How Do German General Practitioners Assess Medical Specialist Care Needs of Nursing Home Residents? Results of a Postal Survey in North-Western Germany

 , , , and
, , , and
Abstract
1. Introduction
- -
- How do GPs rate specialist care needs of nursing home residents in Germany?
- -
- How do they view their coordination function, the appropriateness of their qualification for nursing home care, and the provision of service by only one practice?
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Respondents
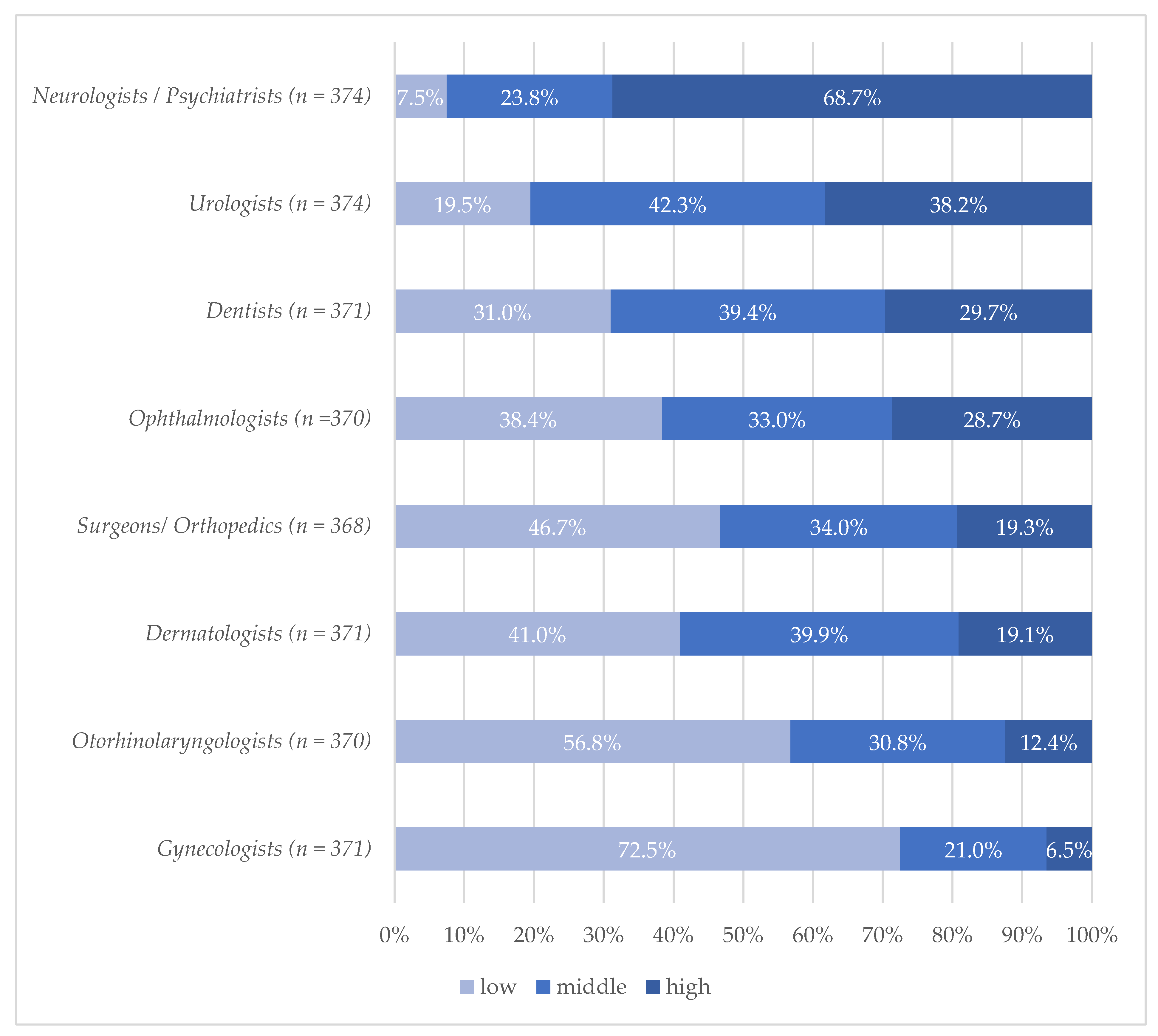
3.2. Opinions on Care Needs of Nursing Home Residents by Different Specialists
3.3. Views on Coordination of Care and Referrals
3.4. Opinions about Qualification and Single-Practice Policy
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Statistisches Bundesamt. Pflegestatistik 2017—Pflege im Rahmen der Pflegeversicherung—Deutschlandergebnisse. 2018. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Publikationen/Downloads-Pflege/pflege-deutschlandergebnisse-5224001179004.pdf?__blob=publicationFile (accessed on 28 June 2020).
- Gordon, A.L.; Franklin, M.; Bradshaw, L.; Logan, P.; Elliott, R.; Gladman, J.R.F. Health status of UK care home residents: A cohort study. Age Ageing 2014, 43, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Boscardin, W.J.; Steinman, M.A.; Schwartz, J.B. Patterns of chronic co-morbid medical conditions in older residents of U.S. nursing homes: Differences between the sexes and across the agespan. J. Nutr. Health Aging 2014, 18, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, A.; Behrendt, S.; Chrysanthi, T.; Stieglitz, K.; Breitkreuz, T.; Grobe, T.; Klauber, J. Qualitätsmessung mit Routinedaten in Deutschen Pflegeheimen: Eine erste Standortbestimmung. In Pflege-Report 2018: Qualität in der Pflege, 1st ed.; Jacobs, K., Kuhlmey, A., Greß, S., Klauber, J., Schwinger, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Briggs, R.; Robinson, S.; Martin, F.; O’Neill, D. Standards of medical care for nursing home residents in Europe. Eur. Geriatr. Med. 2012, 3, 365–367. [Google Scholar] [CrossRef]
- Amblàs-Novellas, J.; Santaeugènia, S.J.; Vela, E.; Clèries, M.; Contel, J.C. What lies beneath: A retrospective, population-based cohort study investigating clinical and resource-use characteristics of institutionalized older people in Catalonia. BMC Geriatr. 2020, 20, 187. [Google Scholar] [CrossRef] [PubMed]
- Balzer, K.; Butz, S.; Bentzel, J.; Boulkhemair, D.; Lühmann, D. Medical specialist attendance in nursing homes. GMS Health Technol. Assess. 2013, 9. [Google Scholar] [CrossRef]
- Kleina, T.; Horn, A.; Suhr, R.; Schaeffer, D. Zur Entwicklung der ärztlichen Versorgung in stationären Pflegeeinrichtungen—Ergebnisse einer empirischen Untersuchung. Gesundheitswesen 2017, 79, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.; Czwikla, J.; Tsiasioti, C.; Schwinger, A.; Gand, D.; Schmiemann, G.; Schmidt, A.; Wolf-Ostermann, K.; Kloep, S.; Heinze, F.; et al. Differences in medical specialist utilization among older people in need of long-term care—Results from German health claims data. Int. J. Equity Health 2020, 19. [Google Scholar] [CrossRef] [PubMed]
- Iliffe, S.; Davies, S.L.; Gordon, A.L.; Schneider, J.; Dening, T.; Bowman, C.; Gage, H.; Martin, F.C.; Gladman, J.R.F.; Victor, C.R.; et al. Provision of NHS generalist and specialist services to care homes in England: Review of surveys. Prim. Health Care Res. Dev. 2015, 17, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Rothgang, H.; Borchert, L.; Müller, R.; Unger, R. GEK-Pflegereport 2008. Schwerpunktthema: Medizinische Versorgung in Pflegeheimen. 2008. Available online: https://www.barmer.de/blob/38768/514fa59ad0e7951c3919ff92bbcd419a/data/pdf-pflegereport-2008.pdf (accessed on 28 June 2020).
- Thibault, L.; Kergoat, H. Eye care services for older institutionalised individuals affected by cognitive and visual deficits: A systematic review. Ophthalmic Physiol. Opt. 2016, 36, 566–583. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.M.F.; Ng, Y.T.Y.; Leung, W.K. Oral Health and Its Associated Factors Among Older Institutionalized Residents—A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4132. [Google Scholar] [CrossRef] [PubMed]
- Watson, R.A.; Suchak, N.; Steel, K. A Doctor in the House: Rationale for Providing On-site Urological Consultation to Geriatric Patients in Nursing Health Care Facilities. Urology 2010, 76, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Lemoyne, S.E.; Herbots, H.H.; Blick, D.; de Remmen, R.; Monsieurs, K.G.; van Bogaert, P. Appropriateness of transferring nursing home residents to emergency departments: A systematic review. BMC Geriatr. 2019, 19, 17. [Google Scholar] [CrossRef] [PubMed]
- Czwikla, J.; Schulz, M.; Heinze, F.; Kalwitzki, T.; Gand, D.; Schmidt, A.; Tsiasioti, C.; Schwinger, A.; Kloep, S.; Schmiemann, G.; et al. Needs-based provision of medical care to nursing home residents: Protocol for a mixed-methods study. BMJ Open 2019, 9, e025614. [Google Scholar] [CrossRef] [PubMed]
- Ågotnes, G.; McGregor, M.J.; Lexchin, J.; Doupe, M.B.; Müller, B.; Harrington, C. An International Mapping of Medical Care in Nursing Homes. Health Serv. Insights 2019, 12, 1178632918825083. [Google Scholar] [CrossRef] [PubMed]
- Hallauer, J.; Bienstein, C.; Lehr, U.; Rönsch, H. SÄVIP-Studie zur Arztlichen Versorgung in Pflegeheimen; Vincentz Network Marketing Service: Hannover, Germany, 2005. [Google Scholar]
- Unwin, B.K.; Porvaznik, M.; Spoelhof, G.D. Nursing home care: Part II. Clinical aspects. Am. Fam. Physician 2010, 81, 1229–1237. [Google Scholar] [PubMed]
- Flum, E.; Maagaard, R.; Godycki-Cwirko, M.; Scarborough, N.; Scherpbier, N.; Ledig, T.; Roos, M.; Steinhäuser, J. Assessing family medicine trainees—What can we learn from the European neighbours? GMS Z. Med. Ausbild. 2015, 32. [Google Scholar] [CrossRef]
- Ärztekammer Niedersachsen. Weiterbildungsordnung der Ärztekammer Niedersachsen. 2018. Available online: https://www.aekn.de/fileadmin/media/Downloadcenter/Weiterbildung/WBO_und_Richtlinien/WBO_01_06_2018.pdf (accessed on 28 June 2020).
- KBV. Regelung der Kassenärztlichen Bundesvereinigung zur Fortbildungsverpflichtung der Vertragsärzte und Vertragspsychotherapeuten nach § 95d SGB V. 2016. Available online: https://www.kbv.de/media/sp/Fortbildungsregelung_der_KBV.pdf (accessed on 28 June 2020).
- Ryskina, K.L.; Lam, C.; Jung, H.-Y. Association Between Clinician Specialization in Nursing Home Care and Nursing Home Clinical Quality Scores. J. Am. Med. Dir. Assoc. 2019, 20, 1007–1012. [Google Scholar] [CrossRef]
- Harrison, J.K.; McKay, I.K.; Grant, P.; Hannah, J.; Quinn, T.J. Appropriateness of unscheduled hospital admissions from care homes. Clin. Med. 2016, 16, 103–108. [Google Scholar] [CrossRef]
- Edwards, P.; Roberts, I.; Clarke, M.J.; Di Guiseppi, C.; Wentz, R.; Kwan, I.; Cooper, R.; Felix, L.M.; Pratap, S. Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Allers, K.; Fassmer, A.M.; Spreckelsen, O.; Hoffmann, F. End-of-life care of nursing home residents: A survey among general practitioners in northwestern Germany. Geriatr. Gerontol. Int. 2019. [Google Scholar] [CrossRef]
- Auer, S.R.; Höfler, M.; Linsmayer, E.; Beránková, A.; Prischl, D.; Ratajczak, P.; Steffl, M.; Holmerová, I. Cross-sectional study of prevalence of dementia, behavioural symptoms, mobility, pain and other health parameters in nursing homes in Austria and the Czech Republic: Results from the DEMDATA project. BMC Geriatr. 2018, 18, 178. [Google Scholar] [CrossRef] [PubMed]
- Atramont, A.; Bourdel-Marchasson, I.; Bonnet-Zamponi, D.; Tangre, I.; Fagot-Campagna, A.; Tuppin, P. Impact of nursing home admission on health care use and disease status elderly dependent people one year before and one year after skilled nursing home admission based on 2012-2013 SNIIRAM data. BMC Health Serv. Res. 2017, 17, 667. [Google Scholar] [CrossRef] [PubMed]
- Kutschar, P.; Lex, K.; Osterbrink, J.; Lorenzl, S. Parkinson’s disease, Alzheimer’s disease and oncological diseases in residential geriatric care: Pain frequency and selected healthcare features in comparison. Der Schmerz 2018, 32, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Hessmann, P.; Dodel, R.; Baum, E.; Müller, M.J.; Paschke, G.; Kis, B.; Zeidler, J.; Klora, M.; Reese, J.-P.; Balzer-Geldsetzer, M. Antipsychotic treatment of community-dwelling and institutionalised patients with dementia in Germany. Int. J. Psychiatry Clin. Pract. 2017, 22, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Schüssler, S.; Dassen, T.; Lohrmann, C. Care dependency and nursing care problems in nursing home residents with and without dementia: A cross-sectional study. Aging Clin. Exp. Res. 2016, 28, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Vlachova, M.; Richter, T.; Finne-Soveri, H.; Gindin, J.; Van Der Roest, H.; Denkinger, M.D.; Bernabei, R.; Onder, G.; Topinková, E. Prevalence and Correlates of Hearing and Visual Impairments in European Nursing Homes: Results From the SHELTER Study. J. Am. Med. Dir. Assoc. 2014, 15, 738–743. [Google Scholar] [CrossRef]
- Grimsmo, A.; Løhre, A.; Røsstad, T.; Gjerde, I.; Heiberg, I.H.; Steinsbekk, A. Disease-specific clinical pathways—Are they feasible in primary care? A mixed-methods study. Scand. J. Prim. Health Care 2018, 36, 152–160. [Google Scholar] [CrossRef]
- Dörks, M.; Herget-Rosenthal, S.; Schmiemann, G.; Hoffmann, F. Polypharmacy and Renal Failure in Nursing Home Residents: Results of the Inappropriate Medication in Patients with Renal Insufficiency in Nursing Homes (IMREN) Study. Drugs Aging 2016, 33, 45–51. [Google Scholar] [CrossRef]
- Conroy, S.; van der Cammen, T.; Schols, J.; van Balen, R.; Peteroff, P.; Luxton, T. Medical services for older people in nursing homes—Comparing services in England and the Netherlands. J. Nutr. Health Aging 2009, 13, 559–563. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | |
|---|---|
| Age in years (n = 371) * | |
| Mean (±SD) Median (Interquartile range) | 54.4 (±9.3) 54 (48–61) |
| Sex (n = 373) * | |
| Male | 57.6% |
| Female | 42.4% |
| Years as general practitioner (n = 373) * | |
| Mean (±SD) Median (Interquartile range) | 18.0 (±10.8) 18 (9–25) |
| Practice type (n = 373) * | |
| Single practice | 33.0% |
| Group practice/Medical care center | 67.0% |
| Practice location (n = 373) * | |
| Rural (≤20,000 inhabitants) | 52.3% |
| Semi-urban (>20,000 to ≤100,000 inhabitants) | 25.2% |
| Urban (>100,000 inhabitants) | 22.5% |
| Number of nursing homes visited (n =3 73) * | |
| Mean (±SD) Median (Interquartile range) | 4.1 (±2.2) 4 (3–5) |
| Number of residents cared for (n = 367) * | |
| Mean (±SD) Median (Interquartile range) | 46.8 (±43.5) 30 (20–60) |
| Trained in palliative care (n = 375) Trained in geriatric medicine (n = 375) | 24.3% 4.8% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spreckelsen, O.; Schmiemann, G.; Fassmer, A.M.; Engel, B.; Hoffmann, F.; Freitag, M.H. How Do German General Practitioners Assess Medical Specialist Care Needs of Nursing Home Residents? Results of a Postal Survey in North-Western Germany. Int. J. Environ. Res. Public Health 2020, 17, 7126. https://doi.org/10.3390/ijerph17197126
Spreckelsen O, Schmiemann G, Fassmer AM, Engel B, Hoffmann F, Freitag MH. How Do German General Practitioners Assess Medical Specialist Care Needs of Nursing Home Residents? Results of a Postal Survey in North-Western Germany. International Journal of Environmental Research and Public Health. 2020; 17(19):7126. https://doi.org/10.3390/ijerph17197126
Chicago/Turabian StyleSpreckelsen, Ove, Guido Schmiemann, Alexander Maximilian Fassmer, Bettina Engel, Falk Hoffmann, and Michael Hermann Freitag. 2020. "How Do German General Practitioners Assess Medical Specialist Care Needs of Nursing Home Residents? Results of a Postal Survey in North-Western Germany" International Journal of Environmental Research and Public Health 17, no. 19: 7126. https://doi.org/10.3390/ijerph17197126
APA StyleSpreckelsen, O., Schmiemann, G., Fassmer, A. M., Engel, B., Hoffmann, F., & Freitag, M. H. (2020). How Do German General Practitioners Assess Medical Specialist Care Needs of Nursing Home Residents? Results of a Postal Survey in North-Western Germany. International Journal of Environmental Research and Public Health, 17(19), 7126. https://doi.org/10.3390/ijerph17197126