The Prospects of Secondary Moderate Mitral Regurgitation after Aortic Valve Replacement —Meta-Analysis


 ,
,
Abstract
1. Introduction
2. Methods
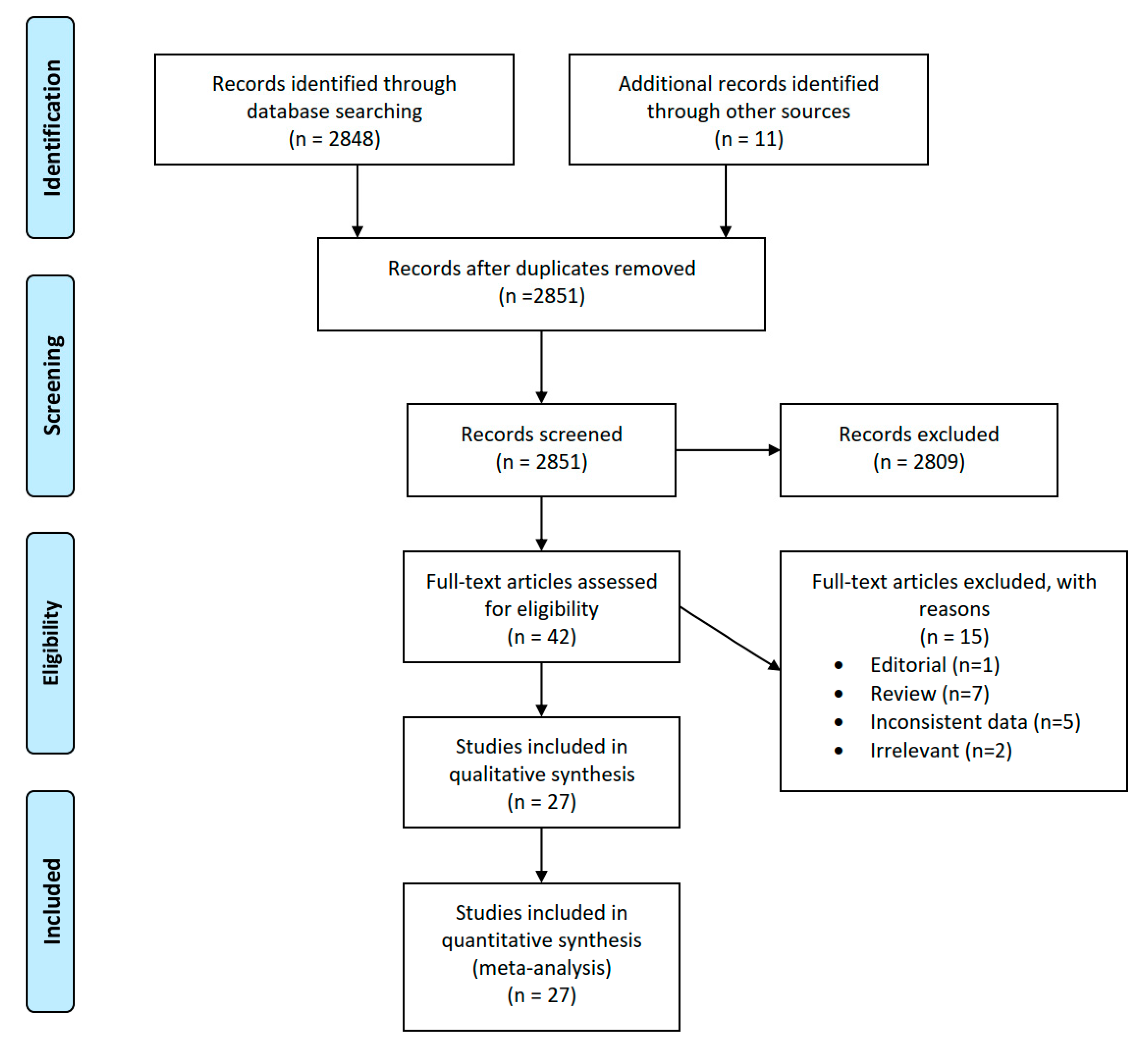
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
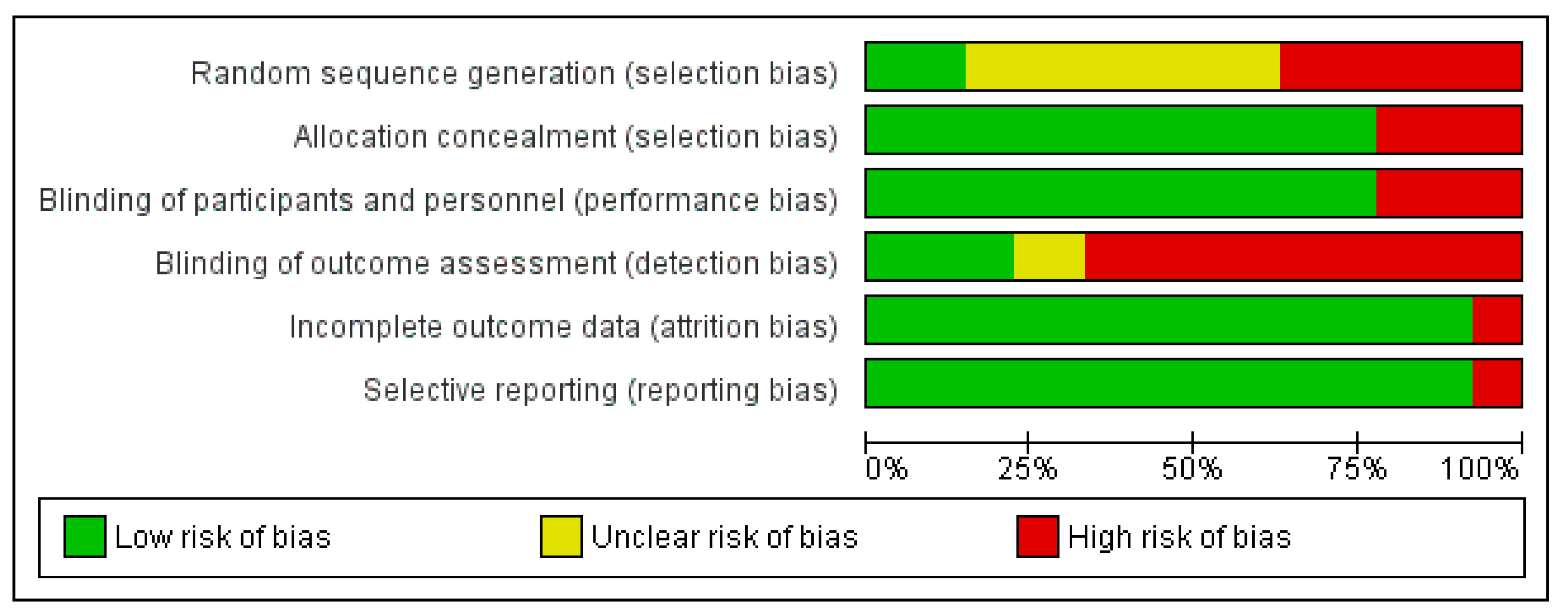
2.4. Risk of Bias
2.5. Data Analysis
3. Results
3.1. Eligible Studies
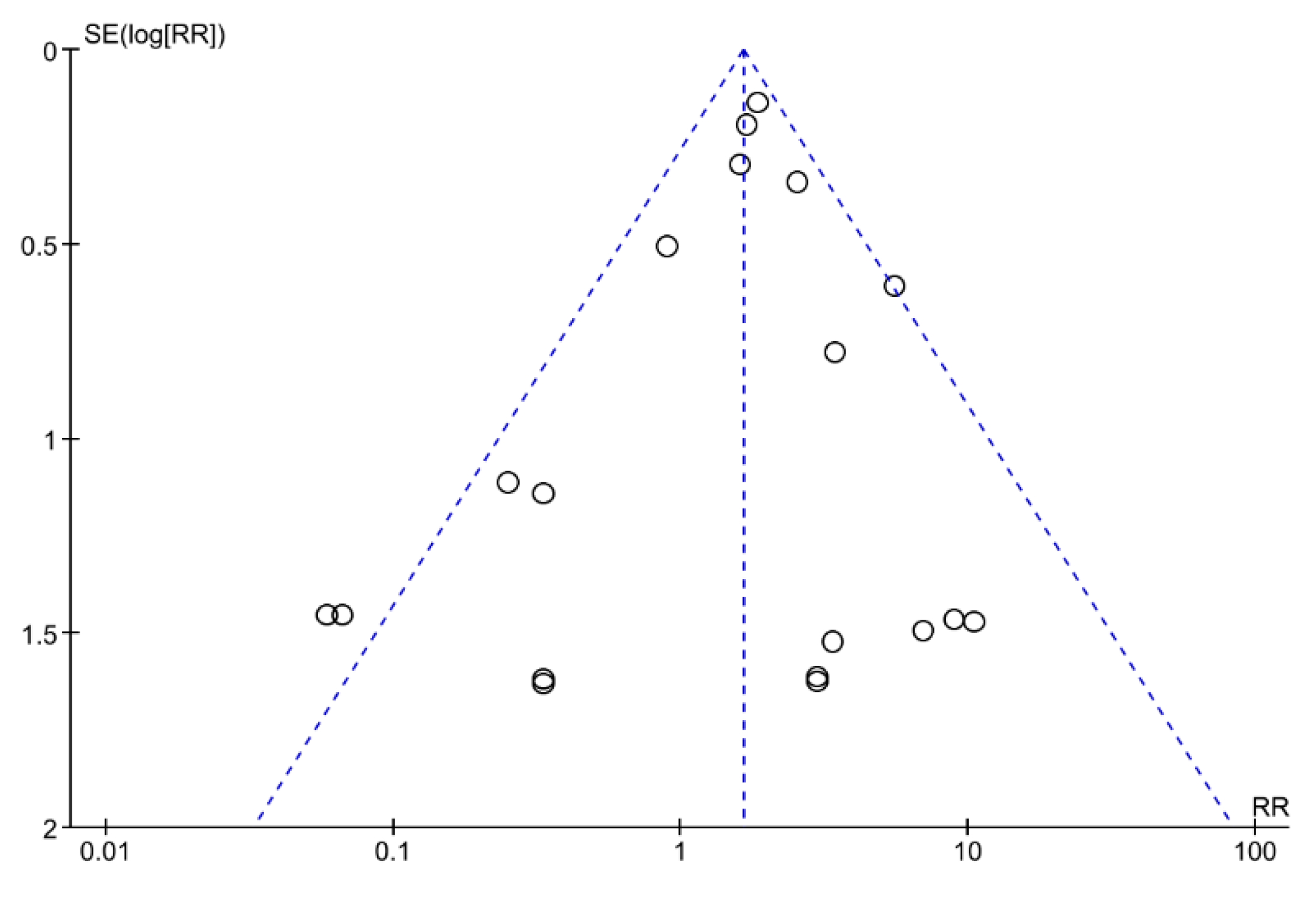
3.2. Risk of Bias
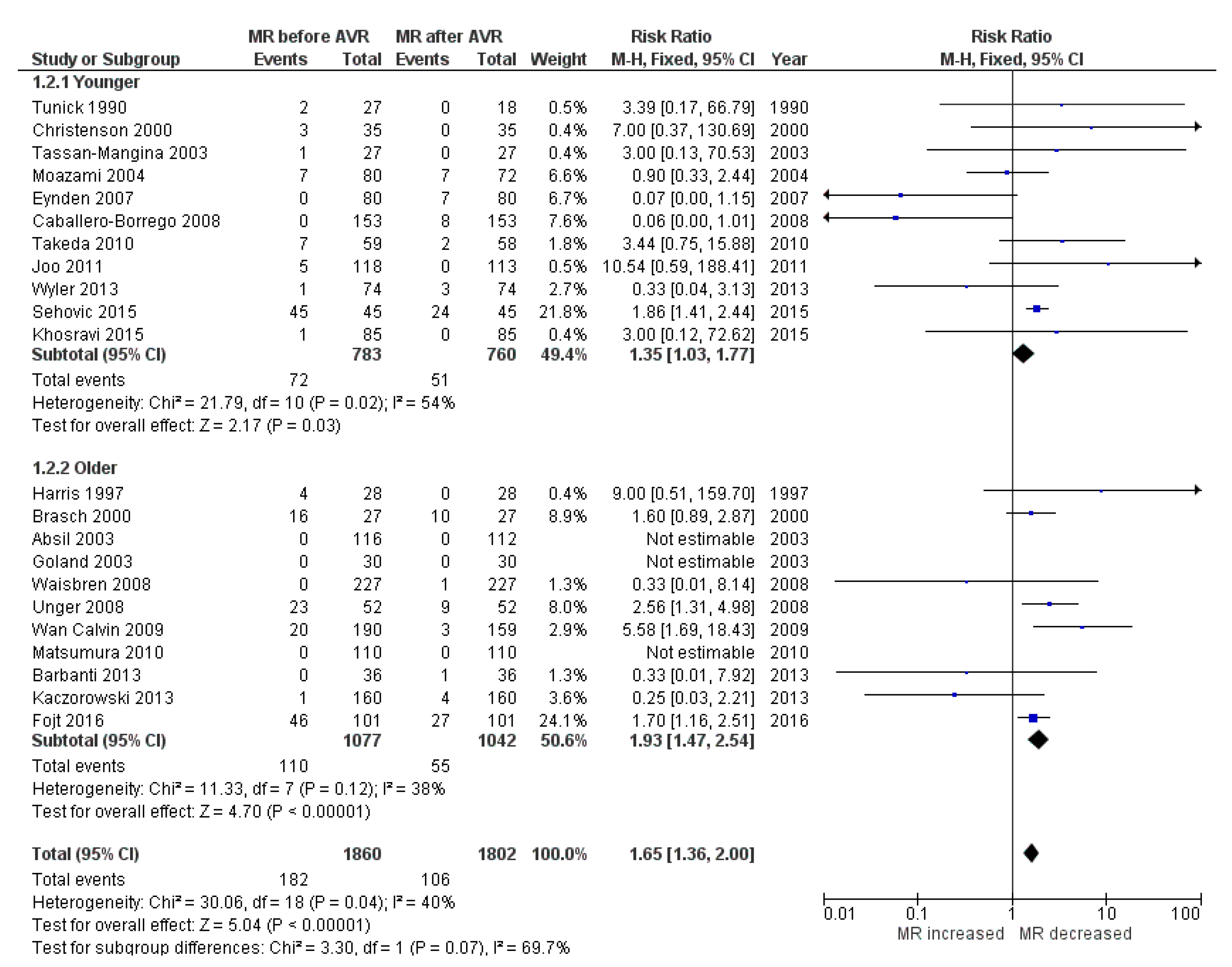
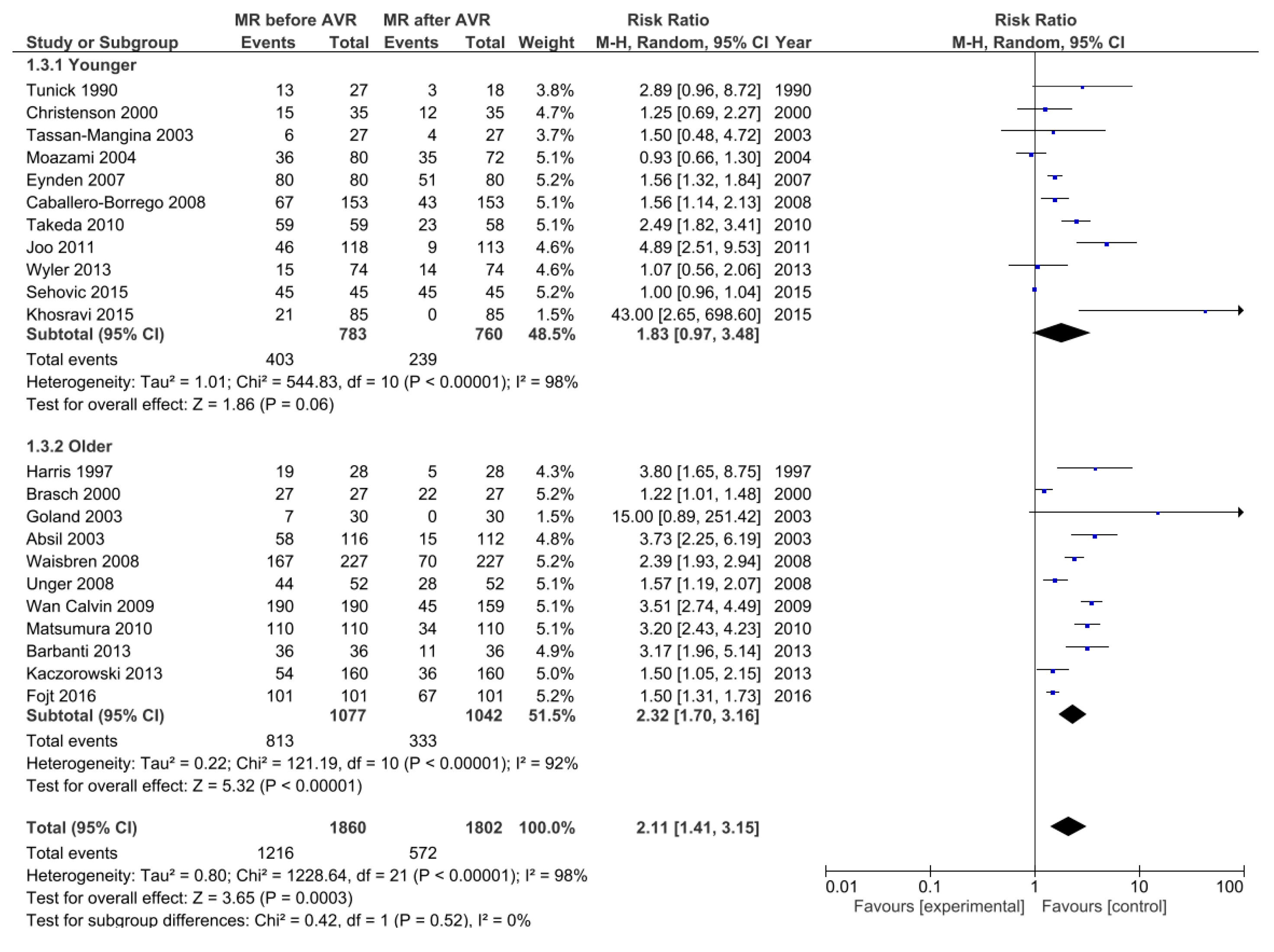
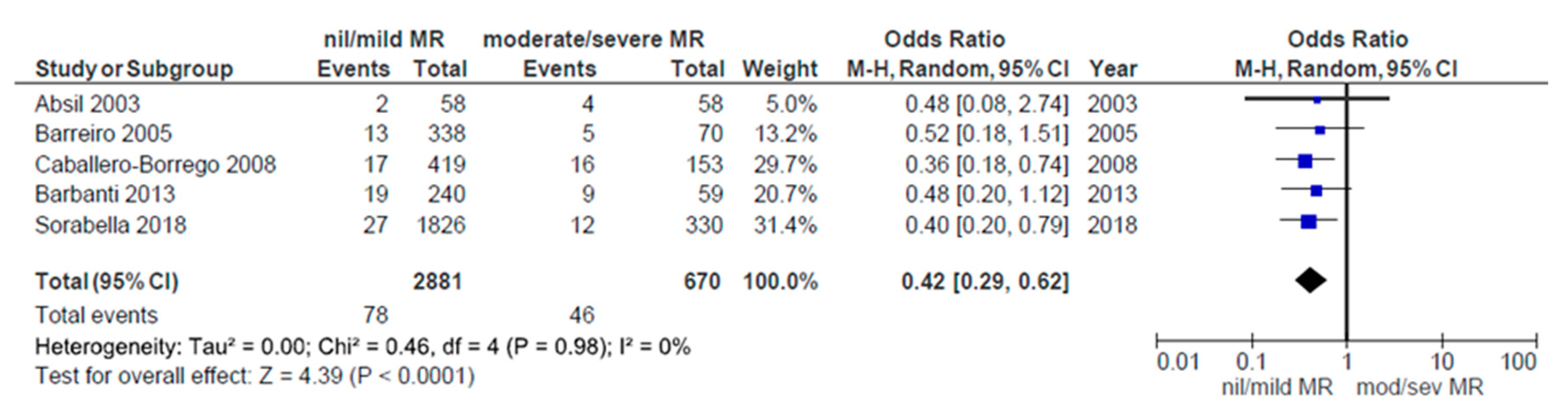
3.3. Change in MR after Aortic Valve Replacement
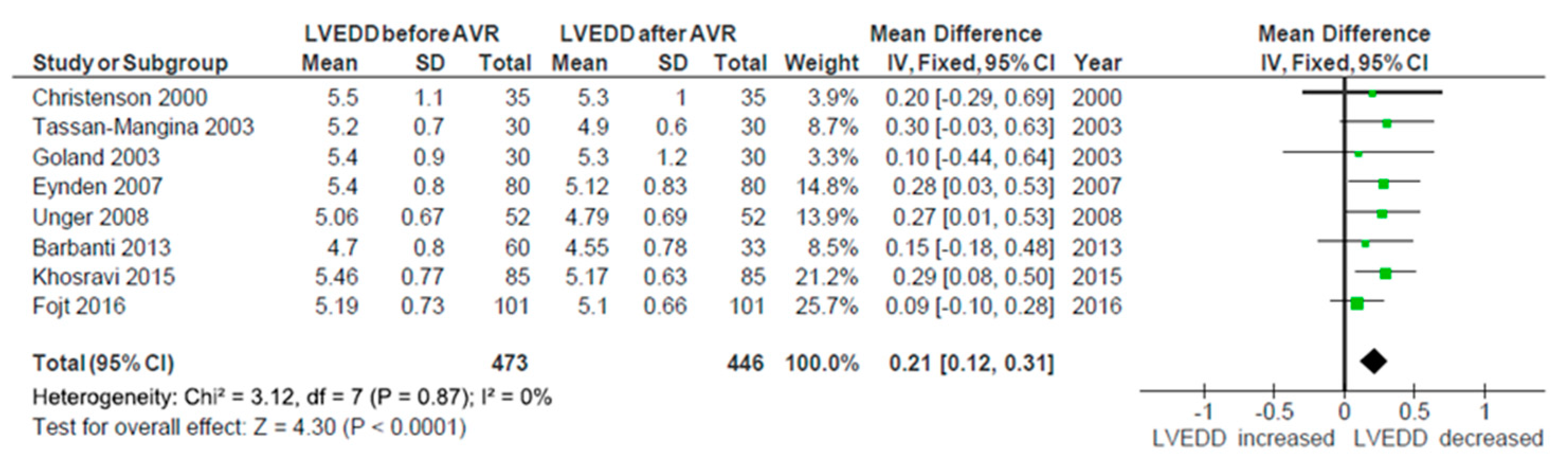
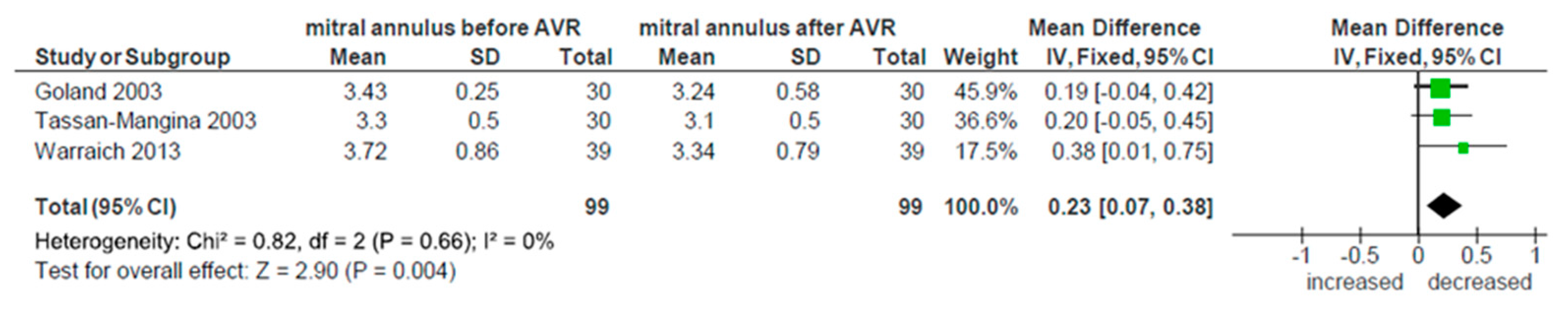
3.4. Reverse Myocardial Remodeling
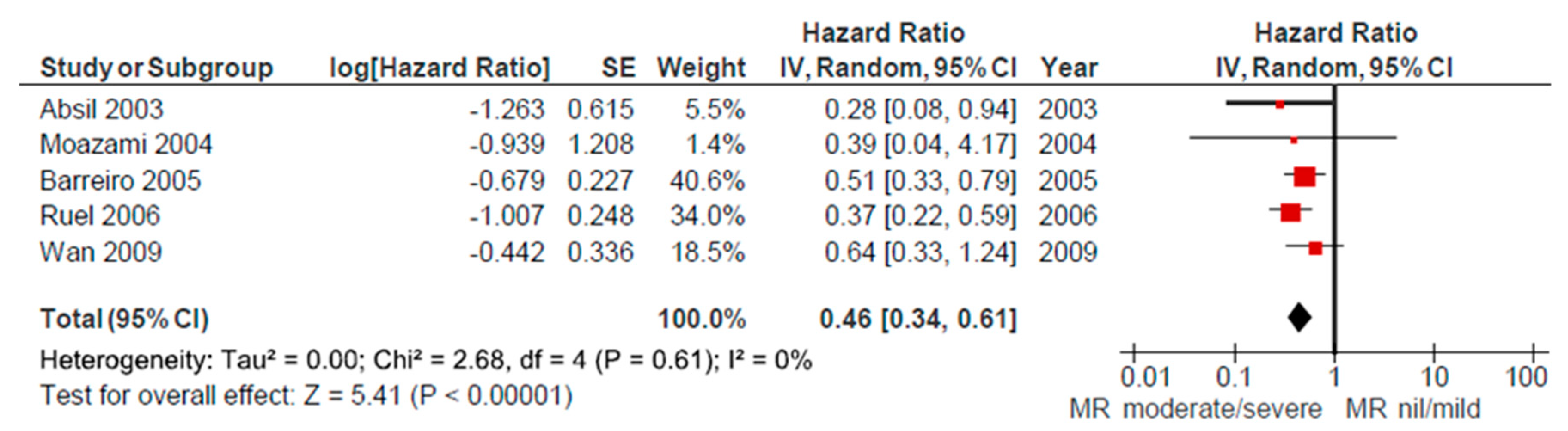
3.5. Mortality and Long-Term Survival
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kappetein, A.P.; Van Geldorp, M.; Takkenberg, J.J.; Bogers, A.J. Optimum management of elderly patients with calcified aortic stenosis. Expert Rev. Cardiovasc. Ther. 2008, 6, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, H.; Patel, P.A.; Gutsche, J.T.; Vallabhajosyula, P.; Szeto, W.Y.; MacKay, E.; Feinman, J.W.; Shah, R.; Zhou, E.; Weiss, S.J.; et al. Surgical Aortic Valve Replacement-Clinical Update on Recent Advances in the Contemporary Era. J. Cardiothorac. Vasc. Anesthesia 2016, 30, 1733–1741. [Google Scholar] [CrossRef] [PubMed]
- Nombela-Franco, L.; Ribeiro, H.B.; Urena, M.; Allende, R.; Amat-Santos, I.; DeLarochellière, R.; Dumont, E.; Doyle, D.; DeLarochellière, H.; Laflamme, J.; et al. Significant mitral regurgitation left untreated at the time of aortic valve replacement: A comprehensive review of a frequent entity in the transcatheter aortic valve replacement era. J. Am. Coll. Cardiol. 2014, 63, 2643–2658. [Google Scholar] [CrossRef] [PubMed]
- Izumi, C.; Kitai, T.; Kume, T.; Onishi, T.; Yuda, S.; Hirata, K.; Yamashita, E.; Kawata, T.; Nishimura, K.; Takeuchi, M.; et al. Effect of Left Ventricular Reverse Remodeling on Long-term Outcomes After Aortic Valve Replacement. Am. J. Cardiol. 2019, 124, 105–112. [Google Scholar] [CrossRef]
- Schubert, S.A.; Yarboro, L.T.; Madala, S.; Ayunipudi, K.; Kron, I.L.; Kern, J.A.; Ailawadi, G.; Stukenborg, G.J.; Ghanta, R.K. Natural history of coexistent mitral regurgitation after aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 1032–1042. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. ESC Scientific Document Group.2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Alghamdi, A.A.; Elmistekawy, E.M.; Singh, S.K.; Latter, D.A. Is concomitant surgery for moderate functional mitral regurgitation indicated during aortic valve replacement for aortic stenosis? A systematic review and evidence-based recommendations. J. Card. Surg. 2010, 25, 182–187. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef]
- Adams, P.B.; Otto, C.M. Lack of improvement in coexisting mitral regurgitation after relief of valvular aortic stenosis. Am. J. Cardiol. 1990, 66, 105–107. [Google Scholar] [CrossRef]
- Tunick, P.A.; Gindea, A.; Kronzon, I. Effect of aortic valve replacement for aortic stenosis on severity of mitral regurgitation. Am. J. Cardiol. 1990, 65, 1219–1221. [Google Scholar] [CrossRef]
- Harris, K.M.; Malenka, D.J.; Haney, M.F.; Jayne, J.E.; Hettleman, B.; Plehn, J.F.; Griffin, B.P. Improvement in mitral regurgitation after aortic valve replacement. Am. J. Cardiol. 1997, 80, 741–745. [Google Scholar] [CrossRef]
- Brasch, A.V.; Khan, S.S.; DeRobertis, M.A.; Kong, J.H.; Chiu, J.; Siegel, R.J. Change in mitral regurgitation severity after aortic valve replacement for aortic stenosis. Am. J. Cardiol. 2000, 85, 1271–1274. [Google Scholar] [CrossRef]
- Christenson, J.T.; Jordan, B.; Bloch, A.; Schmuziger, M. Should a regurgitant mitral valve be replaced simulataneously with a stenotic aortic valve? Tex. Heart Inst. J. 2000, 27, 350–355. [Google Scholar] [PubMed]
- Absil, B.; Dagenais, F.; Mathieu, P.; Métras, J.; Perron, J.; Baillot, R.; Bauset, R.; Doyle, D. Does moderate mitral regurgitation impact early or mid-term clinical outcome in patients undergoing isolated aortic valve replacement for aortic stenosis? Eur. J. Cardio-Thoracic Surg. 2003, 24, 217–222. [Google Scholar] [CrossRef]
- Goland, S.; Loutaty, G.; Arditi, A.; Snir, E.; Abend, I.; Caspi, A. Improvement in mitral regurgitation after aortic valve replacement. Isr. Med. Assoc. J. 2003, 5, 12–14. [Google Scholar] [PubMed]
- Tassan-Mangina, S.; Metz, D.; Nazeyllas, P.; Torossian, F.; Pop, C.; Bertrand, J.; Baehrel, B.; Elaerts, J. Factors determining early improvement in mitral regurgitation after aortic valve replacement for aortic valve stenosis: A transthoracic and transesophageal prospective study. J. Clin. Cardiol. 2003, 26, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Moazami, N.; Diodato, M.D.; Moon, M.R.; Lawton, J.S.; Pasque, M.K.; Herren, R.L.; Guthrie, T.J.; Damiano, R.J. Does functional mitral regurgitation improve with isolated aortic valve replacement? J. Card. Surg. 2004, 19, 444–448. [Google Scholar] [CrossRef]
- Barreiro, C.J.; Patel, N.D.; Fitton, T.P.; Williams, J.A.; Bonde, P.N.; Chan, V.; Alejo, D.E.; Gott, V.L.; Baumgartner, W.A. Aortic valve replacement and concomitant mitral valve regurgitation in the elderly: Impact on survival and functional outcome. Circulation 2005, 112, I443–I447. [Google Scholar]
- Ruel, M.; Kapila, V.; Price, J.; Kulik, A.; Burwash, I.G.; Mesana, T.G. Natural history and predictors of outcome in patients with concomitant functional mitral regurgitation at the time of aortic valve replacement. Circulation 2006, 114, I541–I546. [Google Scholar] [CrossRef]
- Vanden Eynden, F.; Bouchard, D.; El-Hamamsy, I.; Butnaru, A.; Demers, P.; Carrier, M.; Perrault, L.P.; Tardif, J.C.; Pellerin, M. Effect of aortic valve replacement for aortic stenosis on severity of mitral regurgitation. Ann. Thorac. Surg. 2007, 83, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Borrego, J.; Gómez-Doblas, J.J.; Cabrera-Bueno, F.; García-Pinilla, J.M.; Melero, J.M.; Porras, C.; Olalla, E.; De Teresa Galván, E. Incidence, associated factors and evolution of non-severe functional mitral regurgitation in patients with severe aortic stenosis undergoing aortic valve replacement. Eur. J. Cardio-Thoracic Surg. 2008, 34, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Unger, P.; Plein, D.; Van Camp, G.; Cosyns, B.; Pasquet, A.; Henrard, V.; De Cannière, D.; Melot, C.; Piérard, L.A.; Lancellotti, P. Effects of valve replacement for aortic stenosis on mitral regurgitation. Am. J. Cardiol. 2008, 102, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Waisbren, E.C.; Stevens, L.M.; Avery, E.G.; Picard, M.H.; Vlahakes, G.J.; Agnihotri, A.K. Changes in mitral regurgitation after replacement of the stenotic aortic valve. Ann. Thorac. Surg. 2008, 86, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Wan, C.K.; Suri, R.M.; Li, Z.; Orszulak, T.A.; Daly, R.C.; Schaff, H.V.; Sundt, T.M., III. Management of moderate functional mitral regurgitation at the time of aortic valve replacement: Is concomitant mitral valve repair necessary? J. Thorac. Cardiovasc. Surg. 2009, 137, 635–640. [Google Scholar] [CrossRef][Green Version]
- Matsumura, Y.; Gillinov, A.M.; Toyono, M.; Oe, H.; Yamano, T.; Takasaki, K.; Saraiva, R.M.; Shiota, T. Echocardiographic predictors for persistent functional mitral regurgitation after aortic valve replacement in patients with aortic valve stenosis. Am. J. Cardiol. 2010, 106, 701–706. [Google Scholar] [CrossRef]
- Takeda, K.; Matsumiya, G.; Sakaguchi, T.; Miyagawa, S.; Yamauchi, T.; Shudo, Y.; Izutani, H.; Sawa, Y. Impact of untreated mild-to-moderate mitral regurgitation at the time of isolated aortic valve replacement on late adverse outcomes. Eur. J. Cardio-Thoracic Surg. 2010, 37, 1033–1038. [Google Scholar] [CrossRef]
- Joo, H.C.; Chang, B.C.; Cho, S.H.; Youn, Y.N.; Yoo, K.J.; Lee, S. Fate of Functional Mitral Regurgitation and Predictors of Persistent Mitral Regurgitation After Isolated Aortic Valve Replacement. Ann. Thorac. Surg. 2011, 92, 82–87. [Google Scholar] [CrossRef]
- Barbanti, M.; Webb, J.G.; Hahn, R.T.; Feldman, T.; Boone, R.H.; Smith, C.R.; Kodali, S.; Zajarias, A.; Thompson, C.R.; Green, P.; et al. Placement of Aortic Transcatheter Valve Trial Investigators.. Impact of preoperative moderate/severe mitral regurgitation on 2-year outcome after transcatheter and surgical aortic valve replacement: Insight from the Placement of Aortic Transcatheter Valve (PARTNER) Trial Cohort A. Circulation 2013, 128, 2776–2784. [Google Scholar]
- Kaczorowski, D.J.; Macarthur, J.W.; Howard, J.; Kobrin, D.; Fairman, A.; Woo, Y.J. Quantitative evaluation of change in coexistent mitral regurgitation after aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2013, 145, 341–348. [Google Scholar] [CrossRef]
- Warraich, H.J.; Matyal, R.; Bergman, R.; Hess, P.E.; Khabbaz, K.; Manning, W.J.; Mahmood, F. Impact of aortic valve replacement for aortic stenosis on dynamic mitral annular motion and geometry. Am. J. Cardiol. 2013, 112, 1445–1449. [Google Scholar] [CrossRef] [PubMed]
- Wyler, S.; Emmert, M.Y.; Biaggi, P.; Seifert, B.; Grünenfelder, J.; Falk, V.; Salzberg, S. What happens to functional mitral regurgitation after aortic valve replacement for aortic stenosis? Hearth Surg. Forum 2013, 16, E238–E242. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, A.; Sheykhloo, H.; Karbasi-Afshar, R.; Saburi, A. Echocardiographic changes after aortic valve replacement: Does the failure rate of mitral valve change? ARYA Atheroscler. 2015, 11, 147–152. [Google Scholar] [PubMed]
- Sehovic, S.; Talic, A.; Kacila, M.; Tahirovic, E. The Influence of Aortic Valve Replacement on Functional Moderate—To-Severe Mitral Regurgitation in Patients with Aortic Valve Stenosis. Acta Inform. Med. 2015, 23, 147–150. [Google Scholar] [CrossRef]
- Fojt, R.; Moťovská, Z.; Budera, P.; Malý, M.; Straka, Z. Prognostic impact and change of concomitant mitral regurgitation after surgical or transcatheter aortic valve replacement for aortic stenosis. J. Cardiol. 2016, 67, 526–530. [Google Scholar] [CrossRef]
- Sorabella, R.A.; Olds, A.; Yerebakan, H.; Hassan, D.; Borger, M.A.; Argenziano, M.; Smith, C.R.; George, I. Is isolated aortic valve replacement sufficient to treat concomitant moderate functional mitral regurgitation? A propensity-matched analysis. J. Cardiothorac. Surg. 2018, 13, 72. [Google Scholar] [CrossRef]
- Brown, J.M.; O’Brien, S.M.; Wu, C.; Sikora, J.A.; Griffith, B.P.; Gammie, J.S. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: Changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J. Thorac. Cardiovasc. Surg. 2009, 137, 82–90. [Google Scholar] [CrossRef]
- Nicolini, F.; Agostinelli, A.; Fortuna, D.; Contini, G.A.; Pacini, D.; Gabbieri, D.; Zussa, C.; Pigini, F.; De Palma, R.; Gherli, T. RERIC (Registro dell’Emilia Romagna degli Interventi Cardiochirurgici) Investigators. Outcomes of patients undergoing concomitant mitral and aortic valve surgery: Results from an Italian regional cardiac surgery registry. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 763–770. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Reference | Year | Design | Total Pts n | Age | NYHA Mean | Mean Aortic Gradient | MR Measuring and Reporting | MR Change Average | Significance of MR Change |
|---|---|---|---|---|---|---|---|---|---|
| Adams et al. [11] | 1990. | retrospective | 24 | 66 ± 15 | 63.0 | semiquantitative TTE | NS | NS | |
| Tunick et al. [12] | 1990. | retrospective | 44 | 69 ± 12 | semiquantitative TTE, pulsed and continuous wave doppler | MR grade −0.39 | p < 0.05 | ||
| Harris et al. [13] | 1997. | retrospective | 28 | 75 ± 8 | 42.0 | semiquantitative TTE, pulsed, continuous and color doppler | MR jet area −3.0 cm² | p < 0.0001 | |
| Brasch et al. [14] | 2000. | retrospective | 27 | 77 ± 17 | 36.0 | semiquantitative TTE, color dopler | MR grade −0.6 | p = 0.005 | |
| Christenson et al. [15] | 2000. | retrospective | 36 | 64.0 ± 13.3 | 3.0 | semiquantitative TTE, color dopler | NS | NS | |
| Absil et al. [16] | 2003. | retrospective | 116 | 74.8 ± 7.1 | semiquantitative TTE, pulsed and continuous wave doppler | MR grade −0.37 | N/A | ||
| Goland et al. [17] | 2003. | retrospective | 30 | 72.0 ± 6.5 | TTE, color dopler, indexed jet area | MR grade −0.5 | p = 0.0012 | ||
| Tassan-Mangina et al. [18] | 2003. | prospective | 30 | 68 ± 8 | 55.0 | Color dopler jet area TTE, TOE | MR grade −0.15 | p = 0.016 | |
| Moazami et al. [19] | 2004. | retrospective | 107 | 67.1 | 2.7 | semiquantitative Color dopler, TTE | NS | NS | |
| Barreiro et al. [20] | 2005. | retrospective | 408 | 78.1 ± 5.4 | semiquantitative TTE, jet area range | N/A | N/A | ||
| Ruel et al. [21] | 2006. | retrospective | 848 | 69.6 ± 11.6 | semiquantitative TTE, color dopler | N/A | N/A | ||
| Van den Eynden et al. [22] | 2007. | retrospective | 80 | 66 ± 11 | 2.8 | 50.3 | Quantitative TTE | MR grade −0.27 | p < 0.0001 |
| Caballero-Borrego et al. [23] | 2008. | retrospective | 153 | 68.3 ± 9.2 | 54.5 | TTE, color dopler, regurgitant jet area | MR grade −0.67 | p < 0.0001 | |
| Unger et al. [24] | 2008. | prospective | 52 | 77 | 42.0 | Quantitative TTE | Rvol −8.3 mL | p < 0.0001 | |
| Waisbren et al. [25] | 2008. | retrospective | 227 | 71 ± 11 | 51.0 | Quantitative TOE | MR grade −0.43 | p < 0.0001 | |
| Wan et al. [26] | 2009. | retrospective | 190 | 74 ± 11 | 3.0 | 54.0 | semiquantitative TTE, color dopler | MR grade −0.80 | p < 0.0001 |
| Matsumura et al. [27] | 2010. | retrospective | 110 | 73 ± 10 | 43.0 | Quantitative TTE | MR jet area −3.3 cm² | p < 0.001 | |
| Takeda et al. [28] | 2010. | retrospective | 59 | 67 ± 11 | semiquantitative TTE, color dopler | MR grade −0.76 | p = 0.003 | ||
| Joo et al. [29] | 2011. | retrospective | 118 | 63 ± 13 | 2.7 | semiquantitative TTE, color dopler | MR grade −0.98 | significant | |
| Barbanti et al. [30] | 2013. | prospective | 299 | 86.2 ± 5.9 | 3.5 | 42.7 | semiquantitative TTE, color dopler | MR grade −0.47 | significant |
| Kaczorowski et al. [31] | 2013. | retrospective | 462 | 72.9 ± 10.9 | 2.7 | 44.6 | semiquantitative TTE, TOE, color dopler | MR grade −0.28 | p < 0.05 |
| Warraich et al. [32] | 2013. | retrospective | 39 | 74.0 ± 13.7 | Quantitative TOE, TTE | N/A | N/A | ||
| Wyler et al. [33] | 2013. | retrospective | 74 | 68.7 ± 11.7 | 2.6 | 54.9 | semiquantitative TTE, color dopler | NS | NS |
| Khosravi et al. [34] | 2015. | prospective | 85 | 56 ± 6.1 | 35.6 | semiquantitative TTE, color dopler | MR grade −0.64 | p < 0.01 | |
| Sehovic et al. [35] | 2015. | retrospective | 45 | 56.25 ± 7.24 | 2.2 | Quantitative TTE | MR grade −0.47 | significant | |
| Fojt et al. [36] | 2016. | retrospective | 101 | 76.1 ± 8.2 | 2.6 | 42.4 | semiquantitative TTE, color dopler | MR grade −0.55 | p < 0.001 |
| Sorabella et al. [37] | 2018. | retrospective | 660 | 78.1 ± 10.1 | semiquantitative TTE, color dopler | N/A | N/A |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilbija, I.; Matkovic, M.; Cubrilo, M.; Aleksic, N.; Milin Lazovic, J.; Cumic, J.; Tutus, V.; Jovanovic, M.; Putnik, S. The Prospects of Secondary Moderate Mitral Regurgitation after Aortic Valve Replacement —Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7335. https://doi.org/10.3390/ijerph17197335
Bilbija I, Matkovic M, Cubrilo M, Aleksic N, Milin Lazovic J, Cumic J, Tutus V, Jovanovic M, Putnik S. The Prospects of Secondary Moderate Mitral Regurgitation after Aortic Valve Replacement —Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(19):7335. https://doi.org/10.3390/ijerph17197335
Chicago/Turabian StyleBilbija, Ilija, Milos Matkovic, Marko Cubrilo, Nemanja Aleksic, Jelena Milin Lazovic, Jelena Cumic, Vladimir Tutus, Marko Jovanovic, and Svetozar Putnik. 2020. "The Prospects of Secondary Moderate Mitral Regurgitation after Aortic Valve Replacement —Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 19: 7335. https://doi.org/10.3390/ijerph17197335
APA StyleBilbija, I., Matkovic, M., Cubrilo, M., Aleksic, N., Milin Lazovic, J., Cumic, J., Tutus, V., Jovanovic, M., & Putnik, S. (2020). The Prospects of Secondary Moderate Mitral Regurgitation after Aortic Valve Replacement —Meta-Analysis. International Journal of Environmental Research and Public Health, 17(19), 7335. https://doi.org/10.3390/ijerph17197335