Telemedicine in Oral and Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
- A1 patients in oncological follow-up after surgical treatment performed before the COVID-19 pandemic;
- A2 patients suffering from chronic lesions such as precancerous lesions, MRONJ;
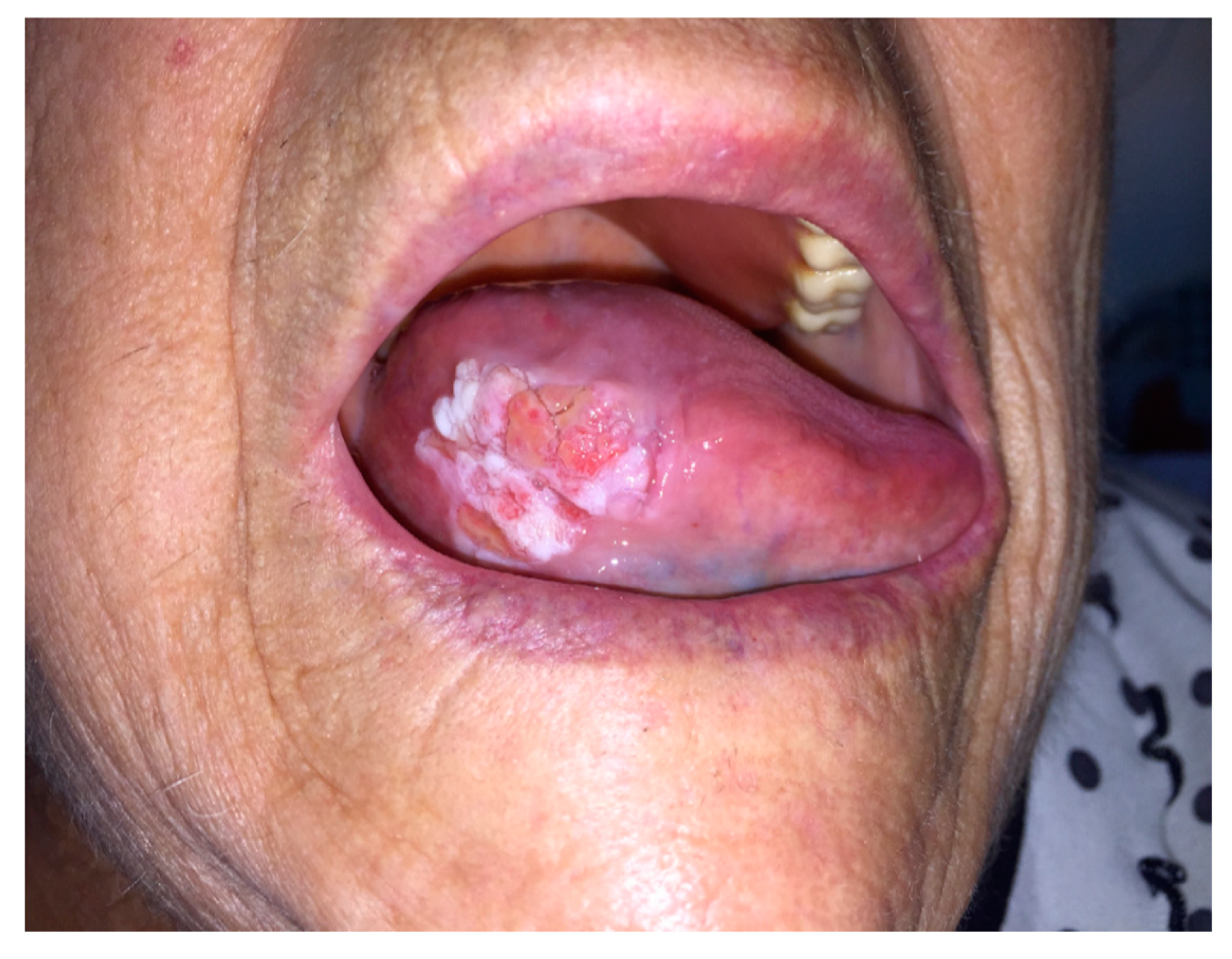
- B1 patients with suspected oncological pathology
- B2 patients with suspected urgent disease (MRONJ, odontogenic abscesses, TMJ dislocation)
2.2. A Group
2.3. B Group
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics and Pathology of the Study Population.
3.2. Results A Group
3.3. Results B Group
3.4. Analysis of Satisfaction Questionnaires
- (1)
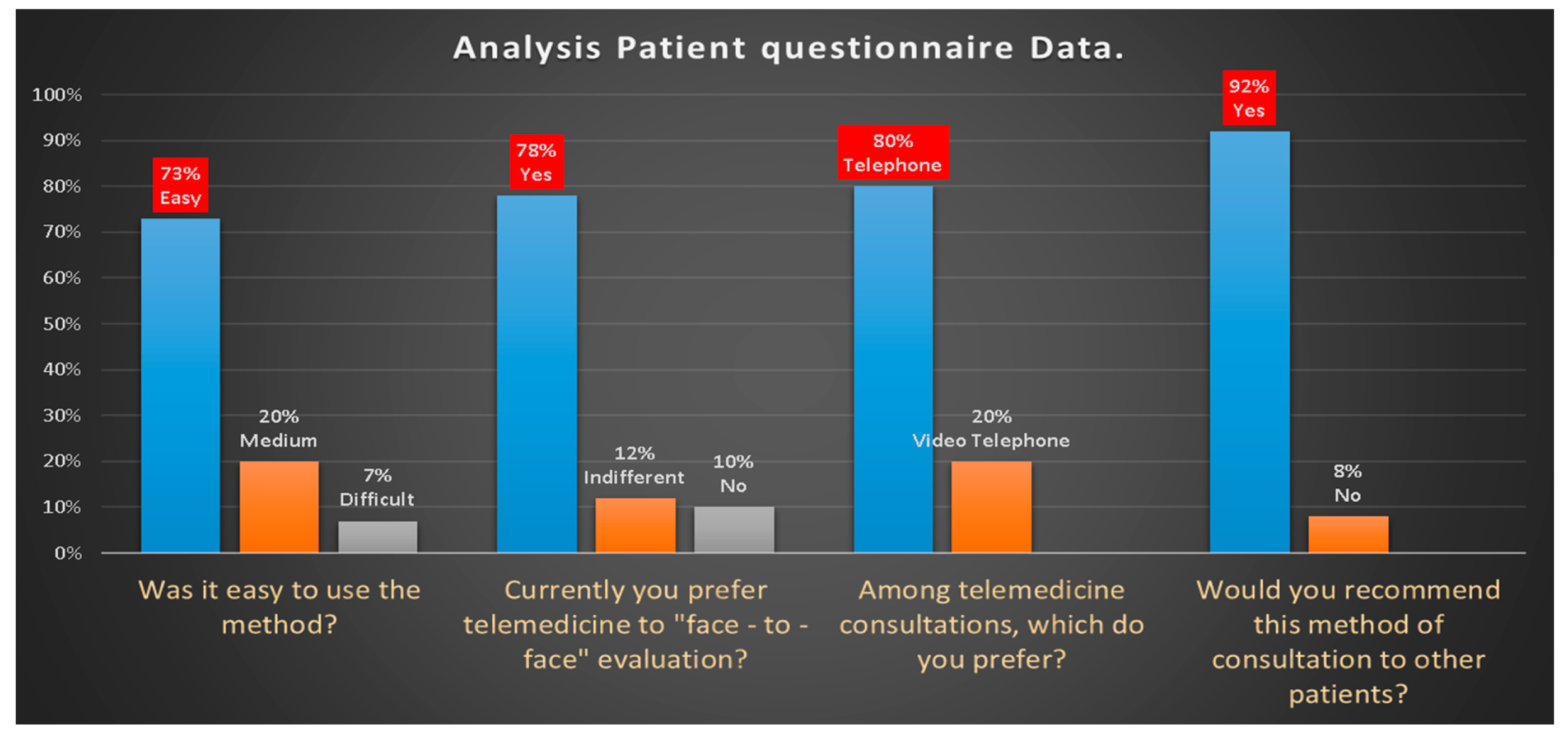
- 73% of patients found easy to participate in the consultation, 20% medium and 7% difficult.
- (2)
- 78% currently preferred telemedicine, 12% indifferent and 10% face-to-face consultation
- (3)
- 80% of patients chose video-telephone consultation rather than telephone consultation because they were able to see the doctor’s face and because it was easier to describe the symptoms.
- (4)
- 92% of patients would recommend video consultation to others.
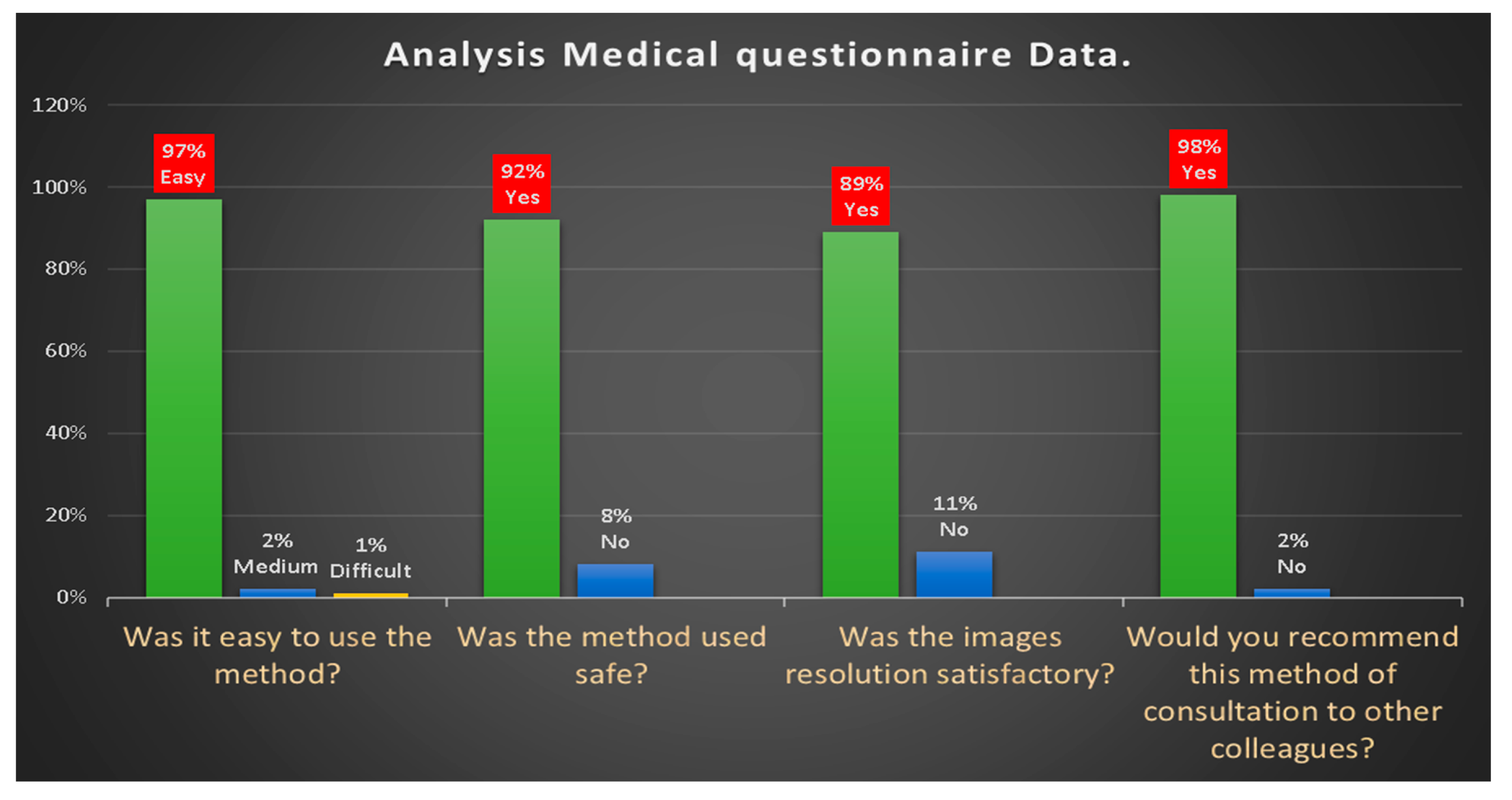
- 97% of doctors found it easy to participate in the consultation, 2% medium and 1% difficult.
- the method proved to be 92% safe
- the resolution of the video image to evaluate facial asymmetries, the presence of swellings, bone exposures, skin and mucous membrane changes due to the presence of suspected lesion was 89% satisfactory
- 98% of doctors would recommend video consultation to other colleagues.
4. Discussion
- evaluate the surgical sites (possible presence of visible masses and/or local recurrences, evident lymphadenopathies, etc.),
- discuss with the patient about the progress of oncological pathology,
- view the cancer surveillance imaging,
- allow the patient to ask questions and clear up doubts,
- involve other specialists in the video-conference, because, as is known, the treatment of head-neck oncological pathology requires a multi-disciplinary approach (maxillofacial surgeon, radiotherapist, oncologist, nutritionist, etc.).
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Elkaddoum, R.; Haddad, F.G.; Eid, R.; Kourie, H.R. Telemedicine for cancer patients during COVID-19 pandemic: Between threats and opportunities. Future Oncol. 2020, 16, 1225–1227. [Google Scholar] [CrossRef] [PubMed]
- Moazzami, B.; Razavi-Khorasani, N.; Moghadam, A.D.; Farokhi, E.; Rezaei, N. COVID-19 and telemedicine: Immediate action required for maintaining healthcare providers well-being. J. Clin. Virol. 2020, 126, 104345. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.Y.; Knight, S.; Guetter, C.R.; Davis, C.H.; Moller, M.; Slama, E.; Crandall, M. Telemedicine and telementoring in the surgical specialties: A narrative review. Am. J. Surg. 2019, 218, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Thomas, P.B.M.; Sim, D.A.; Parker, R.T.; Daniel, C.; Uddin, J.M. Oculoplastic video-based telemedicine consultations: Covid-19 and beyond. Eye 2020, 34, 1193–1195. [Google Scholar] [CrossRef] [PubMed]
- Contreras, C.M.; Metzger, G.A.; Beane, J.D.; Dedhia, P.H.; Ejaz, A.; Pawlik, T.M. Telemedicine: Patient-Provider Clinical Engagement During the COVID-19 Pandemic and Beyond. J. Gastrointest. Surg. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Matusitz, J.; Breen, G.-M. Telemedicine: Its Effects on Health Communication. Health Commun. 2007, 21, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Jena, A.B.; Busch, A.B.; Souza, J.; Uscher-Pines, L.; Landon, B.E. Utilization of Telemedicine Among Rural Medicare Beneficiaries. JAMA 2016, 315, 2015–2016. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Escobar, M.A.; Cardoza-Avendaño, L.; López-Gutiérrez, R.M.; Cruz-Hernández, C. A Double Chaotic Layer Encryption Algorithm for Clinical Signals in Telemedicine. J. Med. Syst. 2017, 41. [Google Scholar] [CrossRef] [PubMed]
- Gunter, R.L.; Chouinard, S.; Fernandes-Taylor, S.; Wiseman, J.T.; Clarkson, S.; Bennett, K.; Greenberg, C.C.; Kent, K.C. Current Use of Telemedicine for Post-Discharge Surgical Care: A Systematic Review. J. Am. Coll. Surg. 2016, 222, 915–927. [Google Scholar] [CrossRef] [PubMed]
- Onuma, A.E.; Kelly, E.P.; Chakedis, J.; Paredes, A.Z.; Tsilimigras, D.I.; Wiemann, B.; Johnson, M.; Merath, K.; Akgul, O.; Cloyd, J.; et al. Patient preferences on the use of technology in cancer surveillance after curative surgery: A cross-sectional analysis. Surgery 2019, 165, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Barca, I.; Cordaro, R.; Kallaverja, E.; Ferragina, F.; Cristofaro, M.G.; Ida, B.; Raffaella, C.; Elvis, K.; Francesco, F.; Giulia, C. Management in oral and maxillofacial surgery during the COVID-19 pandemic: Our experience. Br. J. Oral Maxillofac. Surg. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Nardo, B.; Cannistrà, M.; Diaco, V.; Naso, A.; Novello, M.; Zullo, A.; Ruggiero, M.; Grande, R.; Sacco, R. Optimizing Patient Surgical Management Using WhatsApp Application in the Italian Healthcare System. Telemed. e-Health 2016, 22, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Alabdullah, J.H.; Daniel, S.J. A Systematic Review on the Validity of Teledentistry. Telemed. e-Health 2018, 24, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Barca, I.; Cristofaro, M. Surgical approach to parotid pleomorphic adenoma: A 15-year retrospective cohort study. Br. J. Oral Maxillofac. Surg. 2020, 16, 266. [Google Scholar] [CrossRef]
- Perrotta, I.; Cristofaro, M.G.; Amantea, M.; Russo, E.; De Fazio, S.; Zuccalà, V.; Conforti, F.; Amorosi, A.; Donato, G.; Tripepi, S.; et al. Jaw Osteonecrosis in Patients Treated with Bisphosphonates: An Ultrastructural Study. Ultrastruct. Pathol. 2010, 34, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Cristofaro, M.; Giudice, A.; Amentea, M.; Giudice, M. Diagnostic and therapeutic approach to sialoblastoma of submandibular gland: A case report. M. J. Oral Maxillofac. Surg. 2008, 66, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Barca, I.; Colangeli, W.; Cristofaro, M.G.; Giudice, A.; Giofrè, E.; Varano, A.; Giudice, A. Effects of cold therapy in the treatment of mandibular angle fractures: Hilotherm system vs. ice bag. Ann. Ital. Chir. 2016, 87, 411–416. [Google Scholar]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 Pandemic, Lessons for the Future. Telemed. e-Health 2020, 26, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, C.; Barca, I.; Petrocelli, M.; Orabona, G.D.; A Vaira, L.; Colangeli, W.; Cristofaro, M.G.; Giudice, A.; Giudice, A.; Cassandro, F.M.; et al. The Influence of Socioeconomic Factors on the Epidemiology of Maxillofacial Fractures in Southern Italy. J. Craniofacial Surg. 2018, 29, 2119–2123. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Do you have fever or have you experienced fever within the past 14 days? | YES or NO |
| 2. Have you experienced a recent onset of respiratory problems, such as a cough or difficulty in breathing or diarrhea, ageusia, anosmia within the past 14 days? | YES or NO |
| 3. Have you, within the past 14 days, travelled to risk areas or visited a neighborhood with documented 2019-nCoV transmission? | YES or NO |
| 4. Have you come into contact with a patient with confirmed 2019-nCoV infection within the past 14 days? | YES or NO |
| 5. Have you recently participated in any gathering, meetings, or had close contact with many unacquainted people? | YES or NO |
| Patient Questionnaire | |
| (1) Was the method easy to use? | ▯ Easy ▯ Medium ▯ Difficult |
| (2) Currently you prefer telemedicine to “face-to-face” evaluation? | ▯ Yes ▯ Indifferent ▯ No |
| (3) Among telemedicine consultations, which do you prefer? | ▯ Telephone consultation ▯ Video—Telephone consultation |
| (4) Would you recommend this method of consultation to other patients? | ▯ Yes ▯ No |
| Medical Questionnaire | |
| (1) Was the method easy to use? | ▯ Easy ▯ Medium ▯ Difficult |
| (2) Was the method used safe? | ▯ Yes ▯ No |
| (3) Was the image resolution satisfactory? | ▯ Yes ▯ No |
| (4) Would you recommend this method of consultation to other colleagues? | ▯ Yes ▯ No |
| Sex | Mean Age | Residence |
|---|---|---|
| Male | 68.35 | Province of Catanzaro 25 |
| Other provinces 29 | ||
| Female | 66.23 | Province of Catanzaro 17 |
| Other provinces 19 |
| Group A | |||
| Pathology | Telemedicine | Type | Outpatient Treatment/Service |
| SubGroup A1 Neoplasm Follow-up | 54 contacts | Head & neck Carcinoma: 54 | Clinical control: 7 |
| Advanced dressing: 3 | |||
| Biopsy: 5 | |||
| SubGroup A2 Other Control/Follow-Up | 9 contacts | Pre-cancerous: 6 | |
| MRONJ: 3 | |||
| Group B | |||
| Pathology | Telemedicine | Type | Outpatient Treatment/Service |
| SubGroup B1 Neoplasm 1st visit | 12 contacts | Skin Carcinoma: 3 | Skin Biopsy: 2 |
| Mucosa Oral Carcinoma: 8 | Oral Biopsy: 4 | ||
| Submandibular gland Carcinoma: 1 | |||
| SubGroup B2 Other 1st visit | 15 contacts | MRONJ: 7 | MRONJ: 3 |
| TMJ Dislocation: 2 | TMJ Dislocation: 2 | ||
| Odontogenic abscess: 3 | Odontogenic abscess: 1 | ||
| Sialoadenitis: 3 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barca, I.; Novembre, D.; Giofrè, E.; Caruso, D.; Cordaro, R.; Kallaverja, E.; Ferragina, F.; Cristofaro, M.G. Telemedicine in Oral and Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7365. https://doi.org/10.3390/ijerph17207365
Barca I, Novembre D, Giofrè E, Caruso D, Cordaro R, Kallaverja E, Ferragina F, Cristofaro MG. Telemedicine in Oral and Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(20):7365. https://doi.org/10.3390/ijerph17207365
Chicago/Turabian StyleBarca, Ida, Daniela Novembre, Elio Giofrè, Davide Caruso, Raffaella Cordaro, Elvis Kallaverja, Francesco Ferragina, and Maria Giulia Cristofaro. 2020. "Telemedicine in Oral and Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic" International Journal of Environmental Research and Public Health 17, no. 20: 7365. https://doi.org/10.3390/ijerph17207365
APA StyleBarca, I., Novembre, D., Giofrè, E., Caruso, D., Cordaro, R., Kallaverja, E., Ferragina, F., & Cristofaro, M. G. (2020). Telemedicine in Oral and Maxillo-Facial Surgery: An Effective Alternative in Post COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 17(20), 7365. https://doi.org/10.3390/ijerph17207365