Double Eyelid Tape Wear Affects Anterior Ocular Health among Young Adult Women with Single Eyelids


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Study Location
2.3. Participant Selection
2.4. Study Procedures
2.5. Statistical Analysis
3. Results
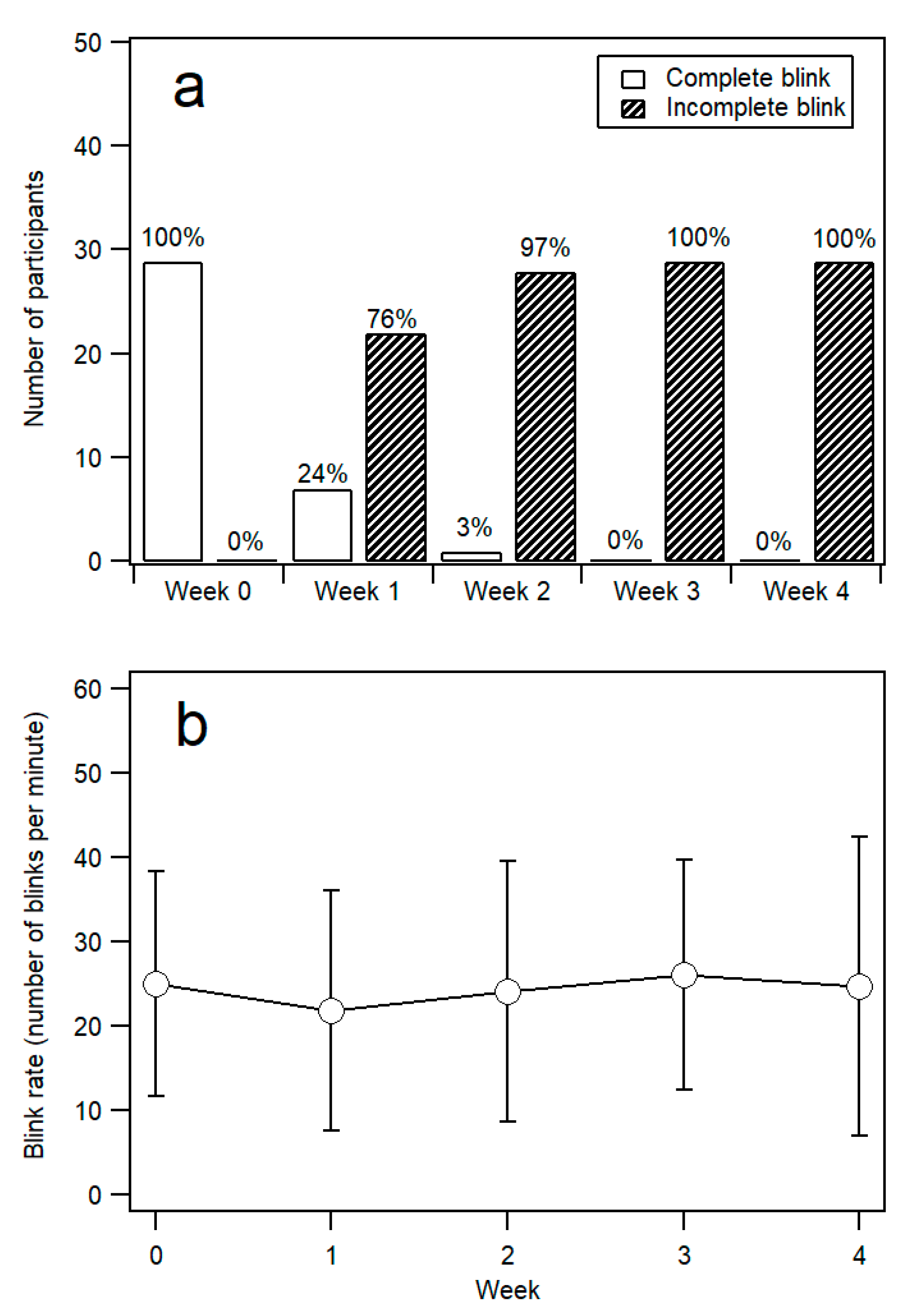
3.1. Blink Characteristics
3.2. Ocular Surface Health
3.2.1. Corneal Abrasion
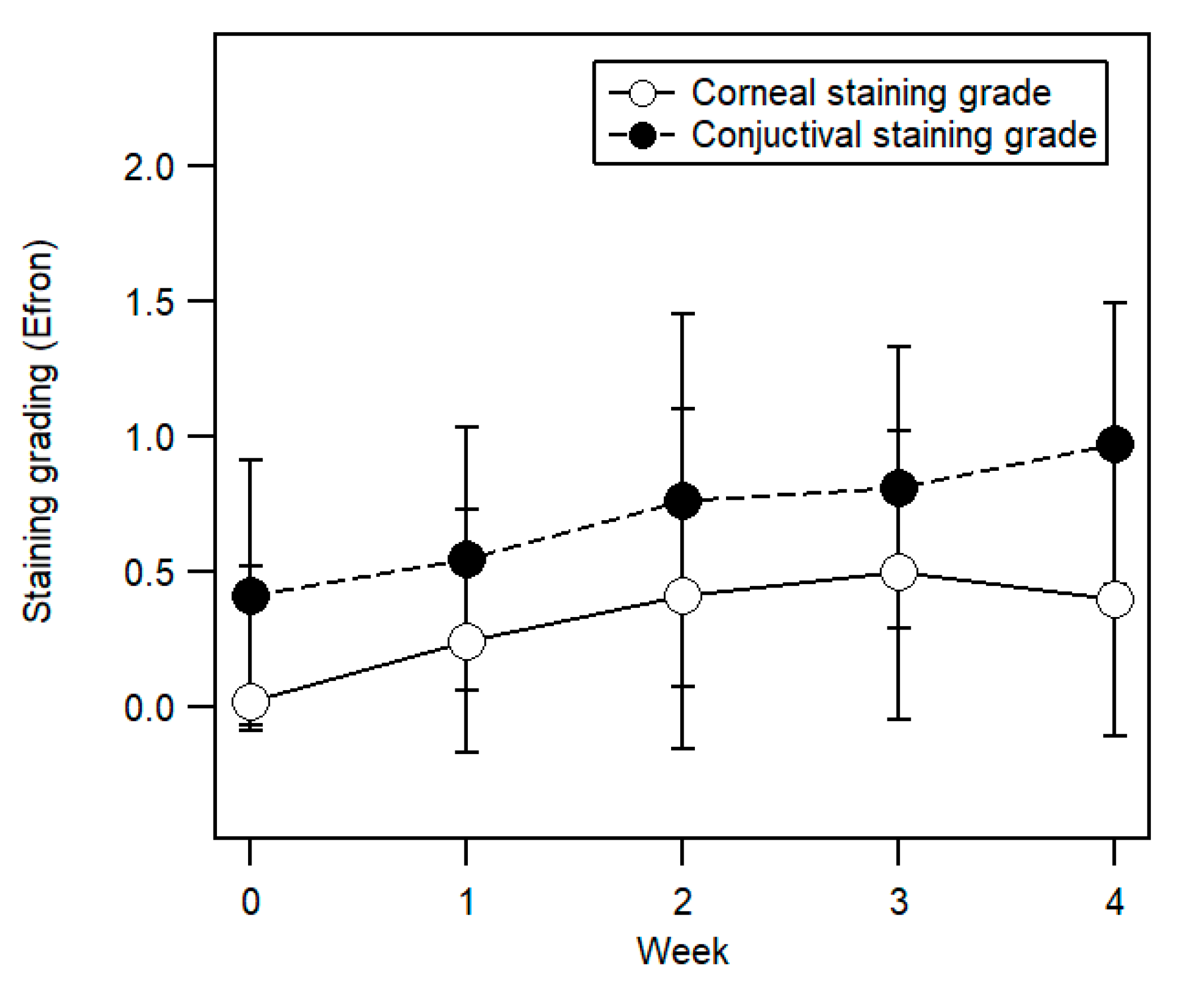
3.2.2. Corneal and Conjunctival Staining
3.2.3. Horizontal and Vertical Corneal Curvature
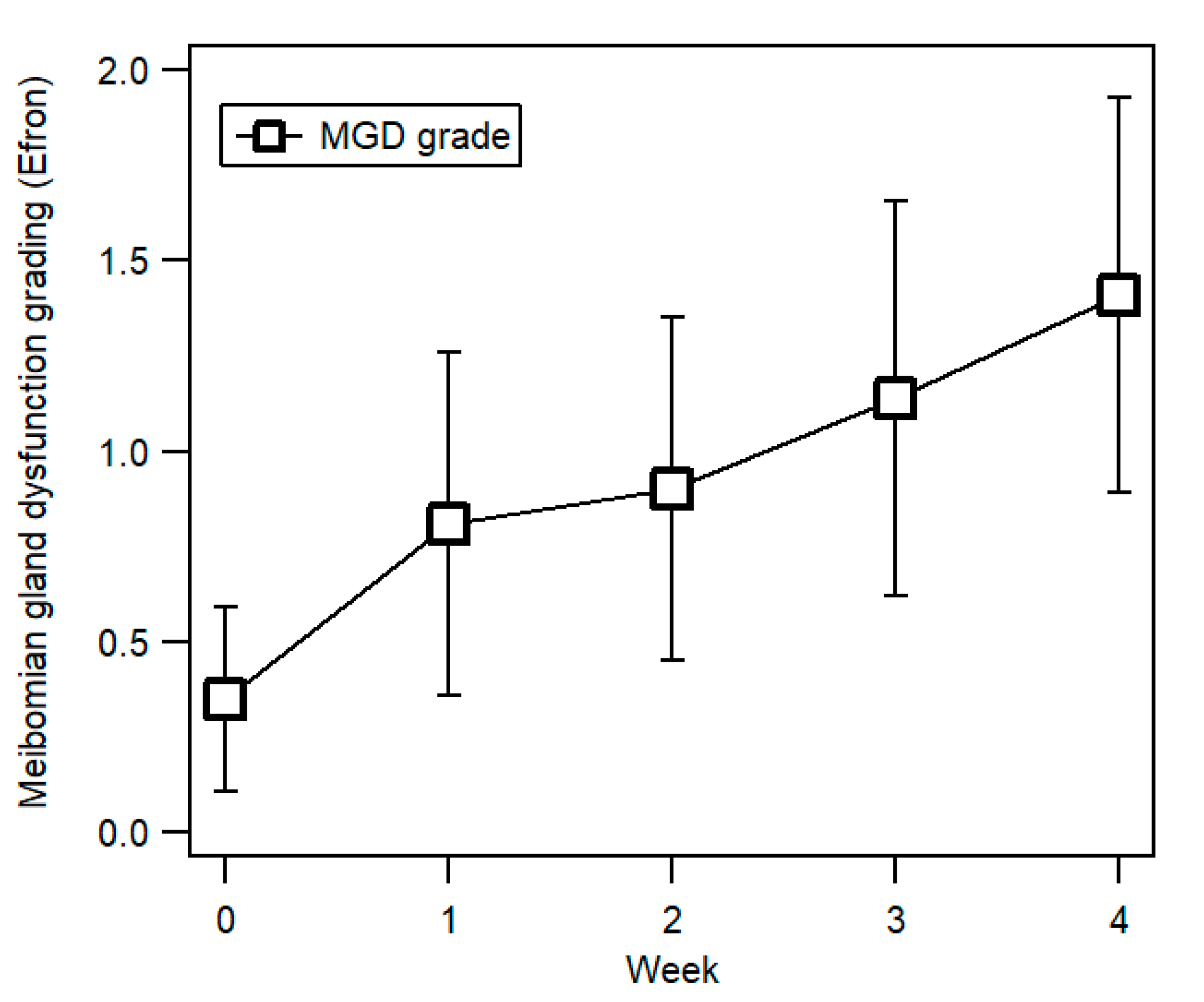
3.2.4. Meibomian Gland Dysfunction
3.3. Tear Break-Up Time (TBUT)
3.4. Intraocular Pressure (IOP)
3.5. Ocular Surface Disease Index (OSDI) Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kiranantawat, K.; Suhk, J.H.; Nguyen, A.H. The Asian eyelid: Relevant anatomy. Semin. Plast. Surg. 2015, 29, 158–164. [Google Scholar] [PubMed]
- Rhee, S.C.; Woo, K.-S.; Kwon, B. Biometric study of eyelid shape and dimensions of different races with references to beauty. Aesthetic Plast. Surg. 2012, 36, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Park, D.H.; Choi, W.S.; Yoon, S.H.; Song, C.H. Anthropometry of Asian eyelids by age. Plast. Reconstr. Surg. 2008, 121, 1405–1413. [Google Scholar] [CrossRef]
- Saonanon, P. Update on Asian eyelid anatomy and clinical relevance. Curr. Opin. Ophthalmol. 2014, 25, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.Q.; Hsu, P.W.; Dinh, T.A. Asian blepharoplasty. Semin. Plast. Surg. 2009, 23, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.Y.; Kadir, K.; Ngeow, W.C.; Othman, S.A. The prevalence of double eyelid and the 3D measurement of orbital soft tissue in malays and chinese. Sci. Rep. 2017, 7, 14819. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.C.; Lee, S.H. Attractive composite faces of different races. Aesthetic Plast. Surg. 2010, 34, 800–801. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Bissell, K. The globalization of beauty: How is ideal beauty influenced by globally published fashion and beauty magazines? J. Intercult. Commun. Res. 2014, 43, 194–214. [Google Scholar] [CrossRef]
- Zhang, M. A Chinese beauty story: How college women in China negotiate beauty, body image, and mass media. Chin. J. Commun. 2012, 5, 437–454. [Google Scholar] [CrossRef]
- Johansson, P. Chinese Women and Consumer Culture: Discourses on Beauty and Identity in Advertising and Women’s Magazines; Stockholms Universitet: Stockholm, Sweden, 1998; pp. 1985–1995. [Google Scholar]
- Watts, J. China’s cosmetic surgery craze. Lancet 2004, 363, 958. [Google Scholar] [CrossRef]
- Zhu, L.; Chen, X. Mechanical analysis of eyelid morphology. Acta Biomater. 2013, 9, 7968–7976. [Google Scholar] [CrossRef] [PubMed]
- Clavin, H.D. Cosmetic Tape, Applicator Therefor and Method. U.S. Patent No: 4,653,483, 31 March 1987. [Google Scholar]
- Ng, A.; Evans, K.; North, R.V.; Jones, L.; Purslow, C. Impact of eye cosmetics on the eye, adnexa, and ocular surface. Eye Contact Lens 2016, 42, 211–220. [Google Scholar] [CrossRef]
- Ng, A.; Evans, K.; North, R.; Purslow, C. Eye cosmetic usage and associated ocular comfort. Ophthalmic Physiol. Opt. 2012, 32, 501–507. [Google Scholar] [CrossRef]
- Wilson, S.E.; Bannan, R.A.; McDonald, M.B.; Kaufman, H.E. Corneal trauma and infection caused by manipulation of the eyelashes after application of mascara. Cornea 1990, 9, 182. [Google Scholar] [CrossRef]
- Uchino, M.; Schaumberg, D.A. Dry eye disease: Impact on quality of life and vision. Curr. Ophthalmol. Rep. 2013, 1, 51–57. [Google Scholar] [CrossRef]
- Tong, L.; Waduthantri, S.; Wong, T.; Saw, S.; Wang, J.; Rosman, M.; Lamoureux, E. Impact of symptomatic dry eye on vision-related daily activities: The Singapore Malay Eye Study. Eye 2010, 24, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Gong, L.; Sun, X.; Chapin, W.J. Anxiety and depression in patients with dry eye syndrome. Curr. Eye Res. 2011, 36, 1–7. [Google Scholar] [CrossRef]
- Hajar-Maidin, M.H.; Mohd-Ali, B.; Ahmad, A.; Mohammed, Z.; Mohamed, J. Associations between dry eye symptoms with tear film stability, volume, and osmolarity in a sample of young adults in Kuala Lumpur. Sudan J. Paediatr. 2018, 10, 32. [Google Scholar]
- Wan, T.; Jin, X.; Lin, L.; Xu, Y.; Zhao, Y. Incomplete blinking may attribute to the development of meibomian gland dysfunction. Curr. Eye Res. 2016, 41, 179–185. [Google Scholar] [CrossRef]
- Norris, M.R.; Bielory, L. Cosmetics and ocular allergy. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Coroneo, M.T.; Rosenberg, M.L.; Cheung, L.M. Ocular effects of cosmetic products and procedures. Ocul Surf. 2006, 4, 94–102. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Okura, M.; Kawashima, M.; Katagiri, M.; Shirasawa, T.; Tsubota, K. New eye cleansing product improves makeup-related ocular problems. J. Ophthalmol. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.J.; Iskander, D.R.; Saunders, A.; Hook, S.; Anthony, E.; Gillon, R. Blinking patterns and corneal staining. Eye Contact Lens 2006, 32, 287–293. [Google Scholar] [CrossRef]
- Kawashima, M.; Tsubota, K. Tear lipid layer deficiency associated with incomplete blinking: A case report. BMC Ophthalmol. 2013, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.D.; Lane, K.J.; Ousler III, G.W.; Angjeli, E.; Smith, L.M.; Abelson, M.B. Blink: Characteristics, controls, and relation to dry eyes. Curr. Eye Res. 2018, 43, 52–66. [Google Scholar] [CrossRef] [PubMed]
- Himebaugh, N.L.; Begley, C.G.; Bradley, A.; Wilkinson, J.A. Blinking and tear break-up during four visual tasks. Optom. Vis. Sci. 2009, 86, E106–E114. [Google Scholar] [CrossRef]
- Ciolino, J.B.; Mills, D.M.; Meyer, D.R. Ocular manifestations of long-term mascara use. Ophthal. Plast. Reconstr. Surg. 2009, 25, 339–341. [Google Scholar] [CrossRef]
- Hunter, M.; Bhola, R.; Yappert, M.C.; Borchman, D.; Gerlach, D. Pilot study of the influence of eyeliner cosmetics on the molecular structure of human meibum. Ophthalmic Res. 2015, 53, 131–135. [Google Scholar] [CrossRef]
- Wang, H.-y.; Seger, K.R.; Yang, S.-n.; Xing, X.-l. The role of ethnicity versus environment in tear film stability: A pilot study. Cont. Lens. Anterior Eye 2019, 42, 553–556. [Google Scholar] [CrossRef]
- Craig, J.P.; Lim, J.; Han, A.; Tien, L.; Xue, A.L.; Wang, M.T. Ethnic differences between the Asian and Caucasian ocular surface: A co-located adult migrant population cohort study. Ocul. Surf. 2019, 17, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.; Yap, M. Age, gender, and tear break-up time. Optom. Vis. Sci. 1993, 70, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.T.; Tien, L.; Han, A.; Lee, J.M.; Kim, D.; Markoulli, M.; Craig, J.P. Impact of blinking on ocular surface and tear film parameters. Ocul. Surf. 2018, 16, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Mohidin, N.; Jaafar, A.B. Effect of smoking on tear stability and corneal surface. J. Curr. Ophthalmol. 2020, 32, 232. [Google Scholar] [CrossRef] [PubMed]
- Mohidin, N.; Zulkipli, N.N. Tear Stability, Corneal Staining and Dry Eye Symptoms in Contact Lens Wearers. J. Sains Kesihatan Malaysia (Malaysian J. Health Sci.) 2019, 17, 35–41. [Google Scholar] [CrossRef]
- Yeh, T.N.; Graham, A.D.; Lin, M.C. Relationships among tear film stability, osmolarity, and dryness symptoms. Optom. Vis. Sci. 2015, 92, e264. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Pflugfelder, S.C. The effects of long-term contact lens wear on corneal thickness, curvature, and surface regularity. Ophthalmology 2000, 107, 105–111. [Google Scholar] [CrossRef]
- Del Águila-Carrasco, A.J.; Domínguez-Vicent, A.; Pérez-Vives, C.; Ferrer-Blasco, T.; Montés-Micó, R. Assessment of modifications in thickness, curvatures, and volume upon the cornea caused by disposable soft contact lens wear. Eur. J. Ophthalmol. 2015, 25, 385–390. [Google Scholar] [CrossRef]
- Radaie-Moghadam, S.; Hashemi, H.; Jafarzadehpur, E.; Yekta, A.A.; Khabazkhoob, M. Corneal biomechanical changes following toric soft contact lens wear. J. Ophthalmic. Vis. Res. 2016, 11, 131. [Google Scholar]
- Çavdarlı, C.; Topçu-Yılmaz, P. Does Long-term Soft Contact Lens Wear Affect Corneal and Anterior Chamber Parameters? Turk. J. Ophthalmol. 2018, 48, 166. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Claoué, C. Transport and interaction of cosmetic product material within the ocular surface: Beauty and the beastly symptoms of toxic tears. Cont. Lens. Anterior Eye. 2012, 35, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, B.; Armstrong, S. Penetrating eye injury caused by eyelash curlers—A cause for concern? Graefes. Arch. Clin. 2010, 248, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Maidin, M.H.H.; Mohd-Ali, B.; Mohammed, Z.; Mohamed, J. Meibomian Gland Dropout and Ocular Surface Appearances of Young Adults in Kuala Lumpur (Kehilangan K elenjar Meibomian dan C iri P ermukaan O kular D ewasa M uda di Kuala Lumpur). Sains. Malays. 2020, 49, 801–808. [Google Scholar] [CrossRef]
- Nichols, K.K. Patient-reported symptoms in dry dye disease. Ocul. Surf. 2006, 4, 137–145. [Google Scholar] [CrossRef]
- Kotliar, K.; Maier, M.; Bauer, S.; Feucht, N.; Lohmann, C.; Lanzl, I. Effect of intravitreal injections and volume changes on intraocular pressure: Clinical results and biomechanical model. Acta Ophthalmol. Scand. 2007, 85, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Ulrich, J.L.; Sanz, A.; Feliu-Soler, A.; Álvarez, M.; Borràs, X. Could white coat ocular hypertension affect to the accuracy of the diagnosis of Glaucoma? Relationships between anxiety and intraocular pressure in a simulated clinical setting. Appl. Psychophysiol. Biofeedback 2018, 43, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Zhou, Y.; Zhang, S.; Cui, C.; Song, X.; Zhu, X.; Fu, Y. Impact of full-incision double-eyelid blepharoplasty on tear film dynamics and dry eye symptoms in young Asian females. Aesthetic Plast. Surg. 2020, 1–8. [Google Scholar] [CrossRef]
- Shao, C.; Fu, Y.; Lu, L.; Chen, J.; Shen, Q.; Zhu, H.; Fan, X. Dynamic changes of tear fluid after cosmetic transcutaneous lower blepharoplasty measured by optical coherence tomography. Am. J. Ophthalmol. 2014, 158, 55–63. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the ocular surface disease index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Perry, J.D. Invited Discussion on: Impact of Full-Incision Double-Eyelid Blepharoplasty on Dry Eye Symptoms in Young Asian Patients. Aesthetic Plast. Surg. 2020, 1–2. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Week 0 | Week 1 | Week 2 | Week 3 | Week 4 | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | Mean ± SD | 95% CI | ||
| Blink rate (bpm) | 24.97 ± 13.38 | 20.1, 29.84 | 21.79 ± 14.26 | 16.6, 26.98 | 24.07 ± 15.46 | 18.44, 29.70 | 26.00 ± 13.67 | 21.02, 30.98 | 24.69 ± 17.69 | 18.25, 31.13 | 0.45 |
| Corneal staining grade | 0.02 ± 0.09 | −0.02, 0.00 | 0.24 ± 0.41 | 0.09, 0.33 | 0.41 ± 0.57 | 0.21, 0.62 | 0.50 ± 0.55 | 0.30, 0.80 | 0.40 ± 0.51 | 0.21, 0.61 | <0.001 |
| Conjunctival staining grade | 0.41 ± 0.50 | 0.23, 0.60 | 0.55 ± 0.49 | 0.37, 0.73 | 0.76 ± 0.69 | 0.51, 1.01 | 0.81 ± 0.52 | 0.62, 1.00 | 0.97 ± 0.52 | 0.78, 1.15 | <0.001 |
| Horizontal corneal curvature (D) | 43.35 ± 1.45 | 42.82, 43.88 | 43.28 ± 1.39 | 42.77, 43.78 | 43.28 ± 1.40 | 42.77, 43.78 | 43.32 ± 1.44 | 42.79, 43.84 | 43.28 ± 1.40 | 42.77, 43.79 | 0.12 |
| Vertical corneal curvature (D) | 44.88 ± 1.52 | 44.33, 45.44 | 44.91 ± 1.49 | 44.36, 45.45 | 44.81 ± 1.37 | 44.31, 45.31 | 44.83 ± 1.55 | 44.27, 45.39 | 44.84 ± 1.49 | 44.30, 45.38 | 0.55 |
| Meibomian gland dysfunction (MGD) grade | 0.35 ± 0.24 | 0.26, 0.43 | 0.81 ± 0.45 | 0.65, 0.97 | 0.90 ± 0.45 | 0.73, 1.06 | 1.14 ± 0.52 | 0.95, 1.33 | 1.41 ± 0.52 | 1.22, 1.60 | <0.001 |
| Tear break-up time (TBUT) (s) | 3.59 ± 1.60 | 3.01, 4.17 | 2.76 ± 1.57 | 2.19, 3.33 | 2.24 ± 1.12 | 1.83, 2.65 | 1.83 + 1.07 | 1.44, 2.22 | 1.66 ± 0.90 | 1.33, 1.98 | <0.001 |
| Intraocular pressure (IOP) (mmHg) | 16.21 ± 3.03 | 15.10, 17.31 | 15.03 + 3.07 | 13.92, 16.15 | 15.21 ± 3.25 | 14.03, 16.39 | 14.55 ± 3.11 | 13.42, 15.68 | 14.45 ± 2.81 | 13.43, 15.47 | <0.01 |
| Ocular Surface Disease Index (OSDI) score | 9.98 ± 8.18 | 7.00, 16.98 | - | - | - | - | - | - | 11.12 ± 10.90 | 7.16, 18.28 | 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yong, P.T.; Arif, N.; Sharanjeet-Kaur, S.; Hairol, M.I. Double Eyelid Tape Wear Affects Anterior Ocular Health among Young Adult Women with Single Eyelids. Int. J. Environ. Res. Public Health 2020, 17, 7701. https://doi.org/10.3390/ijerph17217701
Yong PT, Arif N, Sharanjeet-Kaur S, Hairol MI. Double Eyelid Tape Wear Affects Anterior Ocular Health among Young Adult Women with Single Eyelids. International Journal of Environmental Research and Public Health. 2020; 17(21):7701. https://doi.org/10.3390/ijerph17217701
Chicago/Turabian StyleYong, Pui Theng, Norlaili Arif, Sharanjeet Sharanjeet-Kaur, and Mohd Izzuddin Hairol. 2020. "Double Eyelid Tape Wear Affects Anterior Ocular Health among Young Adult Women with Single Eyelids" International Journal of Environmental Research and Public Health 17, no. 21: 7701. https://doi.org/10.3390/ijerph17217701
APA StyleYong, P. T., Arif, N., Sharanjeet-Kaur, S., & Hairol, M. I. (2020). Double Eyelid Tape Wear Affects Anterior Ocular Health among Young Adult Women with Single Eyelids. International Journal of Environmental Research and Public Health, 17(21), 7701. https://doi.org/10.3390/ijerph17217701