An fMRI Study on Self-Perception of Patients after Aesthetic Implant-Prosthetic Rehabilitation

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects (Protocol Viscon-01)
2.2. Neuropsychological Battery
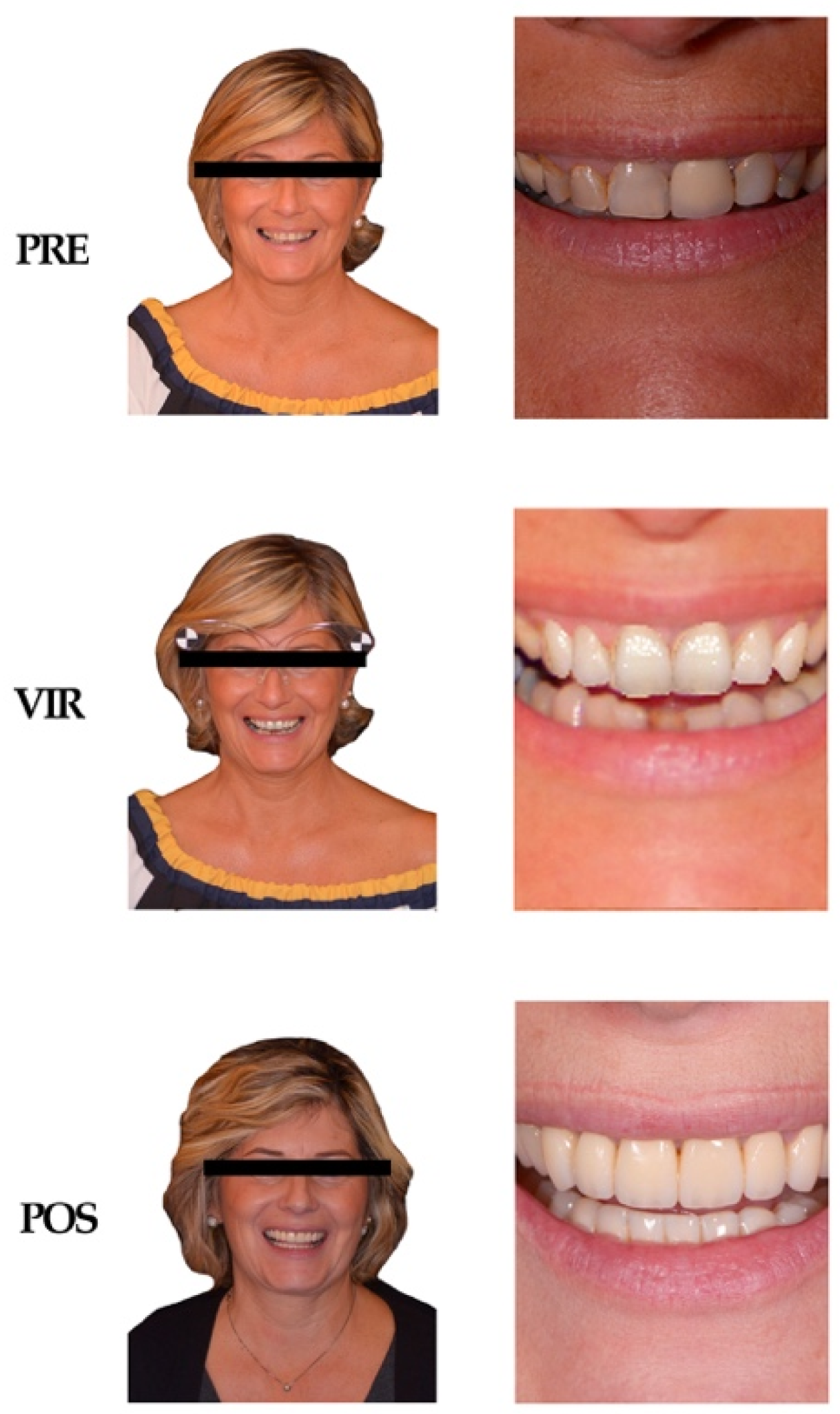
2.3. Stimuli
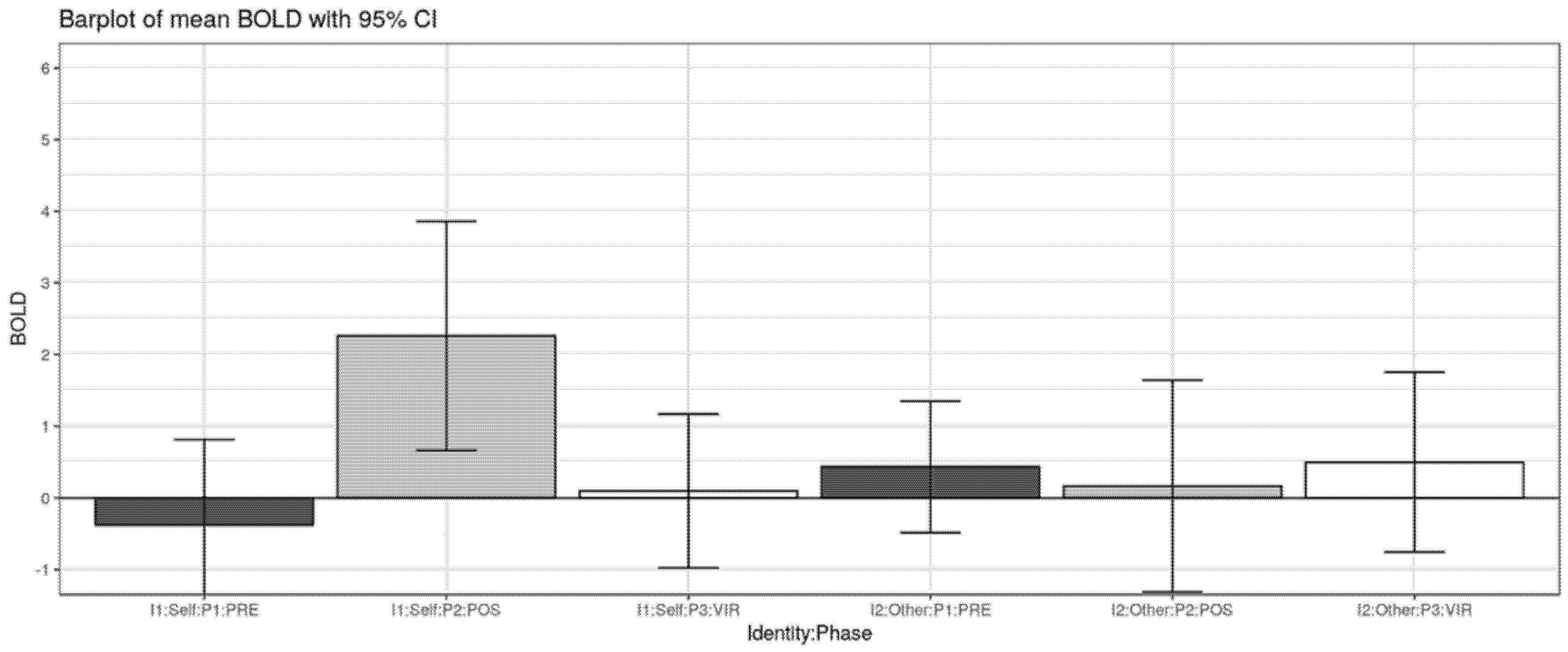
2.4. Factors Taken into Consideration
- -
- IDENTITY FACTOR: with the two levels SELF and OTHER.
- -
- PHASE FACTOR: with levels PRE, VIR, and POST.
2.5. Experimental Tasks
2.6. fMRI Data Acquisition
2.7. fMRI Data Analysis
- c1-1.
- Main effect of Identity (SELF vs. OTHER). Contrast weights for [SELF–PRE, SELF–VIR, SELF–POST, OTHER–PRE, OTHER–VIR, OTHER–POST]: [+1 +1 +1 −1 −1 −1].
- c1-2.
- Simple effect of Phase PRE vs. VIR. Contrast weights: [+1 −1 0 +1 −1 0].
- c1-3.
- Simple effect of Phase PRE vs. POST. Contrast weights: [+1 0 −1 +1 0 −1].
- c1-4.
- Simple effect of Phase PRE vs. VIR for SELF (SELF–PRE vs. SELF–VIR). Contrast weights: [+1 −1 0 0 0 0].
- c1-5.
- Simple effect of Phase PRE vs. VIR for OTHER (OTHER–PRE vs. OTHER–VIR). Contrast weights: [0 0 0 +1 −1 0].
- c1-6.
- Simple effect of Phase PRE vs. POST for SELF (SELF–PRE vs. SELF–POST). Contrast weights: [+1 0 −1 0 0 0].
- c1-7.
- Simple effect of Phase PRE vs. POST for OTHER (OTHER–PRE vs. OTHER–POST). Contrast weights: [0 0 0 +1 0 −1].
- c2-1.
- Main effect of Identity (SELF vs. OTHER): one-sample t-test over c1-1 contrasts.
- c2-2.
- Main effect of Phase (PRE vs. VIR vs. POST): two-sample t-test over c1-2 and c1-3 contrasts.
- c2-3.
- Identity by Phase interaction (SELF/OTHER vs. PRE/VIR): paired t-test over c1-4 and c1-5 contrasts.
- c2-4.
- Identity by Phase interaction (SELF/OTHER vs. PRE/POST: paired t-test over c1-6 and c1-7 contrasts.
3. Results
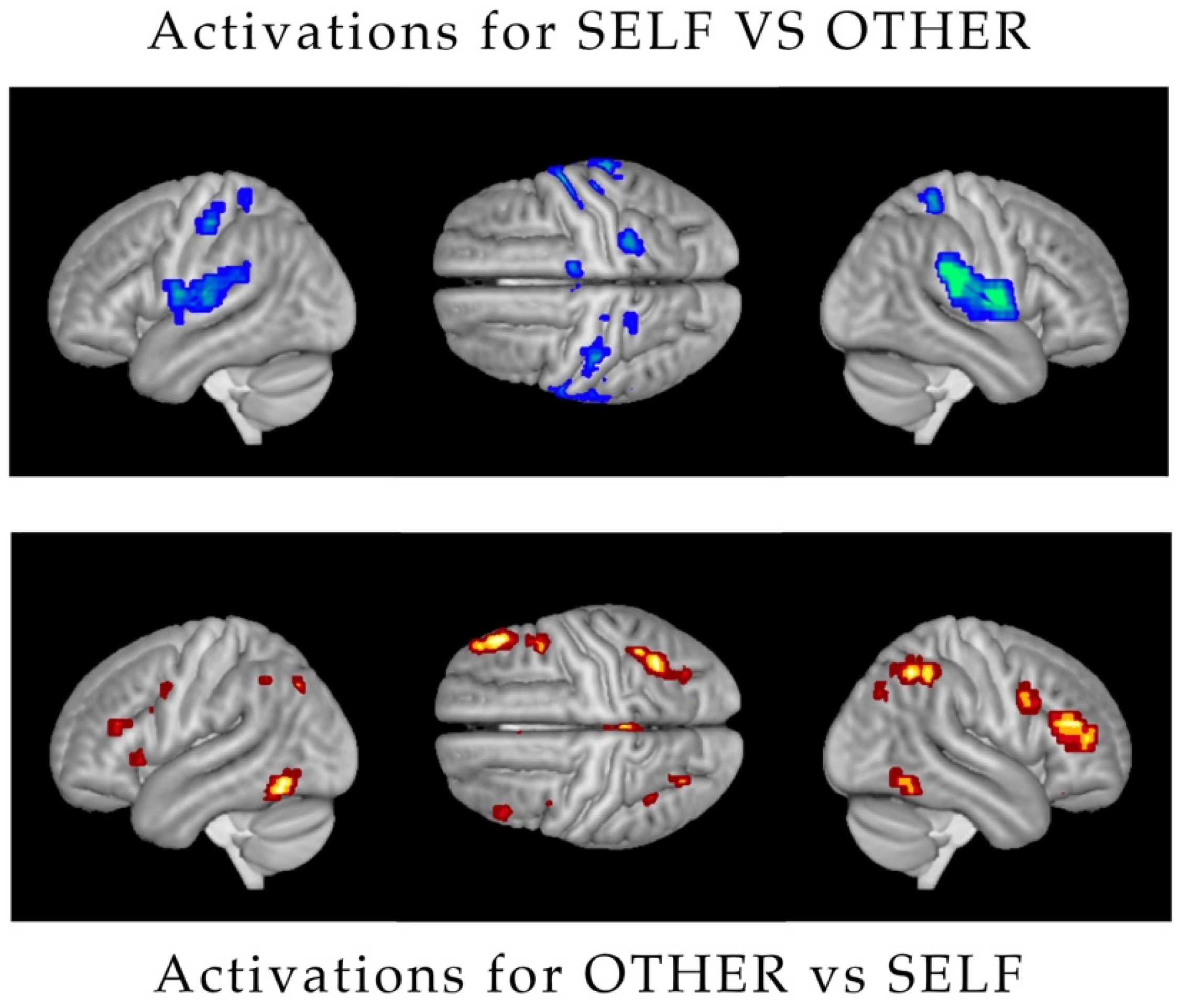
3.1. Main Effect of Identity
3.2. Main Effect of Phase
3.3. Identity by Phase Interaction (Self/Other vs. PRE/VIR)
3.4. Identity by Phase Interaction (Self/Other vs. Pre/Post)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethics Approval and Consent to Participate
Availability of Data and Materials
References
- Fueki, K.; Baba, K. Shortened dental arch and prosthetic effect on oral health-related quality of life: A systematic review and meta-analysis. J. Oral Rehabil. 2017, 44, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Liebermann, A.; Frei, S.; Pinheiro Dias Engler, M.L.; Zuhr, O.; Prandtner, O.; Edelhoff, D.; Saedi Pour, R. Multidisciplinary full-mouth rehabilitation with soft tissue regeneration in the esthetic zone. J. Esthet. Restor. Dent. 2018, 20, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Smile Lynx-3D Lynx. Available online: http://www.3d-lynx.com/ (accessed on 1 January 2018).
- Magne, P.; Hanna, J.; Magne, M. The case for moderate “guided prep” indirect porcelain veneers in the anterior dentition. The pendulum of porcelain veneer preparations: From almost no-prep to over prep to no prep. Eur. J. Esthet. Dent. 2013, 8, 376–388. [Google Scholar] [PubMed]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional vs. Digital Impressions for full arch anti screw-retained Maxillary Rehabilitations. A randomized clinical trial. Int. J. Environ Res. Public Health 2019, 16, 829. [Google Scholar] [CrossRef] [PubMed]
- Coachman, C.; Paravina, R.D. Digitally Enanched Esthetic Dentistry—From Treatment Planning to Quality Control. J. Esthet. Restor. Dent. 2016, 28 (Suppl. 1), S3–S4. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.S.; Smith, D.V.; Delgado, M.R. Using fMRI to study reward processing in humans: Past, present, and future. J. Neurophysiol. 2016, 115, 1664–1678. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Tottenham, N.; Tanaka, J.W.; Leon, A.C.; McCarry, T.; Nurse, M.; Hare, T.A.; Marcus, D.J.; Westerlund, A.; Casey, B.; Nelson, C. The NimStim set of facial expressions: Judgments from untrained research participants. Psychiatry Res. 2009, 168, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Presentation 20.0. Neurobehavioral System. Available online: http://www.neurobs.com/ (accessed on 24 March 2018).
- Statistical Parametric Mapping Wellcome Center for Human Neuroimaging. Available online: https://www.fil.ion.ucl.ac.uk/spm/ (accessed on 2 April 2018).
- Morita, T.; Saito, D.N.; Ban, M.; Shimada, K.; Okamoto, Y.; Kosaka, H.; Okazawa, H.; Asada, M.; Naito, E. Self-face recognition shares brain regions active during proprioceptive illusion in the right inferior fronto-parietal superior longitudinal fasciculus III network. Neuroscience 2017, 348, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.D.; Hitch, G. Working Memory. Psychol. Learn. Motiv. 1974, 8, 47–89. [Google Scholar]
- Friston, K.J.; Penny, W.; Phillips, C.; Kiebel, S.; Hinton, G.; Ashburner, J. Classical and Bayesian Inference in Neuroimaging: Theory. Neuroimage 2002, 16, 465–483. [Google Scholar] [CrossRef]
- Morita, T.; Itakura, S.; Saito, D.N.; Nakashita, S.; Harada, T.; Kochiyama, T.; Sadato, N. The Role of the Right Prefrontal Cortex in Self-evaluation of the Face: A Functional Magnetic Resonance Imaging Study. J. Cogn. Neurosci. 2007, 20, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Penny, W.D.; Friston, K.J.; Ashburner, J.T.; Kiebel, S.J.; Nichols, T.E. Statistical Parametric Mapping: The Analysis of Functional Brain Images, 1st ed.; Academic Press: Cambridge, MA, USA, 2006. [Google Scholar]
- Platek, S.M.; Wathne, K.; Tierney, N.G.; Thomson, J.W. Neural correlates of self-face recognition: An effect-location meta-analysis. Brain Res. 2008, 1232, 173–184. [Google Scholar] [CrossRef]
- Bernstein, M.; Yovel, G. Two neural pathways of face processing: A critical evaluation of current models. Neurosci. Biobehav. Rev. 2015, 55, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Martín-Loeches, M.; Hernández-Tamames, J.A.; Martín, A.; Urrutia, M. Beauty and ugliness in the bodies and faces of others: An fMRI study of person esthetic judgement. Neuroscience 2014, 277, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Al Saleh, S.; Abu-Raisi, S.; Almajed, N.; Bukhary, F. Esthetic self-perception of smiles among a group of dental students. Int. J. Esthet. Dent. 2018, 13, 220–230. [Google Scholar] [PubMed]
- Bortolon, C.; Capdevielle, D.; Altman, R.; Macgregor, A.; Attal, J.; Raffard, S. Mirror self-face perception in idividuals with schizophrenia. Feeling of strangeness associated with one’s own image. Psychiatry Res. 2017, 253, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Càrdena-Bahena, Á.; Velazquez-Olmedo, L.B.; Falcón-Flores, J.A.; García-Zámano, I.E.; Montes-Salmerón, R.E.; Reza-Bravo, G.G.; Sánchez-García, S. Self-perception of oral health in older adults from Mexico City. Rev. Med. Inst. Mex. Seguro Soc. 2018, 56 (Suppl. 1), S54–S63. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Brain Region | Voxels | p-Value | Z | MNI Coordinates (mm) 10 |
|---|---|---|---|---|
| R Posterior-Medial Frontal (SMA) | 1 | 0.09 | 4.5 | 10 0 76 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattoni, F.; Tetè, G.; Uccioli, R.; Manazza, F.; Gastaldi, G.; Perani, D. An fMRI Study on Self-Perception of Patients after Aesthetic Implant-Prosthetic Rehabilitation. Int. J. Environ. Res. Public Health 2020, 17, 588. https://doi.org/10.3390/ijerph17020588
Cattoni F, Tetè G, Uccioli R, Manazza F, Gastaldi G, Perani D. An fMRI Study on Self-Perception of Patients after Aesthetic Implant-Prosthetic Rehabilitation. International Journal of Environmental Research and Public Health. 2020; 17(2):588. https://doi.org/10.3390/ijerph17020588
Chicago/Turabian StyleCattoni, Francesca, Giulia Tetè, Riccardo Uccioli, Fabio Manazza, Giorgio Gastaldi, and Daniela Perani. 2020. "An fMRI Study on Self-Perception of Patients after Aesthetic Implant-Prosthetic Rehabilitation" International Journal of Environmental Research and Public Health 17, no. 2: 588. https://doi.org/10.3390/ijerph17020588
APA StyleCattoni, F., Tetè, G., Uccioli, R., Manazza, F., Gastaldi, G., & Perani, D. (2020). An fMRI Study on Self-Perception of Patients after Aesthetic Implant-Prosthetic Rehabilitation. International Journal of Environmental Research and Public Health, 17(2), 588. https://doi.org/10.3390/ijerph17020588