Clustering of Six Key Risk Behaviors for Chronic Disease among Adolescent Females

 , , ,
, , ,
Abstract
1. Introduction
- Provide a snapshot of adolescent females’ perceptions of their health and their health behaviors, and investigate whether knowledge of health guidelines is associated with adherence;
- Explore patterns of clustering of the six risk behaviors and identify correlates of these behavioral profiles, including the perceived value of different life domains, to inform preventive intervention approaches.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Self-Rated Health
2.2.2. Knowledge of Health Guidelines
2.2.3. Moderate-Vigorous Physical Activity (MVPA)
2.2.4. Sedentary Recreational Screen Time
2.2.5. Fruit and Vegetable Intake
2.2.6. Sleep
2.2.7. Alcohol Use
2.2.8. Smoking
2.2.9. Adherence to Health Guidelines
2.2.10. Perceived Value of Life Domains
2.3. Statiscial Analysis
3. Results
3.1. Self-Rated Health; Risk Behaviors; and Knowledge of, and Adherence to, Health Guidelines
3.2. Logistic Regression
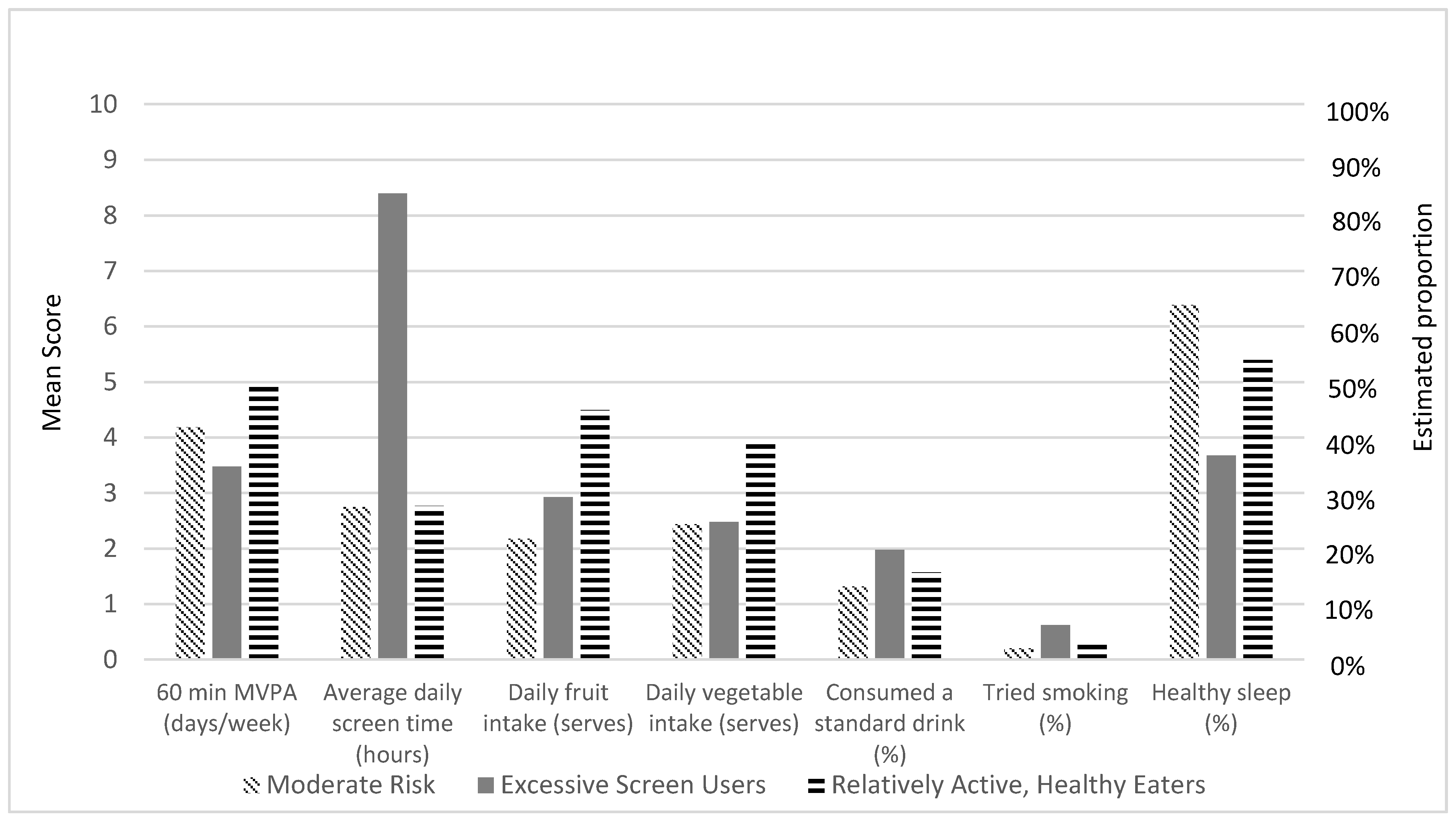
3.3. Latent Class Analysis
3.4. Asssociation of Latent Classes with Ranked Value of Life Domains
4. Discussion
4.1. Practical Implications for Public Health
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Health Behavior | Knowledge Assessment Item | Correct Response |
|---|---|---|
| Moderate-to-Vigorous Physical Activity | Based on the Australian guidelines, what do you think is the recommended amount of physical activity for your age? Moderate intensity physical activity requires some effort, but still allows you to speak easily while undertaking the activity. e.g., active play, brisk walking, recreational swimming, dancing, or riding a bike. Vigorous intensity physical activity requires more effort and makes you breathe harder and faster (“huff and puff”), e.g., running, fast cycling, and organized sports. | At least 60 min of moderate-to-vigorous intensity aerobic physical activity every day |
| Recreational Screen time | Based on Australian guidelines, what do you think is the recommended limit for recreational screen time (e.g., television, seated electronic games and computer use for entertainment purposes) for people your age? | Less than 2 h per day |
| Fruit intake | Based on Australian guidelines, please select what you believe is the recommended number of serves of fruit you should eat each day. | 2 serves per day |
| Vegetable intake | Based on Australian guidelines, please select what you believe is the recommended number of serves of vegetables you should eat each day. | 5 serves per day |
| Sleep | Please select what you think is the recommended number of hours people your age should sleep each night. | For participants between the age of 6–13 years: 9–11 h For participants between the age of 14–17 years: 8–10 h |
| Alcohol | For children and young people under 18 years of age, the safest option is to drink how many standard drinks per day? | Not drinking is the safest option |
| Tobacco | N/A | N/A |
References
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Australian Institute of Health and Welfare. The Health of Australia’s Females; Cat. no. PHE 240; AIHW: Canberra, Australia, 2019. [Google Scholar]
- Ding, D.; Rogers, K.; van der Ploeg, H.; Stamatakis, E.; Bauman, A.E. Traditional and Emerging Lifestyle Risk Behaviors and All-Cause Mortality in Middle-Aged and Older Adults: Evidence from a Large Population-Based Australian Cohort. PLoS Med. 2015, 12, e1001917. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Physical Activity Across the Life Stages; Cat. no. PHE 225; AIHW: Canberra, Australia, 2018. [Google Scholar]
- Evans-Whipp, T.; Gasser, C. Are Children and Adolescents Getting Enough Sleep? Australian Institute of Family Studies: Growing Up in Australia: The Longitudinal Study of Australian Children (LSAC) Annual Statistical Report 2018. 2019. Available online: https://growingupinaustralia.gov.au/research-findings/annual-statistical-reports-2018 (accessed on 9 August 2020).
- Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2016: Detailed Findings; AIHW: Canberra, Australia, 2017. [Google Scholar]
- Khan, A.; Burton, N.W. Is physical inactivity associated with depressive symptoms among adolescents with high screen time? Evidence from a developing country. Ment. Health Phys. Act. 2017, 12, 94–99. [Google Scholar] [CrossRef]
- Palmer, C.A.; Oosterhoff, B.; Bower, J.L.; Kaplow, J.B.; Alfano, C.A. Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. J. Psychiatr. Res. 2018, 96, 1–8. [Google Scholar] [CrossRef]
- Lawrence, D.; Johnson, S.; Hafekost, J.; de Haan, K.B.; Sawyer, M.; Ainley, J.; Zubrick, S. The Mental Health of Children and Adolescents. In Report on the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing; Department of Health: Canberra, Australia, 2015. [Google Scholar]
- Suchert, V.; Hanewinkel, R.; Isensee, B. Sedentary behavior, depressed affect, and indicators of mental well-being in adolescence: Does the screen only matter for girls? J. Adolesc. 2015, 42, 50–58. [Google Scholar] [CrossRef]
- Lundeen, E.A.; Norris, S.A.; Adair, L.S.; Richter, L.M.; Stein, A.D. Sex differences in obesity incidence: 20-year prospective cohort in South Africa. Pediatric Obes. 2016, 11, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Gary, D.; O’Malley, P.M.; Hamilton, A.; Schulenberg, J. Recent increases in depressive symptoms among US adolescents: Trends from 1991 to 2018. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 1289 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Australian 24-Hour Movement Guidelines for Children (5–12 years) and Young People (13–17 years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep; Department of Health: Canberra, Australia, 2019.
- Abula, K.; Gröpel, P.; Chen, K.; Beckmann, J. Does knowledge of physical activity recommendations increase physical activity among Chinese college students? Empirical investigations based on the transtheoretical model. J. Sport Health Sci. 2018, 7, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Haack, S.A.; Byker, C.J. Recent population adherence to and knowledge of United States federal nutrition guides, 1992–2013: A systematic review. Nutr. Rev. 2014, 72, 613–626. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Mihrshahi, S.; Bellew, W.; Bauman, A.; Ding, D. Children’s adherence to health behavior recommendations associated with reducing risk of non-communicable disease. Prev. Med. Rep. 2017, 8, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Spring, B.; Moller, A.C.; Coons, M.J. Multiple health behaviours: Overview and implications. J. Public Health 2012, 34, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Krokstad, S.; Ding, D.; Grunseit, A.C.; Sund, E.R.; Holmen, T.L.; Rangul, V.; Bauman, A. Multiple lifestyle behaviours and mortality, findings from a large population-based Norwegian cohort study—The HUNT Study. BMC Public Health 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2016, 41, 311–327. [Google Scholar] [CrossRef]
- Lazzeri, G.; Panatto, D.; Domnich, A.; Arata, L.; Pammolli, A.; Simi, R.; Giacchi, M.V.; Amicizia, D.; Gasparini, R. Clustering of health-related behaviors among early and mid-adolescents in Tuscany: Results from a representative cross-sectional study. J. Public Health (Oxf) 2018, 40, e25–e33. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Karunamuni, N.; Spence, J.C.; Storey, K.; Forbes, L.; Raine, K.; Cameron Wild, T.; McCargar, L. Chronic Disease–Related Lifestyle Risk Factors in a Sample of Canadian Adolescents. J. Adolesc. Health 2009, 44, 606–609. [Google Scholar] [CrossRef]
- Champion, K.E.; Parmenter, B.; McGowan, C.; Spring, B.; Wafford, Q.E.; Gardner, L.A.; Thornton, L.; McBride, N.; Barrett, E.L.; Teesson, M.; et al. Effectiveness of school-based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: A systematic review and meta-analysis. Lancet Digit. Health 2019. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; National Health and Medical Research Council: Canberra, Australia, 2009. [Google Scholar]
- Ridgers, N.D.; Timperio, A.; Crawford, D.; Salmon, J. Validity of a brief self-report instrument for assessing compliance with physical activity guidelines amongst adolescents. J. Sci. Med. Sport 2012, 15, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Booth, M.; Okely, A.D. The reliability of the adolescent sedentary activity questionnaire (ASAQ). Prev. Med. 2007, 45, 71–74. [Google Scholar] [CrossRef]
- Rustihauser, I.; Webb, K.; Abraham, B.; Allsopp, R. Evaluation of Short Dietary Questions from the 1995 NNS; Commonwealth Department of Health and Aged Care: Canberra, Australia, 2001.
- Golley, R.K.; Maher, C.A.; Matricciani, L.; Olds, T.S. Sleep duration or bedtime? Exploring the association between sleep timing behaviour, diet and BMI in children and adolescents. Int. J. Obes. 2013, 37, 546–551. [Google Scholar] [CrossRef]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behavior Surveillance—United States, 2017. MMWR Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef] [PubMed]
- Muthen, L.K.; Muthen, B.O. Mplus Users Guide, 7th ed.; Muthen & Muthen: Los Angeles, CA, USA, 1998–2012. [Google Scholar]
- Asparouhov, T.; Muthen, B.O. Auxiliary Variables in Mixture Modeling: A 3-Step Approach Using Mplus. Mplus Web Notes: No. 15. 2013. Available online: https://statmodel.com/examples/webnotes/AuxMixture_submitted_corrected_webnote (accessed on 25 May 2020).
- Australian Bureau of Statistics. National Health Survey: First Results, 2017–2018; ABS cat. no. 4364.0.55.001; ABS: Canberra, Australia, 2018. [Google Scholar]
- Michaelson, V.; Pickett, W.; Vandemeer, E.; Taylor, B.; Davison, C. A mixed methods study of Canadian adolescents’ perceptions of health. Int. J. Qual. Stud. Health Well-Being 2016, 11, 32891. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Borraccino, A.; Pera, R.; Lemma, P. “What being healthy means to me”: A qualitative analysis uncovering the core categories of adolescents’ perception of health. PLoS ONE 2019, 14, e0218727. [Google Scholar] [CrossRef] [PubMed]
- Gasser, C.; Evans-Whipp, T.; Terhaag, S. The Physical Health of Australian Children. Australian Institute of Family Studies: Growing Up in Australia: The Longitudinal Study of Australian Children (LSAC) Annual Statistical Report 2018. 2019. Available online: https://aifs.gov.au/publications/growing-australia-longitudinal-study-australian-children-lsac (accessed on 9 August 2020).
- Slade, T.; Chapman, C.; Swift, W.; Keyes, K.; Tonks, Z.; Teesson, M. Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open 2016, 6, e011827. [Google Scholar] [CrossRef]
- Dir, A.L.; Bell, R.L.; Adams, Z.W.; Hulvershorn, L.A. Gender Differences in Risk Factors for Adolescent Binge Drinking and Implications for Intervention and Prevention. Front. Psychiatry 2017, 8, 289. [Google Scholar] [CrossRef]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Adair, L.S. Obesogenic clusters: Multidimensional adolescent obesity-related behaviors in the U.S. Ann. Behav. Med. 2008, 36, 217–230. [Google Scholar] [CrossRef]
- Peiró-Velert, C.; Valencia-Peris, A.; González, L.M.; García-Massó, X.; Serra-Añó, P.; Devís-Devís, J. Screen media usage, sleep time and academic performance in adolescents: Clustering a self-organizing maps analysis. PLoS ONE 2014, 9, e99478. [Google Scholar] [CrossRef]
- Kristjánsson, Á.L.; Sigfúsdóttir, I.D.; Allegrante, J.P. Health Behavior and Academic Achievement Among Adolescents: The Relative Contribution of Dietary Habits, Physical Activity, Body Mass Index, and Self-Esteem. Health Educ. Behav. 2008, 37, 51–64. [Google Scholar] [CrossRef]
- Miller, M.L.; Thayer, J.F. On the Nature of Self-Monitoring: Relationships with Adjustment and Identity. Personal. Soc. Psychol. Bull. 1988, 14, 544–553. [Google Scholar] [CrossRef]
- Locke, E.A. Motivation through conscious goal setting. Appl. Prev. Psychol. 1996, 5, 117–124. [Google Scholar] [CrossRef]
- Perkins, H.W.; Berkowitz, A.D. Perceiving the community norms of alcohol use among students: Some research implications for campus alcohol education programming. Int. J. Addict. 1986, 21, 961–976. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Learning Theory; Prentice Hall: Upper Saddle River, NJ, USA, 1977. [Google Scholar]
- Prochaska, J.J.; Spring, B.; Nigg, C.R. Multiple health behavior change research: An introduction and overview. Prev. Med. 2008, 46, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Arias, N.; Calvo, M.D.; Benítez-Andrades, J.A.; Álvarez, M.J.; Alonso-Cortés, B.; Benavides, C. Socioeconomic Status in Adolescents: A Study of Its Relationship with Overweight and Obesity and Influence on Social Network Configuration. Int. J. Environ. Res. Public Health 2018, 15, 2014. [Google Scholar] [CrossRef] [PubMed]

| Behaviour | Knowledge of Guidelines | Adherence to Guidelines | ||||
|---|---|---|---|---|---|---|
| Mean | SD | N | % | N | % | |
| MVPA for at least 60 min | 4.30 (days/week) | 1.77 | 175 | 25.70 | 76 | 11.3 |
| Recreational Screen time | 3.06 (h/day) | 1.93 | 352 | 51.80 | 246 | 36.6 |
| Fruit intake | 2.69 (serves/day) | 1.40 | 247 | 36.50 | 541 | 80.50 |
| Vegetable intake | 2.75 (serves/day) | 1.32 | 237 | 35.00 | 74 | 11.00 |
| Sleep | 8.63 (h/night) | 1.08 | 482 | 70.90 | 382 | 60.40 |
| Alcohol | 14.1% (n = 59) consumed a standard drink | - | 633 | 93.60 | 360 | 85.90 |
| Smoking | 2.4% (n = 16) tried smoking | - | - | - | - | - |
| Classes | AIC | aBIC | Entropy | H0 Loglikelihood Value | LMRT (p-Value) | BLRT p-Value |
|---|---|---|---|---|---|---|
| 1 | 11,485.354 | 11,500.090 | - | −5731.677 | - | - |
| 2 | 11,318.814 | 11,344.267 | 0.926 | −5640.407 | 179.103 (p = 0.384) | <0.001 |
| 3 * | 11,192.008 | 11,228.177 | 0.800 | −5569.004 | 140.118 (p < 0.001) | <0.001 |
| 4 | 11,105.894 | 11,152.780 | 0.809 | −5517.947 | 100.192 (p = 0.212) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gardner, L.A.; Champion, K.E.; Parmenter, B.; Grummitt, L.; Chapman, C.; Sunderland, M.; Thornton, L.; McBride, N.; The Health4Life Team; Newton, N.C. Clustering of Six Key Risk Behaviors for Chronic Disease among Adolescent Females. Int. J. Environ. Res. Public Health 2020, 17, 7211. https://doi.org/10.3390/ijerph17197211
Gardner LA, Champion KE, Parmenter B, Grummitt L, Chapman C, Sunderland M, Thornton L, McBride N, The Health4Life Team, Newton NC. Clustering of Six Key Risk Behaviors for Chronic Disease among Adolescent Females. International Journal of Environmental Research and Public Health. 2020; 17(19):7211. https://doi.org/10.3390/ijerph17197211
Chicago/Turabian StyleGardner, Lauren A., Katrina E. Champion, Belinda Parmenter, Lucinda Grummitt, Cath Chapman, Matthew Sunderland, Louise Thornton, Nyanda McBride, The Health4Life Team, and Nicola C. Newton. 2020. "Clustering of Six Key Risk Behaviors for Chronic Disease among Adolescent Females" International Journal of Environmental Research and Public Health 17, no. 19: 7211. https://doi.org/10.3390/ijerph17197211
APA StyleGardner, L. A., Champion, K. E., Parmenter, B., Grummitt, L., Chapman, C., Sunderland, M., Thornton, L., McBride, N., The Health4Life Team, & Newton, N. C. (2020). Clustering of Six Key Risk Behaviors for Chronic Disease among Adolescent Females. International Journal of Environmental Research and Public Health, 17(19), 7211. https://doi.org/10.3390/ijerph17197211