Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life



Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Instruments
2.2.1. Quality of Life—San Martín Scale
2.2.2. Communication Profile Questionnaire
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Participant Communication Profile
3.2. Communication Needs and Quality of Life Index
3.3. Quality of Life Relative to Communicative Profiles
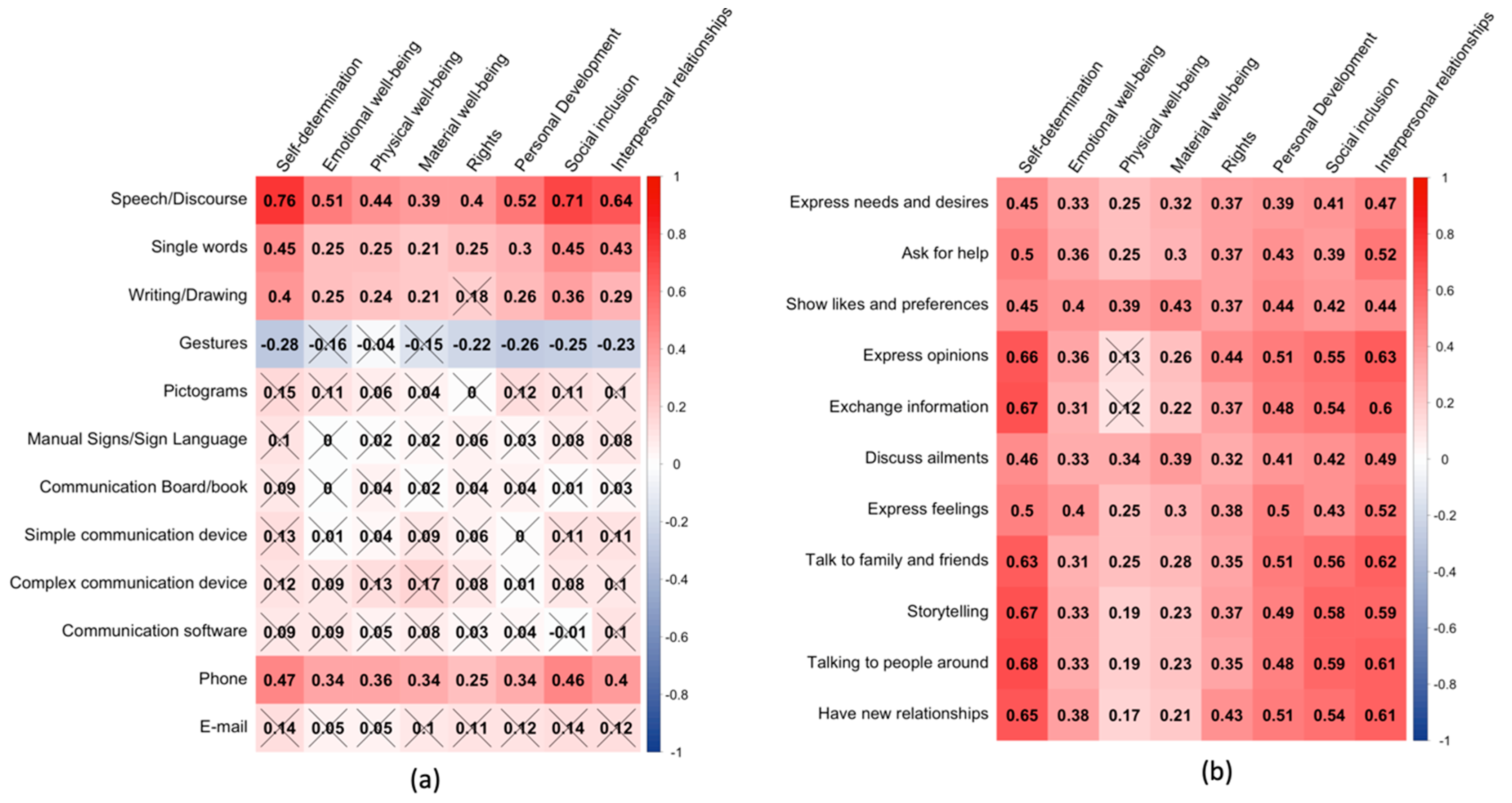
3.4. Personal and Communicative Factors as Predictors of Quality of Life
3.5. Professionals’ Perceptions: ACC Use and Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brady, N.C.; Bruce, S.; Goldman, A.; Erickson, K.; Mineo, B.; Ogletree, B.T.; Paul, D.; Romski, M.A.; Sevcik, R.; Siegel, E.; et al. Communication Services and Supports for Individuals with Severe Disabilities: Guidance for Assessment and Intervention. Am. J. Intellect. Dev. Disabil. 2016, 121, 121–138. [Google Scholar] [CrossRef]
- Markham, C.; van Laar, D.; Gibbard, D.; Dean, T. Children with speech, language and communication needs: Their perceptions of their quality of life. Int. J. Lang. Commun. Disord. 2009, 44, 748–768. [Google Scholar] [CrossRef]
- Saito, Y. Augmentative and alternative communication practice in the pursuit of family quality of life: A review of the literature. Res. Pract. Pers. Sev. Disabil. 2007, 32, 50–65. [Google Scholar] [CrossRef]
- Smith, M.; Manduchi, B.; Burke, É.; Carroll, R.; McCallion, P.; McCarron, M. Communication difficulties in adults with Intellectual Disability: Results from a national cross-sectional study. Res. Dev. Disabil. 2020, 97, 103557. [Google Scholar] [CrossRef]
- Coppens-Hofman, M.C.; Terband, H.; Snik, A.F.M.; Maassen, B.A.M. Speech Characteristics and Intelligibility in Adults with Mild and Moderate Intellectual Disabilities. Folia Phoniatr. Logop. 2016, 68, 175–182. [Google Scholar] [CrossRef]
- Marrus, N.; Hall, L. Intellectual disability and language disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2017, 26, 539–554. [Google Scholar] [CrossRef]
- Tuffrey-Wijne, I.; McEnhill, L. Communication difficulties and intellectual disability in end-of-life care. Int. J. Palliat. Nurs. 2008, 14, 189–194. [Google Scholar] [CrossRef]
- Purcell, M.; Morris, I.; McConkey, R. Staff Perceptions of the Communicative Competence of Adult Persons with Intellectual Disabilities. Br. J. Dev. Disabil. 1999, 45, 16–25. [Google Scholar] [CrossRef]
- Chew, K.L.; Iacono, T.; Tracy, J. Overcoming communication barriers - working with patients with intellectual disabilities. Aust. Fam. Physician 2009, 38, 10–14. [Google Scholar]
- Light, J.; Mcnaughton, D. Designing AAC Research and Intervention to Improve Outcomes for Individuals with Complex Communication Needs. Augment. Altern. Commun. 2015, 31, 85–96. [Google Scholar] [CrossRef]
- Snowling, M.J.; Adams, J.W.; Bishop, D.V.M.; Stothard, S.E. Educational attainments of school leavers with a preschool history of speech-language impairments. Int. J. Lang. Commun. Disord. 2001, 36, 173–183. [Google Scholar] [CrossRef]
- Ball, S.J. Language and Social Advantage: Theory into Practice; Clegg, J., Ginsborg, J., Eds.; John Wiley and Sons, Ltd.: Chichester, UK, 2006. [Google Scholar]
- Gilmore, L.; Cuskelly, M. Vulnerability to loneliness in people with intellectual disability: An explanatory model: Vulnerability to loneliness. J. Policy Pract. Intellect. Disabil. 2014, 11, 192–199. [Google Scholar] [CrossRef]
- Overmars-Marx, T.; Thomése, F.; Verdonschot, M.; Meininger, H. Advancing social inclusion in the neighbourhood for people with an intellectual disability: An exploration of the literature. Disabil. Soc. 2014, 29, 255–274. [Google Scholar] [CrossRef]
- Felce, D. Defining and applying the concept of quality of life. J. Intellect. Disabil. Res. 1997, 41, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.; Hwang, B.; Kim, J.H.; Eisenman, L.T.; Killian, D.J. Quality of life in applied research: A review and analysis of empirical measures. Am. J. Ment. Retard. 1995, 99, 623–641. [Google Scholar]
- McVilly, K.R.; Rawlinson, R.B. Quality of life issues in the development and evaluation of services for people with intellectual disability. J. Intellect. Dev. Disabil. 1998, 23, 199–218. [Google Scholar] [CrossRef]
- McIntyre, D. The difficulties of inclusive pedagogy for initial teacher education and some thoughts on the way forward. Teach. Teach. Educ. Int. J. Res. Stud. 2009, 25, 602–608. [Google Scholar] [CrossRef]
- Rapley, M. Quality of Life Research: A Critical Introduction; SAGE Pubications: London, UK, 2003. [Google Scholar]
- Rusch, F.R.; MIllar, D.M. Emerging transition best practices. In Beyond High School: Transition from School to Work; Rusch, F.R., Chadsey, J.G., Eds.; Wadsworth Publishing Co.: Belmont, CA, USA, 1998. [Google Scholar]
- Taylor, S.J.; Bogdan, R.C. Quality of life and the individual’s perspective. In Quality of Life: Perspectives and Issues; American Association on Mental Retardation: Washington, DC, USA, 1990; pp. 27–40. [Google Scholar]
- Bowling, A. Measuring Health: A Review of Quality of Life Measurement Scales, 2nd ed.; Open University Press: Buckingham, PA, USA, 1997. [Google Scholar]
- Kraemer, B.R.; McIntyre, L.L.; Blacher, J. Quality of life for young adults with mental retardation during transition. Ment. Retard. 2003, 41, 250–262. [Google Scholar] [CrossRef]
- Schalock, R.L.; Keith, K.D. Quality of Life Questionnaire; IDS: Worthington, OH, USA, 1993. [Google Scholar]
- Schalock, R.L.; Lemanowicz, J.A.; Conroy, J.W.; Feinstein, C.S. A multi-variate investigative study of the correlates of quality of life. J. Dev. Disabil. 1994, 3, 59–73. [Google Scholar]
- Biggs, E.E.; Carter, E.W. Quality of Life for Transition-Age Youth with Autism or Intellectual Disability. J. Autism Dev. Disord. 2016, 46, 190–204. [Google Scholar] [CrossRef]
- Davis, E.; Reddihough, D.; Murphy, N.; Epstein, A.; Reid, S.M.; Whitehouse, A.; Williams, K.; Leonard, H.; Downs, J. Exploring quality of life of children with cerebral palsy and intellectual disability: What are the important domains of life? Child. Care Health Dev. 2017, 43, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Neumann, S.; Quinting, J.; Rosenkranz, A.; de Beer, C.; Jonas, K.; Stenneken, P. Quality of life in adults with neurogenic speech-language-communication difficulties: A systematic review of existing measures. J. Commun. Disord. 2019, 79, 24–45. [Google Scholar] [CrossRef] [PubMed]
- Cruice, M.; Worrall, L.; Hickson, L.; Murison, R. Finding a focus for quality of life with aphasia: Social and emotional health, and psychological well-being. Aphasiology 2003, 17, 333–353. [Google Scholar] [CrossRef]
- Hilari, K.; Needle, J.J.; Harrison, K.L. What are the important factors in health-related quality of life for people with aphasia? A systematic review. Arch. Phys. Med. Rehabil. 2012, 93, S86–S95. [Google Scholar] [CrossRef] [PubMed]
- Hilari, K.; Byng, S. Health-related quality of life in people with severe aphasia. Int. J. Lang. Commun. Disord. 2009, 44, 193–205. [Google Scholar] [CrossRef]
- Schertz, M.; Karni-Visel, Y.; Tamir, A.; Genizi, J.; Roth, D. Family quality of life among families with a child who has a severe neurodevelopmental disability: Impact of family and child socio-demographic factors. Res. Dev. Disabil. 2016, 53–54, 95–106. [Google Scholar] [CrossRef]
- Dalton, C.; Sweeney, J. Communication supports in residential services for people with an intellectual disability. Br. J. Learn. Disabil. 2013, 41, 22–30. [Google Scholar] [CrossRef]
- Schalock, R.L.; Verdugo, M.Á. Handbook on Quality of Life for Human Service Practitioners; American Association on Mental Retardation: Washington, DC, USA, 2002. [Google Scholar]
- Van Hecke, N.; Claes, C.; Vanderplasschen, W.; De Maeyer, J.; De Witte, N.; Vandevelde, S. Conceptualisation and Measurement of Quality of Life Based on Schalock and Verdugo’s Model: A Cross-Disciplinary Review of the Literature. Soc. Indic. Res. 2018, 137, 335–351. [Google Scholar] [CrossRef]
- Schalock, R.L.; Verdugo, M.A. El concepto de calidad de vida en los servicios y apoyos para personas con discapacidad intelectual [The concept of quality of life in services and supports for people with intellectual disabilities]. Siglo Cero Rev. Esp. Sobre Discapac. Intelect. 2007, 38, 21–36. [Google Scholar]
- Tamarit Cuadrado, J. La transformación de los servicios hacia la calidad de vida. Una iniciativa de innovación social de FEAPS. Siglo Cero Rev. Esp. Sobre Discapac. Intelect. 2015, 46, 47. [Google Scholar] [CrossRef]
- Navas, P.; Gomez, L.E.; Verdugo, M.A.; Schalock, R.L. Derechos de las personas con discapacidad intelectual: Implicaciones de la Convención de Naciones Unidas [Rights of Persons with Intellectual Disabilities: Implications of the United Nations Convention]. Siglo Cero Rev. Esp. Sobre Discapac. Intelect. 2012, 43, 7–28. [Google Scholar]
- United Nations. Convention on the Rights of Persons with Disabilities. Available online: http://www.ohchr.org/EN/Issues/Disability/Pages/TrainingmaterialCRPDConvention_OptionalProtocol.aspx (accessed on 1 July 2020).
- Verdugo, M.A.; Gómez, L.E.; Arias, B.; Navas, P.; Schalock, R.L. Measuring quality of life in people with intellectual and multiple disabilities: Validation of the San Martín scale. Res. Dev. Disabil. 2014, 35, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Hierro Zorrilla, I.; Verdugo Alonso, M.Á.; Gómez Sánchez, L.E.; Fernández Ezquerra, S.; Cisneros Fernández, P. Evaluación de la calidad de vida en personas con discapacidades significativas: Aplicación de la Escala San Martín en la Fundación Obra San Martín. Rev. Esp. Discapac. 2015, 3, 93–105. [Google Scholar] [CrossRef]
- Vega Córdova, V.; Jerano Rio, C.; Flores Robaina, N.; Cruz Ortiz, M.; Artaza, C. Calidad de vida de adultos con discapacidad intelectual institucionalizados en Chile desde la perspectiva de los proveedores de servicios. Univ. Psychol. Ed. Electrónica 2013, 12, 1–27. [Google Scholar] [CrossRef]
- Fried-Oken, M.; Fox, L.; Rau, M.T.; Tullman, J.; Baker, G.; Hindal, M.; Wile, N.; Lou, J.-S. Purposes of AAC device use for persons with ALS as reported by caregivers. Augment. Altern. Commun. Baltim. Md 1985 2006, 22, 209–221. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Austin, P.C. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun. Stat. Simul. Comput. 2009, 38, 1228–1234. [Google Scholar] [CrossRef]
- Friedrich, S.; Pauly, M. MATS: Inference for potentially singular and heteroscedastic MANOVA. J. Multivar. Anal. 2018, 165, 166–179. [Google Scholar] [CrossRef]
- Ferguson, C.J. An effect size primer: A guide for clinicians and researchers. Prof. Psychol. Res. Pract. 2009, 40, 532–538. [Google Scholar] [CrossRef]
- Zhang, Z. Variable selection with stepwise and best subset approaches. Ann. Transl. Med. 2016, 4, 136. [Google Scholar] [CrossRef]
- Beukelman, D.R.; Mirenda, P.; Ball, L.J. Augmentative and Alternative Communication: Supporting Children and Adults with Complex. Communication Needs; Paul H. Brookes Baltimore: Baltimore, MD, USA, 2012. [Google Scholar]
- Brown, F.; Gothelf, C.R.; Guess, D.; Lehr, D.H. Self-Determination for Individuals with the Most Severe Disabilities: Moving beyond Chimera. J. Assoc. Pers. Sev. Handicaps 1998, 23, 17–26. [Google Scholar] [CrossRef]
- Light, J. “Communication is the essence of human life”: Reflections on communicative competence. Augment. Altern. Commun. 1997, 13, 61–70. [Google Scholar] [CrossRef]
- Nieuwenhuijse, A.M.; Willems, D.L.; van Goudoever, J.B.; Echteld, M.A.; Olsman, E. Quality of life of persons with profound intellectual and multiple disabilities: A narrative literature review of concepts, assessment methods and assessors. J. Intellect. Dev. Disabil. 2019, 44, 261–271. [Google Scholar] [CrossRef]
- National Joint Committee for the Communication Needs of Persons with Severe Disabilities. Guidelines for Meeting the Communication Needs of Persons with Severe Disabilities. Available online: https://www.asha.org/policy/GL1992-00201/ (accessed on 20 June 2020).


{kind=link}
| Variable Description | Value |
|---|---|
| Mean (SD) age | 42.3 (13.7) |
| Age range | 19–71 |
| Mean (SD) % disability | 79.8 (9.7) |
| % disability range | 37–99 |
| Conditions associated with ID: | |
| Physical disability | 116 |
| Sensorial disability | 70 |
| Behavioral problems | 69 |
| Cerebral palsy | 60 |
| Dependency assessment: | |
| Moderate level | 32 |
| High level | 112 |
| Unknown | 5 |
| Intensity of support: | |
| Extensive support | 133 |
| Generalized support | 84 |
| Unknown | 64 |
| Communication Modes | CSN | |||
|---|---|---|---|---|
| No (n = 98) | Yes (n = 182) | χ2 p-Value | SMD | |
| Speech/Discourse | 93.8 | 9.3 | ** | 3.2 |
| Single words | 82.7 | 41.2 | ** | 0.9 |
| Writing/Drawing | 37.8 | 7.7 | ** | 0.8 |
| Gestures | 53.1 | 75.8 | ** | 0.5 |
| Pictograms | 19.4 | 19.2 | n.s. | 0.0 |
| Manual Signs/Sign Language | 6.1 | 8.8 | n.s. | 0.1 |
| Communication Board/book | 3.1 | 3.9 | n.s. | 0.0 |
| Simple communication device | 6.1 | 5.0 | n.s. | 0.1 |
| Complex communication device | 4.1 | 1.7 | n.s. | 0.1 |
| Communication software on a device | 1.0 | 2.8 | n.s. | 0.1 |
| Phone | 61.2 | 14.9 | ** | 1.1 |
| 4.1 | 0.6 | n.s. | 0.2 | |
| Communicative Purposes | CSN | |||
|---|---|---|---|---|
| No (n = 98) | Yes (n = 182) | χ2 p-Value | SMD | |
| Express needs and desires | 99.0 | 80.8 | <0.001 | 0.6 |
| Ask for help | 99.0 | 74.7 | <0.001 | 0.8 |
| Show likes and preferences | 99.0 | 80.8 | <0.001 | 0.6 |
| Express opinions | 93.9 | 46.7 | <0.001 | 1.2 |
| Exchange information | 92.9 | 39.6 | <0.001 | 1.4 |
| Discuss ailments | 98.0 | 70.3 | <0.001 | 0.8 |
| Express feelings | 98.0 | 66.5 | <0.001 | 0.9 |
| Talk to family and friends | 96.9 | 52.7 | <0.001 | 1.2 |
| Storytelling | 90.8 | 25.8 | <0.001 | 1.8 |
| Talk to people around them | 93.9 | 36.8 | <0.001 | 1.5 |
| Have new relationships | 92.9 | 43.3 | <0.001 | 1.3 |
| Quality of Life Dimension | All Sample | CSN | CSN versus Non-CSN | ||
|---|---|---|---|---|---|
| No (n = 98) | Yes (n = 182) | Welsch’s t p-Value | Cohen’s d [95% CI] | ||
| Self-determination | 9.4 (3.8) | 12.9 (2.1) | 7.6 (3.2) | <0.001 | 1.8 [1.5, 2.2] |
| Emotional wellbeing | 9.2 (2.78) | 10.9 (2.2) | 8.3 (2.7) | <0.001 | 1.0 [0.7, 1.3] |
| Physical wellbeing | 8.5 (3.4) | 10.1 (2.8) | 7.6 (3.4) | <0.001 | 0.8 [0.5, 1.0] |
| Material wellbeing | 7.6 (3.2) | 8.94 (3.0) | 6.9 (3.1) | <0.001 | 0.7 [0.4, 0.9] |
| Rights | 8.7 (3.3) | 10.1 (2.7) | 7.9 (3.4) | <0.001 | 0.7 [0.5, 1.0] |
| Personal Development | 8.9 (2.9) | 10.6 (2.1) | 8.0 (2.8) | <0.001 | 1.0 [0.7, 1.3] |
| Social inclusion | 9.1 (3.2) | 11.7 (2.0) | 7.7 (2.8) | <0.001 | 1.5 [1.3, 1.9] |
| Interpersonal relationships | 8.2 (3.3) | 10.7 (2.2) | 6.9 (3.1) | <0.001 | 1.4 [1.0, 1.7] |
| Global QLI | 92.1 (16.1) | 104.29 (11) | 85.48 (15.57) | <0.001 | 1.4 [1.1, 1.7] |
| Communication Support Needs | ||||
|---|---|---|---|---|
| No | Yes | |||
| Predictors | R2 | r | R2 | r |
| Personal characteristics | ||||
| Age | 0.10 ** | 0.31 * | 0.05 ** | 0.22 * |
| Sex | 0.001 | −0.005 | 0.01 | −0.08 |
| Level of disability | 0.04 | −0.06 | 0.12 *** | −0.32 *** |
| Number of additional conditions | 0.04 | −0.11 | 0.08 *** | −0.25 *** |
| Additional conditions | ||||
| Physical disability | 0.01 | −0.07 | 0.11 *** | −0.33 *** |
| Sensory—hearing | 0.02 | −0.15 | 0.01 | −0.09 |
| Sensory—visual | 0.004 | 0.09 | 0.04 * | −0.18 * |
| Cerebral palsy | 0.07 | −0.25 * | 0.04 * | −0.18 * |
| Epilepsy | 0.02 | −0.14 | 0.03 * | −0.18 * |
| Mental health | 0.02 | −0.20 * | 0.02 | −0.13 |
| Down syndrome | 0.05 | −0.21 * | 0.001 | −0.01 |
| Serious health problems | 0.05 | −0.20 | 0.01 | −0.08 |
| Behavior problems | 0.11* | −0.33 *** | 0.01 | −0.07 |
| Modes of communication | ||||
| Speech/discourse | 0.33 | 0.24 * | 0.22 *** | 0.43 *** |
| Single words | 0.08 ** | −0.16 | 0.10 *** | 0.32 *** |
| Writing/drawing | 0.05 | 0.08 | 0.05 *** | 0.22 ** |
| Gestures | 0.14 *** | −0.32 ** | 0.03 | −0.15 * |
| Pictograms | 0.04 | −0.05 | 0.06 *** | 0.26 ** |
| Manual signs/sign language | 0.000 | 0.03 | 0.02 * | 0.14 |
| Communication board/book | 0.06 | −0.20 * | 0.02 * | 0.15 * |
| Simple communication device | 0.01 | −0.08 | 0.02 | 0.13 |
| Complex communication device | 0.000 | 0.03 | 0.03 *** | 0.15 * |
| Communication software on a device | 0.03 *** | −0.14 | 0.04 *** | 0.18 * |
| Phone | 0.01 | 0.14 | 0.10 *** | 0.28 *** |
| 0.003 | 0.05 | 0.01 *** | 0.09 | |
| Purposes of communication | ||||
| Express needs and desires | 0.23 *** | 0.17 | 0.19 *** | 0.40 *** |
| Ask for help | 0.23 *** | 0.17 | 0.18 *** | 0.39 *** |
| Show likes and preferences | 0.23 *** | 0.17 | 0.27 *** | 0.46 *** |
| Express opinions | 0.000 | 0.14 | 0.15 *** | 0.39 *** |
| Exchange information | 0.01 | 0.15 | 0.11 *** | 0.34 *** |
| Discuss ailments | 0.01 *** | 0.18 | 0.25 *** | 0.42 *** |
| Express feelings | --- | 0.21 * | 0.16 *** | 0.39 *** |
| Talk to family and friends | 0.02 | 0.13 | 0.17 *** | 0.42 *** |
| Storytelling | 0.01 | 0.11 | 0.09 *** | 0.30 *** |
| Talk to people around | 0.01 | 0.13 | 0.12 *** | 0.36 *** |
| Have new relationships | 0.02 | 0.20* | 0.14 *** | 0.37 *** |
| Predictor | Simple Model (BIC) | Complex Model (AIC) |
|---|---|---|
| Age | YES | |
| Level of disability | YES | YES |
| Physical disability | YES | |
| Speech/discourse | YES | YES |
| Pictograms | YES | |
| Communication software | YES | YES |
| Express needs and desires | YES | |
| Show likes and preferences | YES | YES |
| Storytelling | YES | |
| Have new relationships (yes) | YES | YES |
| B (95 % CI) | Bias | SE (Standard Error) | p | |
|---|---|---|---|---|
| (Intercept) | 82.2 (69.0,96.6) | 0.1 | 7.0 | 0.001 *** |
| Speech/discourse (yes) | 17.7 (14.5,20.8) | −0.0 | 1.6 | 0.001 *** |
| Communication software (yes) | 16.7 (−14.9,40.6) | −1.4 | 13.5 | 0.111 |
| Show likes and preferences (yes) | 15.5 (10.8,20.0) | 0.1 | 2.4 | 0.002 *** |
| Have new relationships (yes) | 4.3 (−0.02,7.7) | −0.1 | 1.9 | 0.026 * |
| Level of disability | −0.2 (−0.3,−0.0) | −0.0 | 0.1 | 0.009 ** |
| B (95 % CI) | Bias | SE | p | |
|---|---|---|---|---|
| (Intercept) | 90.6 (71.3,114.8) | 1.4 | 11.2 | 0.001 *** |
| Speech/discourse (yes) | 18.8 (14.1,23.6) | −0.1 | 2.3 | 0.001 *** |
| Communication software (yes) | 19.7 (−1.7,34.7) | −0.2 | 8.4 | 0.034 * |
| Show likes and preferences (yes) | 15.0 (9.8,19.3) | −0.2 | 2.6 | 0.005 ** |
| Have new relationships (yes) | 3.8 (−0.5,7.8) | −0.2 | 2.1 | 0.039 * |
| Level of disability | −0.3 (−0.5,−0.1) | −0.0 | 0.1 | 0.005 ** |
| Supports Provided | CSN | |||
|---|---|---|---|---|
| No (n = 98) | Yes (n = 182) | χ2 p-Value | SMD | |
| Have the disability support services ever worked with the user using AAC (Augmentative/Alternative Communication)? | 8.4 | 21.8 | <0.01 | 0.38 |
| Are the disability support services adapted from the point of view of cognitive accessibility for the user? | 68.0 | 51.1 | <0.01 | 0.35 |
| Is the training received to provide communication support (e.g., AAC) adequate, taking into account the person’s profile? | 35.4 | 14.1 | <0.001 | 0.51 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, J.C.; Díez, E.; Wojcik, D.Z.; Santamaría, M. Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 7370. https://doi.org/10.3390/ijerph17207370
García JC, Díez E, Wojcik DZ, Santamaría M. Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life. International Journal of Environmental Research and Public Health. 2020; 17(20):7370. https://doi.org/10.3390/ijerph17207370
Chicago/Turabian StyleGarcía, Juan Carlos, Emiliano Díez, Dominika Z. Wojcik, and Mónica Santamaría. 2020. "Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life" International Journal of Environmental Research and Public Health 17, no. 20: 7370. https://doi.org/10.3390/ijerph17207370
APA StyleGarcía, J. C., Díez, E., Wojcik, D. Z., & Santamaría, M. (2020). Communication Support Needs in Adults with Intellectual Disabilities and Its Relation to Quality of Life. International Journal of Environmental Research and Public Health, 17(20), 7370. https://doi.org/10.3390/ijerph17207370