www.unicef.org/reports/state-of-worlds-children-2019 (accessed on 23 November 2019).
- Harding, K.L.; Aguayo, V.M.; Webb, P. Factors associated with wasting among children under five years old in South Asia: Implications for action. PLoS ONE 2018, 13, e0198749. [Google Scholar] [CrossRef]
- Tariku, A.; Bikis, G.A.; Woldie, H.; Wassie, M.M.; Worku, A.G. Child wasting is a severe public health problem in the predominantly rural population of Ethiopia: A community based cross–sectional study. Arch. Public Health 2017, 75, 26. [Google Scholar] [CrossRef] [PubMed]
- Derso, T.; Tariku, A.; Biks, G.A.; Wassie, M.M. Stunting, wasting and associated factors among children aged 6–24 months in Dabat health and demographic surveillance system site: A community based cross-sectional study in Ethiopia. BMC Pediatr. 2017, 17, 96. [Google Scholar] [CrossRef]
- World Health Organisation. Available online: http://www.who.int/nutgrowthdb/estimates/en/ (accessed on 15 April 2020).
- De Vita, M.V.; Scolfaro, C.; Santini, B.; Lezo, A.; Gobbi, F.; Buonfrate, D.; Kimani-Murage, E.W.; Macharia, T.; Wanjohi, M.; Rovarini, J.M.; et al. Malnutrition, morbidity and infection in the informal settlements of Nairobi, Kenya: An epidemiological study. Ital. J. Pediatr. 2019, 45, 12. [Google Scholar] [CrossRef]
- Reuter, C.P.; de Mello, E.D.; da Silva, P.T.; Borges, T.S.; Klinger, E.I.; Franke, S.I.; Valim, A.R. Overweight and obesity in schoolchildren: Hierarchical analysis of associated demographic, behavioral, and biological factors. J. Obes. 2018, 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Tinky, C.; Sunita, M. Inherited factor related to childhood obesity and its prevention. Int. J. Res. Appl. Nat. Soc. Sci. 2017, 5, 2347–4580. [Google Scholar]
- Nutrition and Health. Available online: http://www.egyankosh.ac.in/bitstream/123456789/46632/1/Unit-15.pdf (accessed on 11 June 2020).
- Larqué, E.; Labayen, I.; Flodmark, C.E.; Lissau, I.; Czernin, S.; Moreno, L.A.; Pietrobelli, A.; Widhalm, K. From conception to infancy—Early risk factors for childhood obesity. Nat. Rev. Endocrinol. 2019, 15, 456–478. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Kavle, J.; Perry, A.; Nyaku, A. Programming maternal and child overweight and obesity in the context of undernutrition: Current evidence and key considerations for low-and middle-income countries. Public Health Nutr. 2017, 20, 1286–1296. [Google Scholar] [CrossRef]
- Cohen, E.; Gradidge, P.J.L.; Ndao, A.; Duboz, P.; Macia, E.; Gueye, L.; Boetsch, G.; Pasquet, P.; Holdsworth, M.; Chapuis-Lucciani, N. Biocultural determinants of overweight and obesity in the context of nutrition transition in Senegal: A holistic anthropological approach. J. Biosoc. Sci. 2019, 51, 469–490. [Google Scholar] [CrossRef]
- Ford, N.D.; Patel, S.A.; Narayan, K.V. Obesity in low-and middle-income countries: Burden, drivers, and emerging challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Templin, T.; Hashiguchi, T.C.O.; Thomson, B.; Dieleman, J.; Bendavid, E. The overweight and obesity transition from the wealthy to the poor in low-and middle-income countries: A survey of household data from 103 countries. PLoS Med. 2019, 16. [Google Scholar] [CrossRef]
- Ashdown-Franks, G.; Vancampfort, D.; Firth, J.; Veronese, N.; Jackson, S.E.; Smith, L.; Stubbs, B.; Koyanang, A. Leisure-time sedentary behavior and obesity among 116,762 adolescents aged 12–15 years from 41 low-and middle-income countries. J. Obes. 2019, 27, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Mtolo, A. Food Security and Coping Strategies of an Urban Community in Durban. Master’s Thesis, Durban University of Technology, Durban, South Africa, 2016. [Google Scholar]
- Lakshmi, A.J.; Prakash, J. Diet-related nutrition and health issues in Indian population. In Nutritional and Health Aspects of Food in South Asian Countries; Academic Press: Sri, India, 2020; pp. 11–29. [Google Scholar]
- Perez-Escamilla, R.; Bermudez, O.; Buccini, G.S.; Kumanyika, S.; Lutter, C.K.; Monsivais, P.; Victora, C. Nutrition disparities and the global burden of malnutrition. BMJ 2018, 361, 2252. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, M.; Harb, T.; David, M.; Davies, P.S.; Hill, R.J. Effect of fortified milk on growth and nutritional status in young children: A systematic review and meta-analysis. Public Health Nutr. 2017, 20, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- McQuade, E.T.R.; Clark, S.; Bayo, E.; Scharf, R.J.; DeBoer, M.D.; Patil, C.L.; Gratz, J.C.; Houpt, E.R.; Svensen, E.; Mduma, E.R.; et al. Seasonal food insecurity in Haydom, Tanzania, is associated with low birthweight and acute malnutrition: Results from the MAL-ED study. Am. J. Trop. Med. Hyg. 2019, 100, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Agho, K.E.; Mukabutera, C.; Mukazi, M.; Ntambara, M.; Mbugua, I.; Dowling, M.; Kamara, J.K. Moderate and severe household food insecurity predicts stunting and severe stunting among Rwanda children aged 6–59 months residing in Gicumbi district. Matern. Child. Nutr. 2019, 15, e12767. [Google Scholar] [CrossRef]
- Belayneh, M.; Loha, E.; Lindtjorn, B. Food insecurity, wasting and stunting among young children in a drought prone area in South Ethiopia: A cohort study (P04-040-19). Curr. Dev. Nutr. 2019, 3, 4–19. [Google Scholar] [CrossRef]
- Drammeh, W.; Hamid, N.A.; Rohana, A. Determinants of household food insecurity and its association with child malnutrition in sub-saharan africa: A review of the literature. Curr. Res. Nutr. Food Sci. 2019, 7, 610–623. [Google Scholar] [CrossRef]
- Momanyi, D.K.; Owino, W.O.; Makokha, A.; Evang, E.; Tsige, H.; Krawinkel, M. Gaps in food security, food consumption and malnutrition in households residing along the baobab belt in Kenya. Nutr. Food Sci. 2019, 49, 1099–1112. [Google Scholar] [CrossRef]
- Brown, M.E.; Backer, D.; Billing, T.; Grace, K. Modeling climate and conflict shocks on acute malnutrition in children. AGUFM 2019, 2019, 1172. [Google Scholar]
- Shinsugi, C.; Gunasekara, D.; Gunawardena, N.; Subasinghe, W.; Miyoshi, M.; Kaneko, S. Double burden of maternal and child malnutrition and socioeconomic status in urban Sri Lanka. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Chistian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 42–51. [Google Scholar]
- Asim, M.; Nawaz, Y. Child malnutrition in Pakistan: Evidence from literature. Children 2018, 5, 60. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Ali, D.; Duong, D.B.; Hajeebhoy, N.; Rawat, R.; Menon, P. What roles do women’s status and household food security play in relation to child nutrition in Vietnam. TW Devasahayam. In Ensuring A Square Meal: Women And Food Security In Southeast Asia; World Scientific: Toh Tuck, Singapore, 2018; pp. 123–146. [Google Scholar]
- Ji, M.; Zhang, Y.; Zou, J.; Yuan, T.; Tang, A.; Deng, J. Study on the status of health service utilisation among caregivers of left-behind children in poor rural areas of Hunan province: A baseline survey. Int. J. Environ. Res. Public Health 2017, 14, 910. [Google Scholar] [CrossRef]
- Phooko-Rabodiba, D.; Tambe, B.; Nesamvuni, C.; Mbhenyane, X. Socioeconomic determinants influencing nutritional status of children in sekhukhune district of Limpopo province in South Africa. J. Nutr. Health 2019, 5, 1–7. [Google Scholar]
- Fonyuy, B.E.; Jocelyne, M.T. Knowledge of Mothers and Caregivers on the Causes, Prevention and Consequences of Malnutrition in the Under-Fives. SciFed. J. Public Health 2018, 2, 17–26. [Google Scholar]
- Onyeneke, R.U.; Nwajiuba, C.A.; Igberi, C.O.; Umunna, A.M.; Anosike, F.C.; Oko-Isu, A.; Mononye, J.; Uwadoka, C.; Adeolu, A.L. Impacts of caregivers’ nutrition knowledge and food market accessibility on preschool children’s dietary diversity in remote communities in Southeast Nigeria. Sustainability 2019, 11, 1688. [Google Scholar] [CrossRef]
- Chege, P.M.; Kuria, E.N. Relationship between nutrition knowledge of care-givers and dietary practices of children under five in Kajiado County, Kenya. Women Health 2017, e43820. [Google Scholar] [CrossRef]
- Sinha, A.; McRoy, R.G.; Berkman, B.; Sutherland, M. Drivers of change: Examining the effects of gender equality on child nutrition. Child. Youth Serv. Rev. 2017, 76, 203–212. [Google Scholar]
- Statistics South Africa. Available online: http://www.statssa.gov.za/?s=unemployment (accessed on 8 April 2020).
- Pieters, J.; Rawlings, S. Parental unemployment and child health in China. Rev. Econ. Househ. 2020, 18, 207–237. [Google Scholar]
- Page, M.; Schaller, J.; Simon, D. The effects of aggregate and gender-specific labor demand shocks on child. J. Hum. Resour. 2019, 54, 37–78. [Google Scholar]
- Rashad, A.S.; Sharaf, M.F. Does maternal employment affect child nutrition status? New evidence from Egypt. Oxf. Dev. Stud. 2019, 47, 48–62. [Google Scholar] [CrossRef]
- Brauner-Otto, S.; Baird, S.; Ghimire, D. Maternal employment and child health in Nepal: The importance of job type and timing across the child’s first five years. Soc. Sci. Med. 2019, 224, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Manzione, L.C.; Kriser, H.; Gamboa, E.G.; Hanson, C.M.; Mulokozi, G.; Mwaipape, O.; Hoj, T.H.; Linehan, M.; Torres, S.; Hall, P.; et al. Maternal employment status and minimum meal frequency in children 6–23 months in Tanzania. Int. J. Environ. Res. Public Health 2019, 16, 1137. [Google Scholar] [CrossRef]
- Galgamuwa, L.S.; Iddawela, D.; Dharmaratne, S.D.; Galgamuwa, G. Nutritional status and correlated socioeconomic factors among pre-school and school children in plantation communities, Sri Lanka. BMC Public Health 2017, 17, 377. [Google Scholar] [CrossRef]
- Som, S.V.; Prak, S.; Laillou, A.; Gauthier, L.; Berger, J.; Poirot, E.; Wieringa, F.T. Diets and feeding practices during the first 1000 days window in the Phnom Penh and north eastern districts of Cambodia. J. Nutr. 2018, 10, 500. [Google Scholar] [CrossRef]
- Nasreddine, L.M.; Kassis, A.N.; Ayoub, J.J.; Naja, F.A.; Hwalla, N.C. Nutritional status and dietary intakes of children amid the nutrition transition: The case of the Eastern Mediterranean Region. Nutr. Res. 2018, 57, 12–27. [Google Scholar] [CrossRef]
- Boadu, I.; Ohemeng, A.; Renner, L.A. Dietary intakes and nutritional status of children with sickle cell disease at the Princess Marie Louise Hospital, Accra—A survey. BMC Nutr. 2018, 4, 33. [Google Scholar] [CrossRef]
- Bustan, M.N.; Akhsa, A.L.; Idris, A. Mapping Analysis of Low Birth Weight Babies in Makassar Municipality. In Proceedings of the 13th IEA SEA Meeting and ICPH-SDev, Andala University, West Sumatra, Indonesia, 18 August 2018. [Google Scholar]
- Trivedi, T.; Patel, V.; Subhash, R. Association between maternal factors and birth weight of children from a selected village of anand district. Research Reviews. Afr. J. Health Prof. Educ. 2019, 8, 21–40. [Google Scholar]
- Meshram, I.I.; Rao, K.M.; Balakrishna, N.; Harikumar, R.; Arlappa, N.; Sreeramakrishna, K.; Laxmaiah, A. Infant and young child feeding practices, sociodemographic factors and their association with nutritional status of children aged < 3 years in India: Findings of the National Nutrition Monitoring Bureau survey, 2011–2012. Public Health Nutr. 2019, 22, 104–114. [Google Scholar]
- Lestari, E.D.; Hasanah, F.; Nugroho, N.A. Correlation between non-exclusive breastfeeding and low birth weight to stunting in children. Paediatr. Indones. 2018, 58, 123–127. [Google Scholar] [CrossRef]
- Mustelin, L.; Hedman, A.M.; Thornton, L.M.; Kuja-Halkola, R.; Keski-Rahkonen, A.; Cantor-Graae, E.; Almqvist, C.; Birgegård, A.; Lichtenstein, P.; Mortensen, P.B.; et al. Risk of eating disorders in immigrant populations. Acta Psychiatr. Scand. 2017, 136, 156–165. [Google Scholar] [CrossRef]
- Oldenburg, C.E.; Guerin, P.J.; Berthé, F.; Grais, R.F.; Isanaka, S. Malaria and nutritional status among children with severe acute malnutrition in Niger: A prospective cohort study. Clin. Infect. Dis. 2018, 67, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Francisco, K.; Florence, K.; Wanzala, P. Risk factors for severe acute malnutrition among children aged 6-59 months admitted at Lubango Pediatric Hospital, Angola. Afr. Health Sci. 2018, 31, 1–12. [Google Scholar]
- Nagata, J.M.; Gippetti, J.; Wager, S.; Chavez, A.; Wise, P.H. Prevalence and predictors of malnutrition among Guatemalan children at 2 years of age. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, C.; Grandjean, P. Immunotoxicity: Impacts and research approaches. In Health Impacts of Developmental Exposure to Environmental Chemical, 2nd ed.; Kishi, R., Grandjean, P., Eds.; Springer: Mariana Bay Sands, Singapore, 2020; Volume 3, pp. 175–190. [Google Scholar]
- Panda, S.K.; Lakra, K.; Panda, S.C. Dietary diversity among women in the reproductive age group in urban field practice area, Vimszr, Burla. Int. J. Med. Bio. Stud. 2019, 3. [Google Scholar] [CrossRef]
- Blakstad, M.M.; Bellows, A.L.; Mosha, D.; Canavan, C.R.; Mlalama, K.; Kinabo, J.; Kruk, M.E.; Masanja, H.; Fawzi, W.W. Neighbour home gardening predicts dietary diversity among rural Tanzanian women. Public Health Nutr. 2019, 22, 1646–1653. [Google Scholar] [CrossRef]
- Shakya, P. Factors Associated with Nutritional Status of 6-59 Months Children in Harisiddhi Municipality, Lalitpur. Ph.D. Thesis, Tribhuvan University, Kirtipur, Nepal, 2017. [Google Scholar]
- Statistics South Africa. Available online: http://www.statssa.gov.za/?p=11757 (accessed on 19 July 2020).
- Otsuka, Y.; Agestika, L.; Sintawardani, N.; Yamauchi, T. Risk factors for undernutrition and diarrhea prevalence in an urban slum in Indonesia: Focus on water, sanitation, and hygiene. Am. J. Trop. Med. 2019, 100, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.; Bakchi, J.; Islam, F.; Imran, A. Sanitation practices and nutritional status of under five children in muradia and Pangashia Union, Patuakhali, Bangladesh. Eur. J. Prev. Med. 2019, 7, 84–89. [Google Scholar]
- Singh, K.M.; Ahmad, N.; Sinha, D.; Mishra, R. Factors affecting nutritional status of india: An economic analysis with special reference to agricultural performance. Mult. Sci. 2019, 9, 117–121. [Google Scholar]
- Schoenbuchner, S.M.; Dolan, C.; Mwangome, M.; Hall, A.; Richard, S.A.; Wells, J.C.; Khara, T.; Sonko, B.; Prentice, A.M.; Moore, S.E. The relationship between wasting and stunting: A retrospective cohort analysis of longitudinal data in Gambian children from 1976 to 2016. Am. J. Clin. Nutr. 2019, 110, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Syeda, B.; Agho, K.; Wilson, L.; Maheshwari, G.K.; Raza, M.Q. Relationship between breastfeeding duration and undernutrition conditions among children aged 0–3 Years in Pakistan. Int. J. Pediatrics Adolesc. Med. 2020, 2352–6467. [Google Scholar] [CrossRef]
- Olack, B.; Burke, H.; Cosmas, L.; Bamrah, S.; Dooling, K.; Feikin, D.R.; Talley, L.E.; Breiman, R.F. Nutritional status of under-five children living in an informal urban settlement in Nairobi, Kenya. J. Health Popul. Nutr. 2011, 29, 357–363. [Google Scholar] [PubMed]
- Afolabi, B.M.; Afolabi, T.M.; Ogunwale, A.; Aiyesetenikan, A. A 2-month intervention study of preventive clothing against mosquito bites among malnourished and well-nourished children under 5 years of age living on the Atlantic Ocean Coast of Lagos, Southwest Nigeria. Malar. J. 2020, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Mother and Child Nutrition. Available online: https://motherchildnutrition.org/malnutrition/about-malnutrition/impact-of-malnutrition.html (accessed on 27 November 2019).
- Kassie, G.W.; Workie, D.L. Determinants of under-nutrition among children under five years of age in Ethiopia. BMC Public Health 2020, 20, 1–11. [Google Scholar]
- Akhade, K.S.; Sankhe, L.R.; Akarte, S.V. Magnitude of malnutrition among underfive children in urban slums of commercial capital of India and its multifactorial causation: A community-based study. Fam. Med. Prim. Care 2019, 8, 3865–3870. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria for Including Literature Sources | Criteria for Excluding Literature Sources |
|---|---|
| Text documented in English | Text documented in languages aside from English |
| Focus is on factors that affect nutritional status | Focus is not on factors that affect nutritional status |
| Addresses at least one of the causes of child malnutrition identified by UNICEF’s theoretical framework of causes of child malnutrition | Addresses none of the causes of child malnutrition identified by UNICEF’s theoretical framework of causes of child malnutrition |
| Studies that provide detailed pertinent text needed for the review Peer-reviewed studies and articles Studies published from 2010 onwards | The text lacks pertinent details needed for review Studies and articles that are not peer-reviewed Studies published before 2010 |
| Name of Province | Frequency | Percentage (%) |
|---|---|---|
| Limpopo | 11 | 40.74 |
| Gauteng | 8 | 29.62 |
| Eastern Cape | 6 | 22.22 |
| KwaZulu-Natal | 6 | 22.22 |
| Mpumalanga | 4 | 14.81 |
| Free State | 3 | 11.11 |
| North West | 3 | 11.11 |
| Western Cape | 4 | 14.81 |
| Northern Cape | 3 | 11.11 |
| Total | 48 | 100 |
| Location Classification (Rural/Urban) | Nutritional Indicator/s | Factors Influencing the Nutritional Status | Reference (s)/Sources |
|---|---|---|---|
| Rural areas | Stunting, underweightness, wasting | Poor access to water and sanitation, unemployment, child illness, and household food insecurity. | Schoeman et al. [28] |
| Rural & peri-urban | Underweightness | Nutrition insecurity, unemployment, food insecurity, monotonous diet, and inadequate dietary intake. | Ntila et al. [29] |
| Urban, peri-urban, informal settlement | Stunting, underweightness, wasting, overweightness, and obesity | Low birth weight, child’s gender, child’s age, age of the caregiver, unemployment, low education level, attending pre-school, low household income, and poor weaning practices. | Madiba et al. [30] |
| Rural | Stunting | Short maternal weight, low socioeconomic status, food insecurity, child illness, and inadequate dietary intake. | MAL-ED Network Investigators [31] |
| Urban | Wasting | The use of tobacco during pregnancy, unwanted pregnancy, and maternal height. | Slemming [25] |
| Rural | Stunting, underweightness, wasting | Unemployment, low income, poverty, illiteracy, and lack of access to adequate clean water. | Mushaphi et al. [32] |
| Rural | Stunting, underweightness, wasting, overweightness, and obesity | Child’s HIV status, low birth weight, caregiver’s age, and area of residence. | Kimani-Murage [33] |
| Rural, urban | Stunting | Low household level, poor access to water and sanitation, low quality of food, illiterate, food insecurity, and monotonous diet. | Otterbach and Rogan [7] |
| Urban, Rural, Urban informal settlement | Stunting, underweightness, wasting, overweightness and obesity, and micronutrient deficiency | Low birth weight, inadequate dietary intake, low household income, food insecurity, unemployment, child age, low maternal weight during pregnancy, household size, poor nutritional education, monotonous diet, child illness, type of house, and maternal BMI. | De Lange [34] |
| Urban | Stunting, wasting, overweightness, and obesity | Low birth weight and food insecurity. | McLaren et al. [35] |
| Urban | Stunting, underweightness, wasting, overweightness, and obesity | Household food insecurity, child illness, attending crèche, unemployment, illiterate, gender, and poor feeding practices. | Mahlangu and Chelule [36] |
| Urban, informal urban settlement | Underweightness | Low birth weight, caregiver’s inadequate nutrition education, hygiene education, age of the child, inadequate toilet facilities, and household situated in informal settlements. | le Roux et al. [37] |
| Rural | Undernutrition, wasting, stunting | Household food insecurity, socioeconomic status, household size, food distribution, caregiver illiterate, and unemployment. | Mandiwana et al. [38] |
| Rural | Stunting, underweightness, wasting, overweightness and obesity, micronutrient deficiency | Unemployment, household food insecurity, poor caregiver nutritional knowledge, inadequate dietary intake, and caregiver illiteracy. | Mushaphi [39] |
| Peri-urban | Underweightness, overweightness/obesity | Poor caregiver nutritional knowledge, low household income, caregiver illiteracy, unemployment, and inadequate dietary intake. | Mabweazara et al. [40] |
| Rural | Wasting, stunting, underweightness, micronutrient deficiency | Child gender, household food insecurity, and food feeding practices | Motadi et al. [41] |
| Peri-urban | Stunting | Low birth weight, maternal height, child gender, and poor maternal nutrition during pregnancy. | Matsungo et al. [42] |
| Rural | Undernutrition, stunting | Household size, low household income, household food insecurity, poor household infrastructure, child illness, and poor access to water and sanitation. | Schoeman et al. [43] |
| Rural | Stunting, underweightness, overweight | Gender of the child, no regular source of income, child illness, caregiver’s illiteracy, household food insecurity, and mother’s perception about child growth. | Lesiapeto et al. [44] |
| Rural | Stunting | Gender of the child, household food insecurity, poor access to piped water, distance to a health facility, socioeconomic status, and caregiver illiteracy. | Dukhi et al. [45] |
| Urban | Stunting | Care-giver illiteracy, home environmental factors, and asset index. | Casale et al. [46] |
| Informal settlement | Underweightness, stunting | Inadequate dietary intake, household food insecurity, poor dietary diversity, low household income, and caregiver illiteracy. | Selepe [47] |
| Rural | Stunting, underweightness, wasting | Low purchasing power, poor caregiver nutritional knowledge, unemployment, inadequate dietary intake, caregiver illiteracy, and poor feeding practice. | Kekana [48] |
| Urban | Stunting, underweightness, wasting | Low levels of physical activities, micro-nutrient deficiency, and inadequate dietary intake. | Nyati et al. [49] |
| Rural | Underweightness | Low birth weight, child’s history of malnutrition, poor sanitation, expensive formula feed, and child HIV status. | Koetaan et al. [50] |
| Rural | Stunting, underweightness, wasting | Unemployment, low household income, household food insecurity, and consumption of monotonous diet | Phooko [51] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mkhize, M.; Sibanda, M. A Review of Selected Studies on the Factors Associated with the Nutrition Status of Children Under the Age of Five Years in South Africa. Int. J. Environ. Res. Public Health 2020, 17, 7973. https://doi.org/10.3390/ijerph17217973
Mkhize M, Sibanda M. A Review of Selected Studies on the Factors Associated with the Nutrition Status of Children Under the Age of Five Years in South Africa. International Journal of Environmental Research and Public Health. 2020; 17(21):7973. https://doi.org/10.3390/ijerph17217973
Chicago/Turabian StyleMkhize, Mbalenhle, and Melusi Sibanda. 2020. "A Review of Selected Studies on the Factors Associated with the Nutrition Status of Children Under the Age of Five Years in South Africa" International Journal of Environmental Research and Public Health 17, no. 21: 7973. https://doi.org/10.3390/ijerph17217973
APA StyleMkhize, M., & Sibanda, M. (2020). A Review of Selected Studies on the Factors Associated with the Nutrition Status of Children Under the Age of Five Years in South Africa. International Journal of Environmental Research and Public Health, 17(21), 7973. https://doi.org/10.3390/ijerph17217973