Abstract
Physical activity (PA) refers to any action produced by skeletal muscle that consumes energy. According to the World Health Organization (WHO), PA is the primary element that can improve health at the community level. Obviously, PA plays an important role in the social, physical, and mental development of men and women, as well as in balancing weight. However, the large-scale negative impacts of physical inactivity on health-related issues are also recognized globally, such as obesity, which is the source of many non-communication diseases (NCDs). In Pakistan alone, 46% of deaths occur due to NCD. The majority of NCD deaths are linked to obesity, and Pakistan is the ninth most obese country in the world. Research on obesity caused by sedentary work in Pakistan is lacking, especially among university employees. To fill this gap, the current study mainly focuses on the rising non-communicable disease (NCD) rates among university employees in Pakistan due to a lack of exercise (obesity, in this case), with the help of a self-designed knowledge, attitude, and practice (KAP) questionnaire. Five universities in the Sindh province of Pakistan were surveyed (n = 276), following the concept of Yin–Yang as a theoretical lens. The results of the current study show that the knowledge, behaviors, and attitudes of university employees have a great influence on their body mass index (BMI). The study shows that Pakistani residents’ (especially teaching staff) perceptions and attitudes towards obesity and PA have been instructive, but their practices need to be improved.
1. Introduction
Physical activity (PA) refers to any physical activity produced by the skeletal muscles that consumes energy. According to the World Health Organization (WHO), the first sign of health at the community level is PA [1]. It is clear that PA plays a crucial role in social and physical development. In addition, PA has been used to maintain weight loss and weight gain and provides physical, social, emotional, and cognitive benefits [2,3]. On the other hand, governments have also recognized the large-scale negative impacts of physical inactivity on health-related problems worldwide. In developing and developed countries, chronic health conditions and non-communication diseases, such as obesity, are mainly associated with physical inactivity [4,5]. Hypertension, hyperglycemia, smoking, obesity, and a lack of physical exercise are the five major causes of death [6]. It is noteworthy that men self-reported a decrease in occupational, domestic, transportation, and leisure PA from 350 MET (metabolic equivalent) hours per week in 1997 to 253 MET hours per week in 2006. Women’s PA decreased from 390 MET working hours per week in 1996 to 246 MET working hours in 2006.
Obesity is considered to be the primary cause for many non-communication diseases (NCDs), including diabetes, hypertension, osteoporosis, and stroke [7]. Obesity is a complex disease involving excess body fat, which has a lack of physical exercise as one of the main causes [8]. As mentioned earlier, this is a medical problem that increases the risk of developing other diseases and health problems, such as heart disease, diabetes, hypertension, and some cancers [7]. Obesity is calculated by body mass index (BMI). WHO has developed different BMI guidelines for the global population and South Asia [9]. For the global population, WHO uses a number of 25 for normal BMI, which ranges from 25 to 30 for overweight, 30 to 35 for class I obesity, 35 to 40 for class II obesity, and 40 or more for obese people in class III. However, in South Asian countries, a normal BMI is 23, overweight is 23–27.5, class I obesity is 27.5–32.5, class II obesity is 32.5–37.5, and the BMI of the class III obese population is 37.5 or above (Table 1). However, the BMI does not measure body fat directly, so some people, like body-builders, may be categorized as obese even if they do not have excess body fat.

Table 1.
Body mass index (BMI) to diagnose obesity (global and South Asia).
Taking into account the WHO guidelines on BMI in South Asia as a standard, the Hayatabad Medical Complex, Pakistan Endocrine Society (PES), University of Manchester, University of Glasgow, and Khyber Medical College University conducted a real-time study in Pakistan of 19,000 subjects across the country, showing that 29% of the Pakistani population is obese, with 31% suffering from class I obesity, 13% from class II obesity, and 7% from class III obesity [9]. This indicates that the obesity rate is 20% higher than that of 31% for the rest of the world (20% in class I, 7% in class II, and 7% in class III). Pakistan is the ninth most obese country in the world, and around 3.4 million Pakistani people died because of obesity in 2010 alone [10]. The risk factors of obesity have been interpreted as a high-fat diet, sedentary work, and motor transport [11]. According to Farooq et al., the main reason for the increase in obesity in Pakistan is a lack of exercise [12]. Among Pakistan’s growing population, there is an urgent need to increase the ratio of PA to reduce obesity. As Professor Dr. AH Amir from Hayatabad Medical complex told the participants at the PES’ fifth annual mid-summer endocrine conference, “This real-time research survey provides the most reliable data on obesity prevalence in Pakistan, so it should be used as a call for action” [9].
The main object of this study is to highlight the rising obesity rates among university employees in Pakistan due to a sedentary lifestyle. Then, the focus is shifted to overcoming this problem mainly by participating in physical activities. In the current study, the impact of physical activities on the obesity of university employees is measured with the help of a self-designed knowledge attitude and practice (KAP) questionnaire, which is used to enhance the knowledge, attitudes, and practices of specific themes [13,14,15,16]. We used Yin–Yang theory (discussed in the “Methods” section in more detail) as the theoretical framework of the current study, which helped in developing the questionnaire survey. The current study offers a fresh understanding of the relationship between the obesity ratio and physical activity participation rate of Pakistani university employees.
2. Studies on Obesity in Pakistan
Pakistan is the sixth most populous country in the world, with an urban population of 39.1% [10]. Pakistan is a developing country and is facing many crises in the field of health due to a lack of awareness. In 2015, there were around 56.4 million deaths worldwide, among which 70% died of non-communicable diseases. In total, 1.6 million died of obesity-related health problems [10]. Obesity is often accompanied by other diseases, and many studies have shown that obesity is a major cause of non-communicable diseases, leading to serious cardiovascular problems, diabetes, and premature death [17,18,19]. In Pakistan, 46% of deaths are caused by NCDs, comprising around 380,000 males and 300,000 females, and the majority of NCD deaths are related to obesity [17,18,19,20]. The main causes of overweight and obesity in Pakistan are unawareness, high-density diet consumption, and physical inactivity. Notably, studies have shown that people living in Pakistan’s big cities are more likely to be obese than those in rural areas [21]. However, there are few studies in Pakistan on the link between a lack of physical exercise and obesity, especially among university employees. A few empirical studies have been conducted [10,17], but the existing literature may oversimplify the relationship between overweight and sedentary work among university employees. Some studies have focused on the difference between overweight and obesity between urban and rural residents, finding that residents living in urban areas are more likely to be overweight or obese than residents living in rural areas, and a parallel gap was drawn between the workload of employees and sports participation [19,22].
3. Methods
A knowledge attitude practice (KAP) survey was conducted as the main method of the current study. The KAP survey is a quantitative method that provides access to quantitative and qualitative information. It reveals what was said, but there may be considerable gaps between what is said and what is done [23]. The KAP survey also helps to identify what is known and done about various health-related subjects and helps to measure the effectiveness of health education activities to change health-related behaviors [13,14,15,16].
3.1. Questionnaire Survey
A self-designed KAP questionnaire was used as a survey tool and was designed from the existing literature, previous data, and our own previous research-related experience and knowledge [13,14,15,16,24]. This questionnaire was designed in the English language, which is the second most spoken, as well as the official, language in Pakistan. We completely followed the relevant ethical considerations. All participants gave their consent for participation before the starting the survey. The protocol of the study was approved by the Institutional Review Board of School of Sports Science and Physical Education, Nanjing Normal University, China.
During the questionnaire survey, the purpose, theme, scope, and objectives of the study were described, and it was made clear that participation was voluntary. In this study, research data were kept private, and the identities of the participants were not revealed. Each questionnaire took 15–20 min to complete for one participant. The questionnaire contained closed- and open-ended questions, such as “what are the health problems that can occur when a person is overweight or obese?”, “do you think Physical inactivity is one of the main reasons for obesity?”, “how often do you consume fast/junk/sugary/oily food or soft drinks?”, “at what time do you usually finish your dinner?”, “is PA is important to you?”, “do you participate in any PA”, and so on. Five universities (i.e., 1. Hamdard University, 2. University of Karachi, 3. Isra University, 4. University of Sindh, and 5. Sukkur Institute of Business Administration) were selected via the random sampling method. These universities are located in the four largest districts in Sindh province, which is the 2nd largest province in Pakistan (Figure 1). On this basis, scattered universities were randomly selected from the Sindh province of Pakistan. From each university, 60 employees were surveyed. First, participants were contacted through our own personal links and connections. These participants then reached out to other participants with the help of snowball sampling [24,25]. The validity measures of the current survey included training the interviewers, pilot studies, and inspecting the quality of the data collection. We measured the Cronbach’s alpha value to evaluate the reliability of the questionnaire. The value was 0.78, which indicates that the internal consistency was acceptable [26].
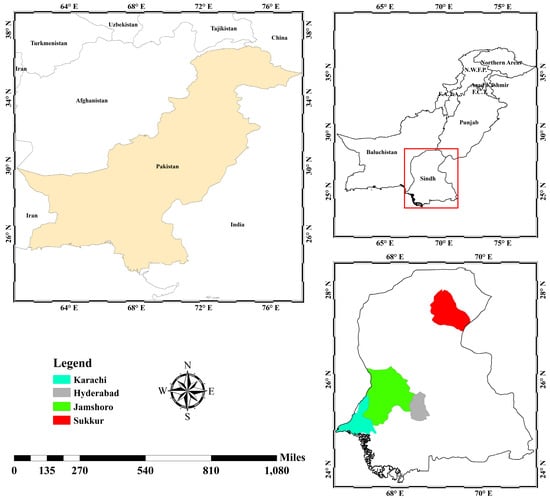
Figure 1.
Study area map (authors’ illustration designed with ArcGIS 10.5).
3.2. Statistical Analysis
After collecting the data and using Amos, 276 valid responses were left (n = 276), giving a 92% response rate (Table 2). The data were analyzed through SPSS Statistics 20 and Amos 24. Risk factor analysis and logistic regression were applied to explore the association between the obesity, BMI, and KAP scores of the participants. In the current study, we hypothesized that there would be significant differences in the level of obesity and physical activity knowledge between teaching and administration staff. We also hypothesized that people living in Pakistan’s big cities would be more likely to be obese than those in small cities and that the ratio of males in Pakistan participating in physical activities would be greater than that of females. We were inspired by the ideology of Yin–Yang, which is the theoretical lens of the current study.
Table 2.
Characteristics of the sample.
3.3. Theoretical Framework
Like other studies [27,28] in different countries, the current study also applies the Yin–Yang concept as a theoretical framework. Yin–Yang theory is a kind of logic that views elements in relation to their whole. Usually, Yang is associated with the functional aspect of an object and has more energetic qualities, such as moving, ascending, expanding, progressing, and acting. Yin, on the other hand, is associated with the less energetic qualities, such as stillness, descending, and under-functioning states (Figure 2). Yin and Yang also apply to the human body. In traditional Chinese medicine, good health is directly related to the balance between Yin and Yang qualities within oneself [29]. If the Yin and Yang become unbalanced, one of the qualities is considered deficient or has vacuity. Yin–Yang theory is applied to the current study through the idea that one’s eating habits and physical activity should be balanced to avoid complications such as obesity [30]. A basic scientific rule is that every action has a reaction: if a person is physically inactive and has unhealthy eating habits, their energy stores will increase, which will cause obesity, and vice versa (see Figure 2). This research provides several opportunities to understand the current situation of Pakistan, especially the participation of Pakistani university employees in physical activities and the ratio of obesity. Notably, this type of data is generally difficult to access in Pakistan, especially from female participants, which makes this material extremely valuable.
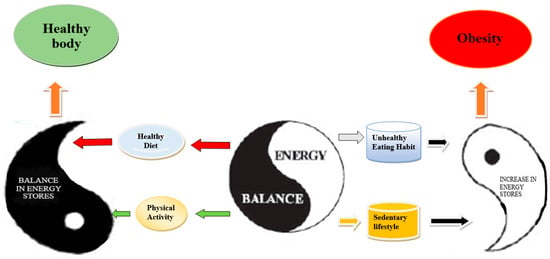
Figure 2.
Yin–Yang model of energy balance.
4. Results
4.1. BMI of the Sample
The BMIs of the participants were measured according to the standard values from WHO (see Table 1). More than half of the population (63%) suffers from obesity of class I, II, or III, respectively. The results also show that almost 16% of the population seems to be overweight (Table 3).
Table 3.
Body mass index (BMIs) of the participants.
4.2. Association between Obesity and KAP Score
Logistic regression was applied to explore the association between obesity and KAP scores adjusted by personal characteristics. The results showed that the KAP score has significant effects on increasing or decreasing obesity among university employees. We observed that the lower scores of the female participants impacted their obesity more compared to the male participants. As the education level rises, the KAP score also rises, which results in a normal body weight. This is the reason why, in our study, the teaching staff seemed to have healthier bodies compared to the administration staff. All the results were significant (p < 0.05, Table 4).
Table 4.
Affiliation of the KAP score with the obesity of university employees.
4.3. Risk Factor Analysis
We compared the scores of the knowledge, attitudes, and practices (KAP) questions with BMI levels. A correlation matrix was used for the risk perception analysis [31,32]. In the current research, the correlation coefficient was analyzed to identify any possible significant relationships between the variables (see Table 5).
Table 5.
Correlation between the knowledge, attitude, and practice scores of the participants and their BMI levels.
According to the results, there is a significant correlation between dietary and PA practice scores and BMI levels. This indicates that practices like not eating/eating less fast/junk/sugary/oily food or soft drinks in one’s daily diet, finishing eating dinner 6 h before sleeping, and frequently engaging in physical activities resulted in healthy individuals with a good BMI level. A significant correlation was found between the cause and prevention of obesity knowledge and the attitude scores of the participants with BMI levels. Better self-awareness regarding the risks of overweight and obesity, knowledge of the causes of overweight and obesity, the importance of PA in daily life, and maintaining a balanced diet could help to make these people healthier and stronger.
4.3.1. Obesity and Physical-Activity-Related Knowledge
Table 6 shows the correct responses of the participants from knowledge section (see also [33]). The majority of university employees have a good understanding about prevention steps (65%) to address obesity and its health problems (47%). However, results show that the participants have little knowledge about physical inactivity as a reason behind obesity (Table 6).
Table 6.
University employees’ knowledge of effects of physical activities and healthy eating habits on obesity.
On the other hand, to compare the knowledge levels of the teaching and administration staff, this study analyzed the correct responses of the participants related to obesity and physical activity knowledge in the shape of the mean, standard deviation, and percentage within the element. The results show that—as hypothesized—there is significant difference in the level of obesity and physical activity knowledge between teaching and administration staff (p < 0.05, see Table 7). The obesity and physical activity knowledge levels of teaching staff are better than those of the administration staff. This shows that the teaching staff understand the health problems of overweight and obesity and the prevention steps to overweight and obesity and consider physical inactivity to be the main reason for obesity. This is the reason why, according to the results, the teaching staff are comparatively less overweight or obese, more active in participating in physical activities, and lead healthier lives.
Table 7.
Obesity and physical-activity-related knowledge—occupation-wise classification.
4.3.2. Obesity and Physical-Activity-Related Attitudes
Table 8 elaborates the questions regarding participants’ attitudes towards the impact of physical activities and healthy eating habits on obesity [34]. Almost 58.70% of the population agree or strongly agree on the idea that obesity is very serious condition. Meanwhile, more than 55% of the university employees showed negative attitudes towards eating less and engaging in some physical activity or exercise (see Table 8).
Table 8.
University employees’ attitudes towards the impact of physical activities and healthy eating habits on obesity.
Meanwhile, the mean, standard deviation, and p value of each variable (obesity and PA-related attitudes) were analyzed to compare the obesity and PA-related attitudes of the respondents from different cities. With the help of an independent-sample t-test (comparing all cities one by one with each other), we determined the significance (two-tailed) of each city. There was not a significant difference in each city’s obesity and PA-related attitude responses (p > 0.05 see Table 9). However, Jamshoro and Sukkur are smaller cities than Karachi and Hyderabad. Nevertheless, among the compared means between the small and big cities, no significant difference was found (p > 0.05) between these cities. Thus, we reject the null hypothesis (HA) that people living in Pakistan’s big cities are more likely to be obese than those in small cities. This result indicates that, whether they live in small or big cities, there is not a large difference between people’s ideas and attitudes towards PA and obesity (Table 9).
Table 9.
Multi-comparison of the obesity and physical-activity-related attitudes of respondents from big and small cities.
4.3.3. Obesity and Physical-Activity-Related Practice
We have summarized the practices of university employees regarding the impact of physical activity and healthy eating habits on obesity in Table 10 (see also [34]). Results showed that most employees have fair knowledge and positive attitude about the impact of physical activity and healthy eating habits on obesity; however, they have a very low level of practicing these in their daily routines (only 15.22% participate in PA; see Table 10).
Table 10.
University employees’ practice on effects of physical activities and healthy eating habits on obesity.
In addition, we ran crosstabs, compared the means, and performed independent-sample t-tests to analyze the ratio of males and females, calculate the means, and observe the significance (two-tailed), respectively. The study showed that almost 85% of the total population agrees or strongly agrees that sports is important in their lives. More than half of the population, 128 (82.5%) participants, was male, and 104 (85.9%) were female (Table 11). Despite the fact that everyone agreed or strongly agreed with the importance of PA participation, 83.9% of males and 86% of females claimed to not participate in any PA, with a p value greater than 0.05 (p > 0.05), which indicates that the groups are not significantly different. Thus, we reject our hypothesis (HA) that the ratio of males in Pakistan participating in physical activities would be greater than that of females. Out of the 15.2% of the population that claimed to participate in physical activities, 4.7% performed PA once a week, and only 2.2% performed it four or more times per week. Moreover, 35.5% of the male and 43% of the female population declared that fatigue from their job and their workload were the main reasons that they did not participate in physical activities. Laziness was also one of the main reasons that participants did not participate in physical activities (male = 41.3% and females = 36.6%, see Table 11). Regarding practices to control obesity with the help of diet, more than 64% of the participants ate fast/junk/sugary/oily food or soft drinks either daily or once–twice a week, comprising 68.6% of the female population and 61.9 of the male population. On the other hand, only 7.2% of the participants consumed no fast/junk/sugary/oily food or soft drinks in their diets, and only 2.2% ate their dinner between 5 and 6 p.m.
Table 11.
Obesity and physical-activity-related practices—gender-wise distribution.
5. Discussion
At present, data on the knowledge, attitudes, and practices related to physical activities and obesity are still lacking. This study is the first to highlight university employees’ KAP about PA and obesity in Pakistan using the concept of the Yin–Yang model. The purpose of the current study was to identify the impact of physical activities on obesity through a KAP survey among university employees in Pakistan. According to the basic principles of the KAP survey, an improvement in knowledge will lead to a modification of attitudes and behaviors, thereby reducing the burden of disease and promoting a healthy lifestyle [11,35,36]. In addition, the KAP model emphasizes the beneficial effects of physical practices on health promotion, disease management, and risk reduction [37]. According to the WHO, the head of the household plays a major role in determining health policies for the family and society and has a significant impact on the health of current and future generations [38]. Therefore, this study selected teachers and other faculty members from different universities, who are considered as important guides that can lead their households and society towards a healthy lifestyle.
We found that the knowledge about the impact of physical activities on obesity was reasonable. This result indicates that participants understand the consequences of a sedentary lifestyle and were aware that engaging in physical activity and eating a healthy diet can overcome obesity. Only 6.8% of the respondents indicated that they did not know the correlation between physical activity and obesity. Among the respondents, the ratio of the administration staff (5.5%) was higher than that of the teaching staff (2%), possibly because the administration staff among our participants were not as highly educated or had less scientific knowledge about the human body compared to the teaching staff. According to Bookari et al. [39], knowledge can be the main factor in moving towards a healthier lifestyle. A good attitude is also the foundation of good behavior. A positive attitude helps to improve the level of knowledge and produce appropriate behavior. In this study, most of the participants showed a very positive attitude towards participating in physical activities, and most of them agreed to reduce or control their obesity levels. Positive attitude and knowledge can lead towards the Yang (functional or physically active in this case) part of the Yin–Yang concept. According to the results, there is not a significant difference in obesity and PA-related attitudes between big (Karachi and Hyderabad) and small (Jamshoro and Sukkur) cities (see Table 6). This indicates that, regardless of whether they live in small or big cities, all respondents had positive attitudes towards PA and obesity-controlling behaviors. As far as practice is concerned, we found that most of the participants (84.8%), despite their high level of knowledge and positive attitudes, did not participate in physical activities at all; the ratio of females was higher than that of males. These results contradict those of some other studies, which argue that an improvement in knowledge will lead to changes in attitudes and behaviors and that knowledge may be the main factor leading to changes in people’s behaviors and habits [11,35,36,39]. On the other hand, fewer members of the population engage in good/healthy eating habits to control overweight or obesity. For example, 64% of the participants consumed fast/junk/sugary/oily food or soft drinks either daily or once–twice a week, and most of the employees (81.5%) finished their dinner at 8–9 or after 9 p.m., which is not the healthiest time according to WHO guidelines [38]. These results support the Yin concept, which is related to less energetic qualities, sedentary lifestyle, and unhealthy eating habits. Furthermore, the results showed that only 21% of the participating university employees had a normal weight, while most of the participants (63.1%) were categorized under various classes of obesity (Class I-III). Notably, these results agree with those of some other studies [9,10], showing that 73% of the population suffers from obesity of at least one class (class I–III). This makes Pakistan the ninth most obese country in the world. The present study reveals that most university employees in the surveyed areas of Pakistan suffer from obesity problems because of their eating habits and sedentary lifestyles.
This KAP study provides a better understanding of university employees’ behaviors towards obesity and PA by implementing the concept of Yin–Yang and offers valuable information about the knowledge levels among teaching and administration staff, the attitudes of people in big and small cities, and gender-wise differences in their practical habits. These results could be used to plan lifestyle-counselling programs for employees with obesity and/or sedentary lifestyle issues. The results of this study may be significant for future obesity control and enhancing physical activity policies. Research that focuses on institutions such as universities may play a significant role in health promotion and the prevention of health problems. There are, however, some limitations to this study. This study used a KAP survey, which is a first-generation approach in health behavior research. Recently, third-generation theory-based methods and fourth-generation multi-theory-based methods have been used in health-related research. This KAP survey used predefined questions to capture information on the important knowledge, attitudes, and practices related to the most common eating habits and sedentary lifestyle issues [40]. The area (Sindh province, Pakistan) is large, but the sample size was relatively small, which could have affected the accuracy and reliability of the survey. As a result, the investigators were trained to control the data. Female participants also spoke to a male surveyor. Indeed, the female respondents, who were voluntary participants, felt relaxed and did not seem conservative when talking to the male researchers. Generally, in Pakistani society, it is difficult to obtain information from universities, especially when the participants include females. Our first attempt was met with many rejections. Lastly, the socio-cultural and religious characteristics of the selected sample were homogeneous, which may have resulted in bias. The investigators attempted to recognize any biases to avoid such results.
6. Conclusions
This study on university employees in Pakistan living in Sindh province is the first to use the KAP model based on Yin–Yang theory. In this study, we examined the influence of physical activity participation knowledge, attitudes, and practices (KAP) among university employees on obesity in Pakistan. The research results clearly show that university employees in Pakistan, especially teaching staff, have a good level of knowledge regarding obesity, its causes, and the consequences of physical inactivity. Most employees have a positive attitude about not being overweight or obese by maintaining healthy eating habits and know that they should participate in physical activities; however, they have a very low level of practically applying this knowledge. In terms of the Yin–Yang concept, the knowledge and attitude of Pakistani university employees towards the logic of Yin is very much clear and positive but the practice towards its functional part (Yang) needs to be improved. Furthermore, this study shows that the knowledge, practices, and attitudes of university employees largely affect their BMI status. This study shows that the awareness and attitude of Pakistani residents about obesity and PA is constantly increasing, but their practices need to be improved. Further studies should be conducted to investigate the reasons for not practicing these activities. For example, despite having positive attitudes and sufficient knowledge that participating in physical activities is good for mental and physical development and that obesity is one of the most fatal NCDs, why do Pakistani individuals not adopt healthy eating styles and participate in physical activities?
Author Contributions
Conceptualization, R.A.L.; Methodology, R.A.L.; Supervision, S.S.; Validation, M.N.K., J.B. and Y.L.; Writing—original draft, R.A.L.; Writing—review and editing, M.A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors thank the participants who made this study possible.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sadrollahi, A.; Hosseinian, M.; Alavi, N.M.; Khalili, Z.; Esalatmanesh, S. Physical activity patterns in the elderly kashan population. Iran. Red Crescent Med. J. 2016, 18, e25008. [Google Scholar] [CrossRef] [PubMed]
- Mirsafian, H.; Dóczi, T.; Mohamadinejad, A. Attitude of Iranian female university students to sport and exercise. Iran. Stud. 2014, 47, 951–966. [Google Scholar] [CrossRef]
- Rasberry, C.N.; Lee, S.M.; Robin, L.; Laris, B.; Russell, L.A.; Coyle, K.K.; Nihiser, A.J. The association between school-based physical activity, including physical education, and academic performance: A systematic review of the literature. Prev. Med. 2011, 52, S10–S20. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.; Sallis, R.; Hutber, A.; Archer, E. Exercise therapy–the public health message. Scand. J. Med. Sci. Sports 2012, 22, e24–e28. [Google Scholar] [CrossRef]
- Paterson, D.H.; Jones, G.R.; Rice, C.L. Ageing and physical activity: Evidence to develop exercise recommendations for older adults. Appl. Physiol. Nutr. Metab. 2007, 32, S69–S108. [Google Scholar] [CrossRef]
- World Health Organization. Medical Eligibility Criteria for Contraceptive Use; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Research and Education at Mayo Clinic. 2020. Available online: https://www.mayo.edu/ (accessed on 25 August 2020).
- Alfonzo, M.; Guo, Z.; Lin, L.; Day, K. Walking, obesity and urban design in Chinese neighborhoods. Prev. Med. 2014, 69, S79–S85. [Google Scholar] [CrossRef]
- Tay, C. Half of Pakistan’s Population Found to Be Obese and Facing High Diabetes Risk; Nutra Ingredients-Asia: Crawley, UK, 2018. [Google Scholar]
- Siddiqui, M.; Hameed, R.; Nadeem, M.; Mohammad, T.; Simbak, N.; Latif, A.; Abubakar, Y.; Baig, A. Obesity in Pakistan; current and future perceptions. J. Curr. Trends Biomed. Eng. Biosci. 2018, 17, 1–4. [Google Scholar]
- World Health Organization. Putting China’s rising burden of chronic disease on the agenda. In Non-Communicable Diseases; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Butt, F.; Butt, A.F.; Alam, F.; Aslam, N.; Moeed, H.A.; Butt, F.A. Perception and Management of Obesity Among Pakistani Doctors. Cureus 2019, 11, e4156. [Google Scholar] [CrossRef]
- Alsulami, A.N.J.; Alshehri, A.A.; Alghamdi, E.A.; Alsefry, F.S.A.; Mansoor, S.T. Assessment of Knowledge and Attitude and Practice of Family Towards Physical Activity in Makkah City, 2017. Egypt J. Hosp. Med. 2018, 70, 1093–1096. [Google Scholar] [CrossRef]
- Fatema, K.; Hossain, S.; Natasha, K.; Chowdhury, H.A.; Akter, J.; Khan, T.; Ali, L. Knowledge attitude and practice regarding diabetes mellitus among Nondiabetic and diabetic study participants in Bangladesh. BMC Public Health 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Gillani, A.H.; Amirul Islam, F.M.; Hayat, K.; Atif, N.; Yang, C.; Chang, J.; Qu, Z.; Fang, Y. Knowledge, attitudes and practices regarding diabetes in the general population: A cross-sectional study from Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 1906. [Google Scholar] [CrossRef]
- Ramezankhani, A.; Motalebi, M.; Tavassoli, E.; Heydarabadi, A.B.; Barekati, H.; Gilasi, H.R.; Moosavi, S.A. The Study of Knowledge, attitude and practice towards physical activity and its Related Factorsof College Students Living on Campus in Shahid Beheshti University of medical science. Arch. Adv. Biosci. 2013, 4, 62–67. [Google Scholar]
- Choo, V. WHO reassesses appropriate body-mass index for Asian populations. Lancet 2002, 360, 235. [Google Scholar] [CrossRef]
- Eckel, R.H. Obesity and heart disease: A statement for healthcare professionals from the Nutrition Committee, American Heart Association. Circulation 1997, 96, 3248–3250. [Google Scholar] [CrossRef] [PubMed]
- Worldometers. Worldometers Info Pakistan Population. Available online: https://www.worldometers.info/demographics/pakistan-demographics/ (accessed on 30 December 2018).
- Kuczmarski, R.J.; Flegal, K.M.; Campbell, S.M.; Johnson, C.L. Increasing prevalence of overweight among US adults: The National Health and Nutrition Examination Surveys, 1960 to 1991. JAMA 1994, 272, 205–211. [Google Scholar] [CrossRef]
- Laar, R.; Zhang, J.; Yu, T.; Qi, H.; Ashraf, M.A. Constraints to women’s participation in sports: A study of participation of Pakistani female students in physical activities. J. Int. J. Sport Policy Polit. 2019, 11, 385–397. [Google Scholar] [CrossRef]
- Tanzil, S.; Jamali, T. Obesity, an emerging epidemic in Pakistan-a review of evidence. J. Ayub Med. Coll. Abbottabad 2016, 28, 597. [Google Scholar]
- Du Monde, M. The KAP Survey Model (Knowledge, Attitudes & Practices); USAID: Washington, DC, USA, 2011.
- Laar, R.A.; Shi, S.; Ashraf, M.A. Participation of Pakistani Female Students in Physical Activities: Religious, Cultural, and Socioeconomic Factors. Religions 2019, 10, 617. [Google Scholar] [CrossRef]
- Ashraf, M.A. Exploring the Potential of Religious Literacy in Pakistani Education. Religions 2019, 10, 429. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53. [Google Scholar] [CrossRef]
- Zigman, J.M.; Elmquist, J.K. Minireview: From anorexia to obesity—The yin and yang of body weight control. Endocrinology 2003, 144, 3749–3756. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.-O.; Kim, W.-K.; Sim, S.-A. Effect of the Yin-Yang Constitution Diet on Metabolic Syndrome Biomarkers in Obese Adults. J. East Asian Soc. Diet. Life 2013, 23, 282–296. [Google Scholar]
- Li, C.-L. A brief outline of Chinese medical history with particular reference to acupuncture. Perspect. Biol. Med. 1974, 18, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Spiegelman, B.M.; Flier, J.S. Obesity and the regulation of energy balance. Cell 2001, 104, 531–543. [Google Scholar] [CrossRef]
- Dholakia, U.M. An investigation of the relationship between perceived risk and product involvement. ACR North Am. Adv. 1997, 24, 159–167. [Google Scholar]
- Weerasekara, P.C.; Withanachchi, C.R.; Ginigaddara, G.; Ploeger, A. Food and Nutrition-Related Knowledge, Attitudes, and Practices among Reproductive-Age Women in Marginalized Areas in Sri Lanka. Int. J. Environ. Res. Public Health 2020, 17, 3985. [Google Scholar] [CrossRef]
- Zeng, Y.; Hu, X.; Li, Y.; Zhen, X.; Gu, Y.; Sun, X.; Dong, H. The quality of caregivers for the elderly in long-term care institutions in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2019, 16, 2164. [Google Scholar] [CrossRef]
- Tang, Q.; Lin, Q.; Yang, Q.; Sun, M.; Liu, H.; Yang, L. Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition. Int. J. Environ. Res. Public Health 2020, 17, 4003. [Google Scholar] [CrossRef]
- Kigaru, D.M.D.; Loechl, C.; Moleah, T.; Macharia-Mutie, C.; Ndungu, Z.W. Nutrition knowledge, attitude and practices among urban primary school children in Nairobi City, Kenya: A KAP study. BMC Nutr. 2015, 1, 44. [Google Scholar] [CrossRef]
- Xu, X.; Chen, C.; Abdullah, A.S.; Liu, L.; Sharma, M.; Li, Y.; Zhao, Y. Smoking related attitudes, motives, and behaviors of male secondary school students in an urban setting of China. SpringerPlus 2016, 5, 2021. [Google Scholar] [CrossRef]
- Kamp, B. Position of the American Dietetic Association, American Society for Nutrition, and Society for Nutrition Education: Food and nutrition programs for community-residing older adults. J. Am. Diet. Assoc. 2010, 110, 463–472. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Healthy Nutrition: The Role of Women: Report on a WHO Meeting, Murmansk, Russian Federation 14–15 June 2000; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Bookari, K.; Yeatman, H.; Williamson, M. Exploring Australian women’s level of nutrition knowledge during pregnancy: A cross-sectional study. Int. J. Womens Health 2016, 8, 405. [Google Scholar] [CrossRef] [PubMed]
- Mohd Shariff, Z.; Lin, K.G.; Sariman, S.; Lee, H.S.; Siew, C.Y.; Mohd Yusof, B.N.; Mun, C.Y.; Mohamad, M. The relationship between household income and dietary intakes of 1–10 year old urban Malaysian. Nutr. Res. Pract. 2015, 9, 278–287. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).