Assessing the Accessibility of Home-Based Healthcare Services for the Elderly: A Case from Shaanxi Province, China


Abstract
1. Introduction
2. Literature Review
3. Analysis Framework and Index System
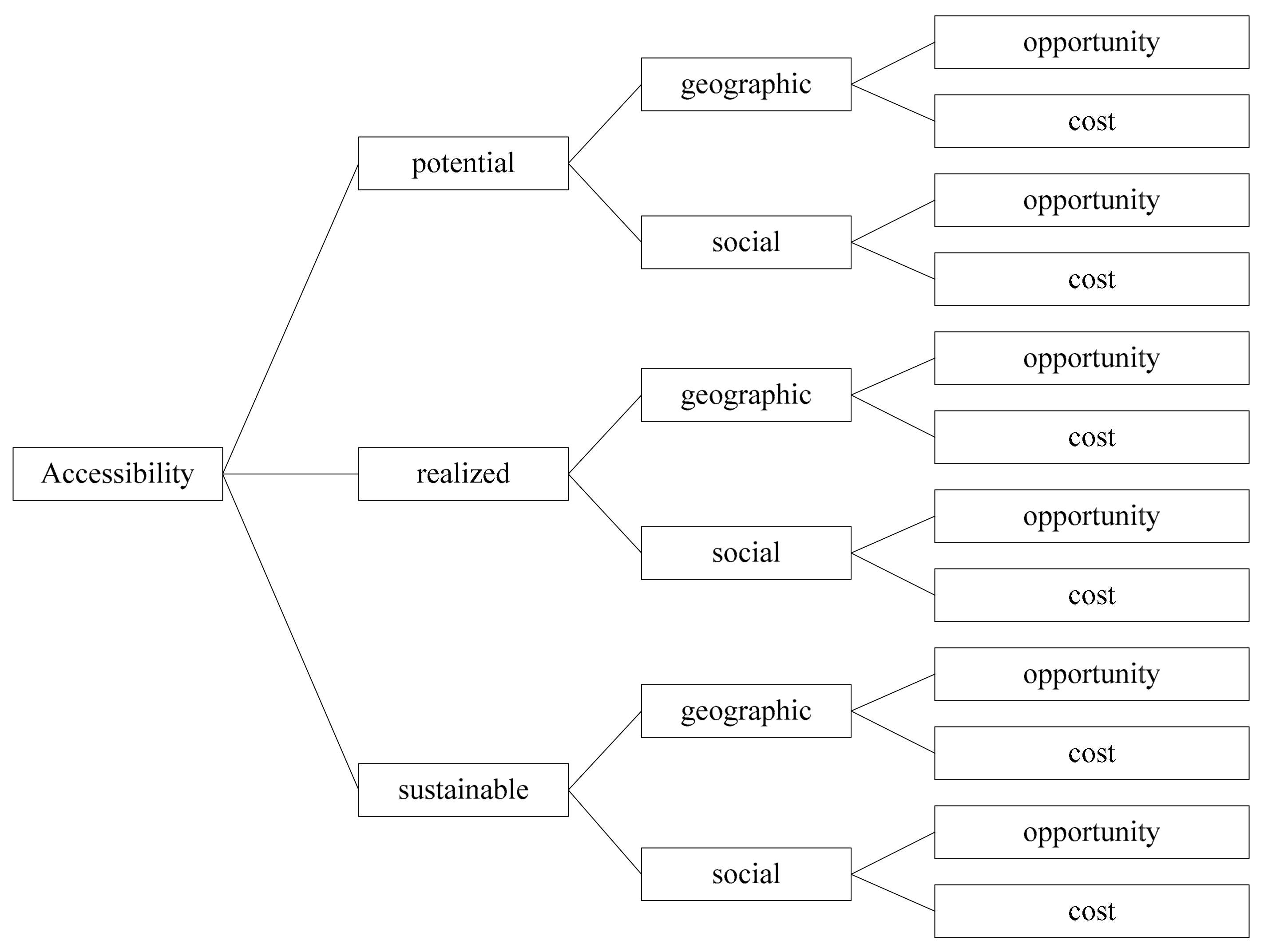
3.1. Analysis Framework
3.2. Index System
4. Empirical Analysis
4.1. Data Resource
4.2. Results
4.3. Evaluation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kong, F.; Xu, L.; Kong, M.; Li, S.; Zhou, C.; Zhang, J.; Ai, B. Association between Socioeconomic Status, Physical Health and Need for Long-Term Care among the Chinese Elderly. Int. J. Environ. Res. Public Health 2019, 16, 2124. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.Y.C.; Wong, E.L.Y.; Chung, R.Y.; Law, S.C.; Threapleton, D.; Kiang, N.; Chau, P.; Wong, S.Y.; Woo, J.; Yeoh, E.K. Collaborate across silos: Perceived Barriers to Integration of Care for the Elderly from the Perspectives of Service Providers. Int. J. Health Plan. Manag. 2018, 33, 768–780. [Google Scholar] [CrossRef] [PubMed]
- Gu, S. A Comparative Study of Increasing Demand for Health Care for Older People in China and the United Kingdom. World Sci. Res. J. 2020, 6, 218–251. [Google Scholar] [CrossRef]
- Anderson, R. A Behavioral Model of Families’ Use of Health Services; Research Series No. A25; Center for Health Administration Studies; University of Chicago: Chicago, IL, USA, 1968; p. 125. [Google Scholar]
- Acheson, R.M. Primary Care: Where Medicine Fails. Br. Med. J. 1975, 15–77. [Google Scholar] [CrossRef]
- Salkever, D.S. Economic Class and Differential Accessibility to Care: Comparisons among Health Care Systems. Int. J. Health Serv. 1975, 5, 373–395. [Google Scholar] [CrossRef] [PubMed]
- Aday, L.A.; Andersen, R.; Fleming, G.V. Health Care in the U.S.: Equitable for Whom? Sage: Beverly Hills, CA, USA, 1980. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The Concept of Accessibility: Definition and Relationship to Consumer Satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Goddard, M.; Smith, P. Equity of Accessibility to Health Care Services: Theory and Evidence from the UK. Soc. Sci. Med. 2001, 53, 1149–1162. [Google Scholar] [CrossRef]
- Peters, D.H.; Garg, A.; Bloom, G.; Walker, D.G.; Brieger, W.R.; Hafizur Rahman, M. Poverty and Access to Health Care in Developing Countries. Ann. N. Y. Acad. Sci. 2008, 1136, 161–171. [Google Scholar] [CrossRef]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred Accessibility to Health Care: Conceptualising Accessibility at the Interface of Health Systems and Populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef]
- Carpentieri, G.; Guida, C.; Masoumi, H.E. Multimodal Accessibility to Primary Health Services for the Elderly: A Case Study of Naples, Italy. Sustainability 2020, 12, 781. [Google Scholar] [CrossRef]
- Quanyun, S.; Li, J.; Yu, W.; Zhichao, Y. Accessibility of Financial Services, Digital Finance and Household Consumption in China: Evidence from Micro Data. N. Am. J. Econ. Financ. 2020, 101213. [Google Scholar] [CrossRef]
- Jadhav, A.V. Rural Elderly and Accessibility to Palliative care: A Public Health Perspective. Indian J. Palliat. Care 2020, 26, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Meyer, P.; Jin, L. Spatial Accessibility to Health Care and Elderly Ambulatory Care Sensitive Hospitalizations. Public Health 2019, 169, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.A.; Wong, G.; Jones, A.P.; Steel, N. Accessibility to Primary Care for Socioeconomically Disadvantaged Older People in Rural Areas: A Realist Review. BMJ Open 2016, 6, e010652. [Google Scholar] [CrossRef] [PubMed]
- Mosca, I.; Van Der Wees, P.J.; Mot, E.S.; Wammes, J.J.; Jeurissen, P.P. Sustainability of Long-term Care: Puzzling Tasks Ahead for Policy-Makers. Int. J. Health Policy Manag. 2016, 6, 195–205. [Google Scholar] [CrossRef]
- Xu, X.; Chen, L. Projection of Long-Term Care Costs in China, 2020–2050: Based on the Bayesian Quantile Regression Method. Sustainability 2019, 11. [Google Scholar] [CrossRef]
- Hodge, H.; Carson, D.; Carson, D.; Newman, L.; Garrett, J. Using Internet Technologies in Rural Communities to Accessibility Services: The Views of Older People and Service Providers. J. Rural Stud. 2017, 54, 469–478. [Google Scholar] [CrossRef]
- Shrestha, B.P.; Millonig, A.; Hounsell, N.B.; Mcdonald, M. Review of Public Transport Needs of Older People in European Context. J. Popul. Ageing 2017, 10, 343–361. [Google Scholar] [CrossRef]
- Suurmond, J.; Rosenmöller, D.L.; el Mesbahi, H.; Lamkaddem, M.; Essink-Bot, M.L. Barriers in Accessibility to Home Care Services among Ethnic Minority and Dutch Elderly—A Qualitative Study. Int. J. Nurs. Stud. 2016, 54, 23–35. [Google Scholar] [CrossRef]
- Van Gaans, D.; Dent, E. Issues of Accessibility to Health Services by Older Australians: A Review. Public Health Rev. 2018, 39, 485–489. [Google Scholar] [CrossRef]
- Israel, S. How Social Policies can Improve Financial Accessibility of Healthcare: A Multi-level Analysis of Unmet Medical Need in European Countries. Int. J. Equity Health 2016, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Baxter, L.M.; Eldin, M.S.; Al Mohammed, A.; Saim, M.; Checchi, F. Accessibility to Care for Non-communicable Diseases in Mosul, Iraq between 2014 and 2017: A Rapid Qualitative Study. Confl. Health 2018, 48. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, T.C.; Goldsmith, L.J. Accessibility in Health Services Research: The Battle of the Frameworks. Nurs. Outlook 2005, 53, 274–280. [Google Scholar] [CrossRef]
- Donabedian, A. Aspects of Medical Care Administration: Specifying Requirements for Health Care; Harvard University Press: Cambridge, UK, 1973. [Google Scholar]
- Khan, A.A.; Bhardwaj, S.M. Accessibility to Health Care: A Conceptual Framework and its Relevance to Health Care Planning. Eval. Health Prof. 1994, 17, 60–76. [Google Scholar] [CrossRef]
- Leporatti, L.; Montefiori, M. The Challenge of Organizing Elderly Care Programmes: Optimal Policy Design under Complete and Asymmetric Information. BE J. Econ. Anal. Policy 2019, 20, 1–15. [Google Scholar] [CrossRef]
- Yee, C.A.; Legler, A.; Davies, M.; Prentice, J.; Pizer, S. Priority Access to Health Care: Evidence from An Exogenous Policy Shock. Health Econ. 2020, 29, 306–323. [Google Scholar] [CrossRef]
- Güeita-Rodriguez, J.; Famoso-Pérez, P.; Salom-Moreno, J.; Carrasco-Garrido, P.; Pérez-Corrales, J.; Palacios-Ceña, D. Challenges Affecting Access to Health and Social Care Resources and Time Management among Parents of Children with Rett Syndrome: A Qualitative Case Study. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef]
- Hamano, T.; Takeda, M.; Tominaga, K.; Sundquist, K.; Nabika, T. Is Accessibility to Dental Care Facilities in Rural Areas Associated with Number of Teeth in Elderly Residents? Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]


{kind=link}
| Accessibility | Geographic | Social | ||
|---|---|---|---|---|
| Potential | Opportunity | Opportunity | ||
| Cost | Cost | |||
| Realized | Opportunity | Opportunity | ||
| Cost | Cost | |||
| Total Index | First Level | Secondary Level | Measurement Indicators (Number) |
|---|---|---|---|
| Accessibility index system of healthcare services for the elderly | Potential accessibility | Geographic accessibility opportunity | Satisfaction with community life (1) |
| Convenience to community healthcare service center (2) | |||
| Geographic accessibility cost | Reasonable level of expenditure for basic healthcare service (3) | ||
| Social accessibility opportunity | Understanding of healthcare service (4) | ||
| attention to healthcare service (5) | |||
| Social accessibility cost | Perfection of the information platform for healthcare service (6) | ||
| Frequency of policy publicity for healthcare service (7) | |||
| Realized accessibility | Geographic accessibility opportunity | Completeness of the content of healthcare service in community (8) | |
| Adequacy of resources of healthcare service in community (9) | |||
| Geographic accessibility cost | Willingness to use healthcare service (10) | ||
| Frequency of use of healthcare service (11) | |||
| Social accessibility opportunity | Trust in using healthcare service (12) | ||
| Benefits of using healthcare services for the elderly (13) | |||
| Social accessibility cost | Convenience of using healthcare services for the elderly (14) | ||
| Waiting time for healthcare service (15) | |||
| Sustainable accessibility | Geographic accessibility opportunity | Ability to solve problems of healthcare personnel (16) | |
| Trust of healthcare personnel in door-to-door care for the elderly (17) | |||
| Geographic accessibility cost | Timeliness of door-to-door care (18) | ||
| Caring for the elderly by healthcare personnel (19) | |||
| Social accessibility opportunity | Willingness of elderly people to participate in social activity (20) | ||
| Health status of elderly people (21) | |||
| Social accessibility cost | Prospects of healthcare services for the elderly in community (22) | ||
| Economic pressure on healthcare services for the elderly (23) |
| Individual Characteristics | Frequency | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 405 | 42.7 |
| Female | 543 | 57.3 |
| Age | ||
| 60–69 | 415 | 43.8 |
| 70–79 | 325 | 34.3 |
| Above 80 | 208 | 21.9 |
| Registered permanent residence | ||
| City | 518 | 54.6 |
| Countryside | 430 | 45.4 |
| Political status | ||
| Communist Party | 247 | 26.1 |
| The masses | 689 | 72.7 |
| Democratic parties | 12 | 1.3 |
| Health status | ||
| Very bad | 43 | 4.5 |
| Bad | 179 | 18.9 |
| Average | 249 | 26.3 |
| Better | 330 | 34.8 |
| Well | 147 | 15.5 |
| Education | ||
| Elementary | 455 | 48.0 |
| Junior | 249 | 26.3 |
| High | 171 | 18.0 |
| Junior college | 49 | 5.2 |
| Bachelor | 24 | 2.5 |
| Indicator | Mean | Median | Standard Deviation | Kurtosis | Skewness |
|---|---|---|---|---|---|
| 1 | 4.52 | 5 | 0.69 | 1.00 | −1.28 |
| 2 | 4.59 | 5 | 0.87 | 4.56 | −2.25 |
| 3 | 3.75 | 4 | 1.46 | −0.56 | −0.94 |
| 4 | 3.64 | 4 | 1.31 | −1.00 | −0.55 |
| 5 | 3.24 | 3 | 1.31 | −1.15 | −0.18 |
| 6 | 2.15 | 2 | 1.18 | −0.12 | 0.89 |
| 7 | 3.20 | 3 | 1.30 | −1.02 | −0.23 |
| 8 | 2.74 | 3 | 1.22 | −0.90 | 0.29 |
| 9 | 3.04 | 3 | 1.13 | −0.85 | −0.03 |
| 10 | 2.95 | 3 | 1.19 | −0.76 | 0.05 |
| 11 | 3.62 | 4 | 1.17 | −0.56 | −0.62 |
| 12 | 3.64 | 4 | 1.30 | −0.51 | −0.76 |
| 13 | 2.99 | 3 | 1.39 | −1.24 | −0.12 |
| 14 | 3.30 | 3 | 1.04 | 0.11 | −0.54 |
| 15 | 2.08 | 1 | 1.50 | −0.71 | 0.96 |
| 16 | 2.86 | 3 | 1.14 | −0.61 | 0.10 |
| 17 | 3.58 | 4 | 1.30 | −0.63 | −0.68 |
| 18 | 3.05 | 3 | 1.19 | −0.89 | −0.24 |
| 19 | 2.60 | 2 | 1.27 | −0.92 | 0.36 |
| 20 | 3.47 | 4 | 1.29 | −0.81 | −0.54 |
| 21 | 3.45 | 4 | 1.10 | −0.78 | −0.25 |
| 22 | 3.11 | 3 | 1.40 | −1.35 | −0.14 |
| 23 | 4.07 | 4 | 1.13 | 0.56 | −1.13 |
| Kaiser-Meyer-Olkin Measure with Adequacy Sample | 0.858 | |
| Bartlett’s sphericity test | Approximate chi-square | 5836.174 |
| Degrees of freedom. | 253 | |
| Significance | 0.000 | |
| Common Factors | Initial Eigenvalues | Rotating Sum of Squares Loading | ||||
|---|---|---|---|---|---|---|
| Total | Variance (%) | Cumulated (%) | Total | Variance (%) | Cumulated (%) | |
| 1 | 6.379 | 27.734 | 27.734 | 3.685 | 16.020 | 16.020 |
| 2 | 2.870 | 12.479 | 40.213 | 3.404 | 14.801 | 30.821 |
| 3 | 1.559 | 6.778 | 46.991 | 2.261 | 9.831 | 40.652 |
| 4 | 1.298 | 5.643 | 52.634 | 1.950 | 8.480 | 49.132 |
| 5 | 1.247 | 5.424 | 58.058 | 1.832 | 7.966 | 57.097 |
| 6 | 1.162 | 5.052 | 63.110 | 1.383 | 6.013 | 63.110 |
| Index | Component 1 | Component 2 | Component 3 | Component 4 | Component 5 | Component 6 |
|---|---|---|---|---|---|---|
| 1 | 0.011 | 0.078 | 0.197 | 0.017 | 0.070 | 0.406 |
| 2 | −0.004 | 0.107 | 0.032 | 0.796 | 0.203 | −0.043 |
| 3 | 0.158 | −0.183 | 0.509 | −0.028 | −0.344 | 0.155 |
| 4 | 0.128 | 0.174 | 0.169 | 0.207 | 0.742 | 0.099 |
| 5 | 0.099 | 0.172 | 0.165 | 0.160 | 0.808 | 0.057 |
| 6 | 0.114 | 0.766 | −0.037 | 0.202 | 0.189 | 0.036 |
| 7 | 0.175 | 0.553 | 0.057 | 0.113 | 0.207 | 0.250 |
| 8 | 0.157 | 0.747 | 0.133 | 0.309 | 0.006 | 0.052 |
| 9 | 0.019 | 0.683 | 0.260 | 0.302 | −0.079 | 0.097 |
| 10 | 0.167 | 0.459 | 0.560 | 0.259 | 0.200 | 0.043 |
| 11 | 0.111 | 0.226 | 0.738 | 0.068 | 0.138 | 0.043 |
| 12 | 0.912 | 0.003 | 0.033 | 0.055 | 0.022 | 0.065 |
| 13 | −0.053 | 0.380 | 0.081 | 0.766 | 0.160 | 0.007 |
| 14 | 0.289 | 0.493 | 0.375 | −0.028 | 0.111 | −0.160 |
| 15 | 0.110 | 0.631 | 0.114 | −0.244 | 0.327 | −0.121 |
| 16 | 0.793 | 0.295 | 0.135 | −0.088 | 0.078 | 0.041 |
| 17 | 0.901 | −0.034 | 0.093 | 0.015 | 0.022 | 0.031 |
| 18 | 0.859 | 0.196 | 0.151 | −0.040 | 0.032 | 0.051 |
| 19 | 0.626 | 0.407 | 0.021 | 0.124 | 0.195 | 0.145 |
| 20 | 0.028 | 0.093 | 0.690 | 0.008 | 0.255 | 0.062 |
| 21 | 0.077 | 0.067 | −0.030 | −0.095 | 0.194 | 0.718 |
| 22 | 0.084 | −0.036 | −0.009 | 0.056 | −0.168 | 0.712 |
| 23 | 0.093 | 0.145 | 0.520 | 0.498 | −0.005 | 0.039 |
| Sub-Accessibility | Measurement Indicators | Percentage of Total Accessibility Weight (Rank) | Percentage of Sub-Accessibility Weight |
|---|---|---|---|
| Potential Accessibility | 1 | 0.0256 (23) | 0.0864 |
| 2 | 0.0389 (17) | 0.1314 | |
| 3 | 0.0452 (11) | 0.1527 | |
| 4 | 0.0499 (3) | 0.1684 | |
| 5 | 0.0479 (5) | 0.1620 | |
| 6 | 0.0441 (13) | 0.1490 | |
| 7 | 0.0445 (12) | 0.1502 | |
| Realized Accessibility | 8 | 0.0461 (10) | 0.1232 |
| 9 | 0.0473 (8) | 0.1264 | |
| 10 | 0.0554 (1) | 0.1481 | |
| 11 | 0.0435 (15) | 0.1162 | |
| 12 | 0.0358 (21) | 0.0956 | |
| 13 | 0.0475 (7) | 0.1270 | |
| 14 | 0.0478 (6) | 0.1278 | |
| 15 | 0.0508 (2) | 0.1358 | |
| Sustainable Accessibility | 16 | 0.0469 (9) | 0.1422 |
| 17 | 0.0360 (20) | 0.1090 | |
| 18 | 0.0436 (14) | 0.1322 | |
| 19 | 0.0498 (4) | 0.1510 | |
| 20 | 0.0373 (19) | 0.1130 | |
| 21 | 0.0388 (18) | 0.1175 | |
| 22 | 0.0350 (22) | 0.1059 | |
| 23 | 0.0427 (16) | 0.1293 |
| Potential Accessibility Indicators | Score | Realized Accessibility Indicators | Score | Sustainable Accessibility Indicators | Score |
|---|---|---|---|---|---|
| 1 | 4.52 | 8 | 2.74 | 16 | 2.86 |
| 2 | 3.75 | 9 | 3.04 | 17 | 3.58 |
| 3 | 4.59 | 10 | 2.95 | 18 | 3.05 |
| 4 | 3.64 | 11 | 3.62 | 19 | 2.60 |
| 5 | 3.24 | 12 | 3.64 | 20 | 3.47 |
| 6 | 2.15 | 13 | 2.99 | 21 | 3.45 |
| 7 | 3.20 | 14 | 3.30 | 22 | 3.11 |
| 15 | 2.08 | 23 | 4.07 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di, X.; Wang, L.; Dai, X.; Yang, L. Assessing the Accessibility of Home-Based Healthcare Services for the Elderly: A Case from Shaanxi Province, China. Int. J. Environ. Res. Public Health 2020, 17, 7168. https://doi.org/10.3390/ijerph17197168
Di X, Wang L, Dai X, Yang L. Assessing the Accessibility of Home-Based Healthcare Services for the Elderly: A Case from Shaanxi Province, China. International Journal of Environmental Research and Public Health. 2020; 17(19):7168. https://doi.org/10.3390/ijerph17197168
Chicago/Turabian StyleDi, Xiaodong, Lijian Wang, Xiuliang Dai, and Liu Yang. 2020. "Assessing the Accessibility of Home-Based Healthcare Services for the Elderly: A Case from Shaanxi Province, China" International Journal of Environmental Research and Public Health 17, no. 19: 7168. https://doi.org/10.3390/ijerph17197168
APA StyleDi, X., Wang, L., Dai, X., & Yang, L. (2020). Assessing the Accessibility of Home-Based Healthcare Services for the Elderly: A Case from Shaanxi Province, China. International Journal of Environmental Research and Public Health, 17(19), 7168. https://doi.org/10.3390/ijerph17197168