Reorienting Nurturing Care for Early Childhood Development during the COVID-19 Pandemic in Kenya: A Review

 , , , , , , and
, , , , , , and 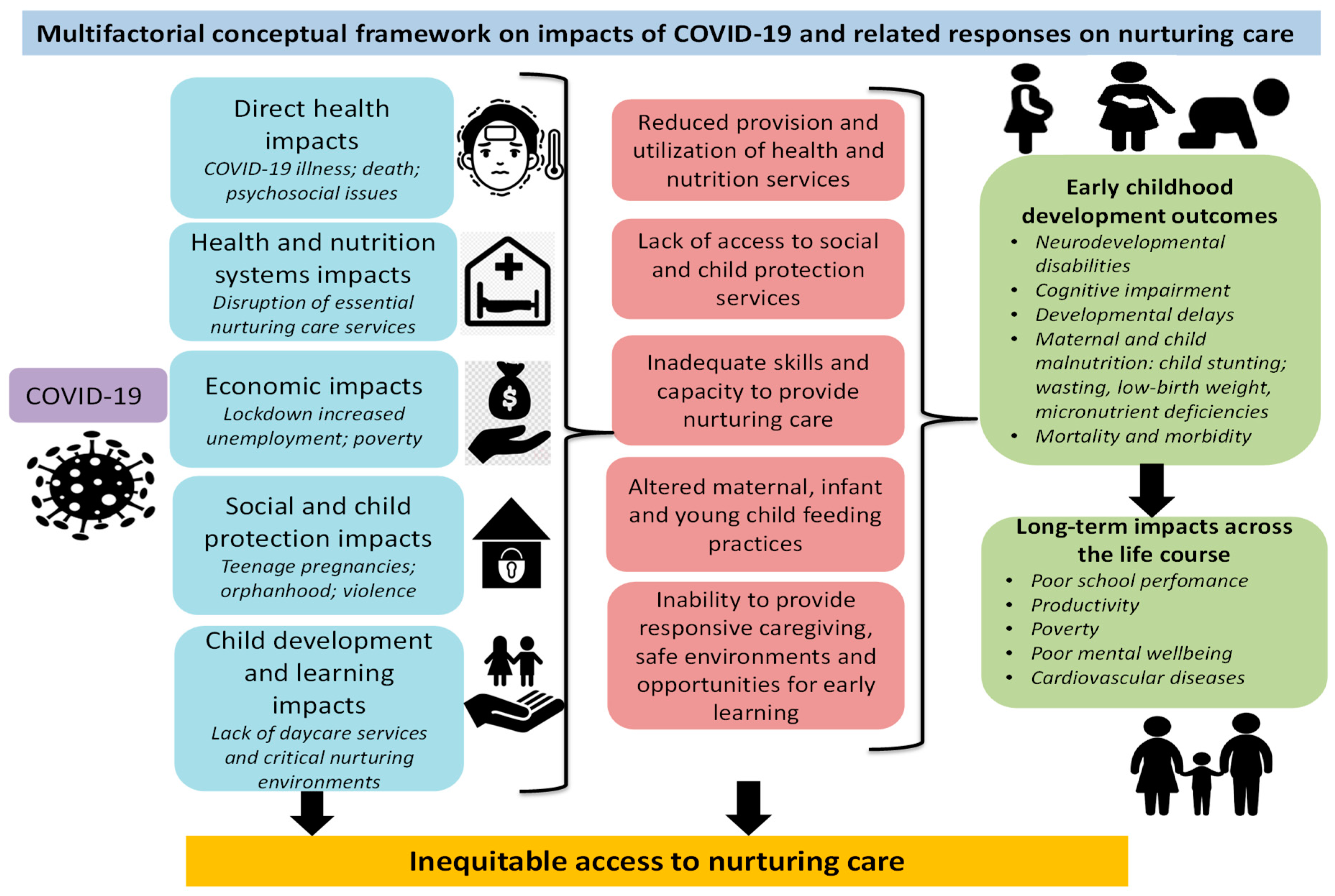{kind=link}
Abstract
1. Introduction
2. Nurturing Care Framework (NCF)
3. Kenyan Context
4. Evidence from Previous Pandemics
5. Impacts of COVID-19 on Nurturing Care
5.1. Conceptual Framework of the Impacts of COVID-19 and Control Measures on Nurturing Care
5.2. Direct Health Impacts of COVID-19
5.2.1. Impacts on Children’s Health
5.2.2. Psychosocial Impacts on Caregivers and Children
5.3. Indirect Health Impacts
Impact on Health and Nutrition Systems
5.4. Economic Impacts
Losses in Income and Increased Poverty Levels
5.5. Social and Child Protection Impacts
5.5.1. Increase in Abuse, Neglect, and Violence
5.5.2. Orphanhood
5.5.3. Teenage Pregnancies in the Pandemic and the Implications for Nurturing Care
5.6. Child Development and Learning Impacts
6. Policy and Program Strategies to Reorient Nurturing Care
6.1. Direct Health and Health and Nutrition System Support
6.2. Economic Support
6.3. Social and Child Protection Support
6.4. Child Development and Learning Support
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ministry of Health. First Case of Coronavirus Disease Confirmed in Kenya; Ministry of Health: Nairobi, Kenya, 2020. Available online: https://www.health.go.ke/wp-content/uploads/2020/03/Statement-on-Confirmed-COVID-19-Case-13-March-2020-final-1.pdf (accessed on 5 July 2020).
- Parliament of Kenya. The COVID 19 Global Pandemic: Impact to the Economy and Policy Options. Special Bulletin No. 1/2020. Available online: http://parliament.go.ke/sites/default/files/2020-04/Special%20Bulletin%20Covid%2019%202.4.2020%20final.pdf (accessed on 3 August 2020).
- World Health Organization. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cusick, S.E.; Georgieff, M.K. The role of nutrition in brain development: The golden opportunity of the “first 1000 days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef]
- World Bank. Poverty Incidence in Kenya Declined Significantly, but Unlikely to Be Eradicated by 2030. Available online: https://www.worldbank.org/en/country/kenya/publication/kenya-economic-update-poverty-incidence-in-kenya-declined-significantly-but-unlikely-to-be-eradicated-by-2030 (accessed on 7 July 2020).
- UN-Habitat. Slum Almanac 2015–2016: Tracking Improvement in the Lives of Slum Dwellers; UN Habitat: Nairobi, Kenya, 2016; Available online: https://unhabitat.org/slum-almanac-2015-2016 (accessed on 10 July 2020).
- De Vita, M.V.; Scolfaro, C.; Santini, B.; Lezo, A.; Gobbi, F.; Buonfrate, D.; Kimani-Murage, E.W.; Macharia, T.; Wanjohi, M.; Rovarini, J.M. Malnutrition, morbidity and infection in the informal settlements of Nairobi, Kenya: An epidemiological study. Ital. J. Pediatr. 2019, 45, 12. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and National AIDS Control Council. Kenya HIV Estimates Report 2018; Ministry of Health and National AIDS Control Council: Nairobi, Kenya, 2020; Available online: https://nacc.or.ke/wp-content/uploads/2018/11/HIV-estimates-report-Kenya-20182.pdf (accessed on 9 July 2020).
- Fisher, P.; Lombardi, J.; Kendall-Taylor, N. Why Households with Young Children Warrant Our Attention and Support during (and after) the COVID-19 Pandemic. Rapid-EC Project. Available online: https://medium.com/rapid-ec-project/why-households-with-young-children-warrant-our-attention-and-support-during-and-after-the-b7cee9b76184 (accessed on 9 July 2020).
- Yoshikawa, H.; Wuermli, A.J.; Britto, P.R.; Dreyer, B.; Leckman, J.F.; Lye, S.J.; Ponguta, L.A.; Richter, L.M.; Stein, A. Effects of the global COVID-19 pandemic on early childhood development: Short-and long-term risks and mitigating program and policy actions. J. Pediatr. 2020, 223, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- United Nations Development Program. Socio-Economic Impact of COVID-19 in Kenya. 2020. Available online: https://www.undp.org/content/dam/rba/docs/COVID-19-CO-Response/Socio-Economic-Impact-COVID-19-Kenya-Policy-Brief-UNDP-Kenya-April-2020.pdf (accessed on 23 July 2020).
- Kelly, E. The scourge of asian flu in utero exposure to pandemic influenza and the development of a cohort of british children. J. Hum. Resour. 2011, 46, 669–694. [Google Scholar] [CrossRef]
- Richter, A.; Robling, P.O. Multigenerational Effects of the 1918-19 Influenza Pandemic in Sweden; Swedish Institute for Social Research: Stockholm, Sweden, 2013; Volume 5. [Google Scholar]
- Ogasawara, K. Persistence of pandemic influenza on the development of children: Evidence from industrializing Japan. Soc. Sci. Med. 2017, 181, 43–53. [Google Scholar] [CrossRef]
- Borren, I.; Tambs, K.; Gustavson, K.; Schjølberg, S.; Eriksen, W.; Håberg, S.E.; Hungnes, O.; Mjaaland, S.; Trogstad, L.I. Early prenatal exposure to pandemic influenza A (H1N1) infection and child psychomotor development at 6 months–A population-based cohort study. Early Hum. Dev. 2018, 122, 1–7. [Google Scholar] [CrossRef]
- Almond, D. Is the 1918 influenza pandemic over? Long-term effects of in utero influenza exposure in the post-1940 US population. J. Political Econ. 2006, 114, 672–712. [Google Scholar] [CrossRef]
- Nelson, R.E. Testing the fetal origins hypothesis in a developing country: Evidence from the 1918 influenza pandemic. Health Econ. 2010, 19, 1181–1192. [Google Scholar] [CrossRef]
- Neelsen, S.; Stratmann, T. Long-run effects of fetal influenza exposure: Evidence from Switzerland. Soc. Sci. Med. 2012, 74, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-J.; Liu, E.M. Does in utero exposure to illness matter? The 1918 influenza epidemic in Taiwan as a natural experiment. J. Health Econ. 2014, 37, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, A.; van der Linden, V.; Yeargin-Allsopp, M.; Carvalho, M.D.C.G.; Ribeiro, E.M.; Braun, K.V.N.; Durkin, M.S.; Pastula, D.M.; Moore, J.T.; Moore, C.A. Motor abnormalities and epilepsy in infants and children with evidence of congenital Zika virus infection. Pediatrics 2018, 141, S167–S179. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.; Antle, B.J.; Berlin, D.; Granger, M.; Meighan, K.; Neilson, B.J.; Shama, W.; Westland, J.; Kaufman, M. Wearing masks in a pediatric hospital: Developing practical guidelines. Can. J. Public Health Revue Canadienne Sante Publique 2004, 95, 256. [Google Scholar] [CrossRef] [PubMed]
- Knox, J.; Arpadi, S.M.; Kauchali, S.; Craib, M.; Kvalsvig, J.D.; Taylor, M.; Bah, F.; Mellins, C.; Davidson, L.L. Screening for developmental disabilities in HIV positive and HIV negative children in South Africa: Results from the Asenze Study. PLoS ONE 2018, 13, e0199860. [Google Scholar] [CrossRef]
- Sherr, L.; Croome, N.; Castaneda, K.P.; Bradshaw, K.; Romero, R.H. Developmental challenges in HIV infected children—An updated systematic review. Child. Youth Serv. Rev. 2014, 45, 74–89. [Google Scholar] [CrossRef]
- Elizabeth Glaser Pediatric AIDS and Hilton Foundation. HIV and Early Childhood Development. ECD Brief January 2019. Available online: https://www.pedaids.org/wp-content/uploads/2019/01/ECD-Brief-Jan.2019.pdf (accessed on 11 July 2020).
- Abubakar, A. Risk factors for Sub-Optimal Child Development 2018 PowerPoint Presentation. Available online: http://www.kenyapaediatric.org/wp-content/uploads/2018/05/Risk-factors-for-Sub-Optimal-Child-Development-Dr.-Amina-Abubakar.pdf (accessed on 23 July 2020).
- Slogrove, A.L.; Becquet, R.; Chadwick, E.G.; Côté, H.C.; Essajee, S.; Hazra, R.; Leroy, V.; Mahy, M.; Murenga, M.; Wambui Mwangi, J. Surviving and thriving—Shifting the public health response to HIV-exposed uninfected children: Report of the 3rd HIV-exposed uninfected child workshop. Front. Pediatr. 2018, 6, 157. [Google Scholar] [CrossRef]
- Braun, R.; Catalani, C.; Wimbush, J.; Israelski, D. Community health workers and mobile technology: A systematic review of the literature. PLoS ONE 2013, 8, e65772. [Google Scholar] [CrossRef]
- Shah, S. Early Childhood Development in Humanitarian Crises: South Sudanese Refugees in Uganda; Routledge: London, UK, 2019. [Google Scholar]
- Karimi-Zarchi, M.; Neamatzadeh, H.; Dastgheib, S.A.; Abbasi, H.; Mirjalili, S.R.; Behforouz, A.; Ferdosian, F.; Bahrami, R. Vertical Transmission of Coronavirus Disease 19 (COVID-19) from Infected Pregnant Mothers to Neonates: A Review. Fetal Pediatr. Pathol. 2020, 39, 246–250. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef]
- Rasmussen, S.A.; Smulian, J.C.; Lednicky, J.A.; Wen, T.S.; Jamieson, D.J. Coronavirus Disease 2019 (COVID-19) and Pregnancy: What obstetricians need to know. Am. J. Obstet. Gynecol. 2020, 222, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Dineshwori, L. First Mother-Baby COVID-19 Vertical Transmission Recorded in India. Available online: https://www.firstpost.com/health/covid-19-in-pregnancy-indias-first-case-of-vertical-coronavirus-transmission-from-mother-to-child-documented-in-pune-hospital-8648071.html (accessed on 1 August 2020).
- Zimmermann, P.; Curtis, N. Coronavirus Infections in Children Including COVID-19: An Overview of the Epidemiology, Clinical Features, Diagnosis, Treatment and Prevention Options in Children. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 among children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed]
- Livingston, E.; Bucher, K. Coronavirus Disease 2019 (COVID-19) in Italy. JAMA 2020, 323, 1335. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Whittaker, E. Kawasaki-like disease: Emerging complication during the COVID-19 pandemic. Lancet 2020, 395, 1741–1743. [Google Scholar] [CrossRef]
- Centers for Disease Control. Coronavirus Disease 2019 in Children—United States, February 12–April 2, 2020; CDC: Antlanta, GA, USA, 2020. [CrossRef]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Ministry of Health. Daily Situation Report-132; Ministry of Health: Nairobi, Kenya, 2020.
- Save the Children. Save the Children’s Global Response Plan to COVID-19: Protecting a Generation of Children; Save the Children: London, UK, 2020; Available online: https://resourcecentre.savethechildren.net/library/save-childrens-global-response-plan-covid-19-protecting-generation-children (accessed on 8 July 2020).
- Mwiti, G. Mental strain from coronavirus might weaken national cohesion. Daily Nation 2020. Available online: https://www.nation.co.ke/kenya/blogs-opinion/opinion/mental-strain-coronavirus-weaken-national-cohesion-549222 (accessed on 5 July 2020).
- Shonkoff, J.P.; Garner, A.S. Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef]
- Ministry of Health. A Comprehensive Guide on Mental Health and Psychosocial Support during the COVID-19 Pandemic; Ministry of Health: Nairobi, Kenya, 2020. Available online: http://cities-rise.org/wp/wp-content/uploads/2020/05/Final-Comprehensive-Guide-on-Mental-Health-and-Psychosocial-Support-For-COVID-19-Pandemic-4.pdf (accessed on 3 August 2020).
- Smile, S.C. Supporting children with autism spectrum disorder in the face of the COVID-19 pandemic. CMAJ 2020, 192, E587. [Google Scholar] [CrossRef]
- World Health Organization. Policy Brief on Covid Impact on Children; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/mca-documents/mca-covid/policy-brief-on-covid-impact-on-children-16-april-2020.pdf?sfvrsn=d349ea27_2&ua=1 (accessed on 12 July 2020).
- African Union. The Abuja Declaration; African Union: Addis Ababa, Ethiopia, 2001; Available online: https://au.int/sites/default/files/pages/32894-file-2001-abuja-declaration.pdf (accessed on 6 July 2020).
- Levine, T.A.; Grunau, R.E.; McAuliffe, F.M.; Pinnamaneni, R.; Foran, A.; Alderdice, F.A. Early childhood neurodevelopment after intrauterine growth restriction: A systematic review. Pediatrics 2015, 135, 126–141. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Allison, B.J.; Castillo-Melendez, M.; Jenkin, G.; Polglase, G.R.; Miller, S.L. Neonatal morbidities of fetal growth restriction: Pathophysiology and impact. Front. Endocrinol. 2019, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef]
- Chepngetich, J.; Keraka, M.; Njagi, J. Assessment of the knowledge on pre conception care among women of reproductive age in Ruiru sub-county, Kiambu county, Kenya. Glob. J. Health Sci. 2018, 3, 82–100. [Google Scholar]
- Bosire, N. Pre-Conception Care Is Crucial for Every Woman Who Plans to Get Pregnant: Over 95 per cent of Women in Kenya Get Pregnant without the Benefit of This Service, due to Ignorance. Daily Nation. 1 May 2017. Available online: https://www.nation.co.ke/kenya/healthy-nation/pre-conception-care-is-crucial-for-every-woman-who-plans-to-get-pregnant-392150 (accessed on 10 July 2020).
- Semaan, A.T.; Audet, C.; Huysmans, E.; Afolabi, B.B.; Assarag, B.; Banke-Thomas, A.; Blencowe, H.; Caluwaerts, S.; Campbell, O.M.; Cavallaro, F.L. Voices from the frontline: Findings from a thematic analysis of a rapid online global survey of maternal and newborn health professionals facing the COVID-19 pandemic. medRxiv 2020. [Google Scholar] [CrossRef]
- Abbas, K.M.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S. Benefit-risk analysis of health benefits of routine childhood immunisation against the excess risk of SARS-CoV-2 infections during the Covid-19 pandemic in Africa. medRxiv 2020. [Google Scholar] [CrossRef]
- United Nations Childrens Fund. Maternal and Newborn Health and COVID-19; United Nations Childrens Fund: New York, NY, USA, 2020; Available online: https://data.unicef.org/topic/maternal-health/covid-19/ (accessed on 27 July 2020).
- Akseer, N.; Kandru, G.; Keats, E.C.; Bhutta, Z.A. COVID-19 pandemic and mitigation strategies: Implications for maternal and child health and nutrition. Am. J. Clin. Nutr. 2020, 112, 251–256. [Google Scholar] [CrossRef]
- World Health Organization. Essential Nutrition Actions: Mainstreaming Nutrition through the Life-Course; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications/i/item/9789241515856 (accessed on 9 July 2020).
- Obonyo, N. How COVID-19 pandemic has affected the healthcare system in Kenya. The Standard. 29 April 2020. Available online: https://www.standardmedia.co.ke/article/2001369644/how-covid-19-pandemic-has-affected-the-healthcare-system-in-kenya (accessed on 15 July 2020).
- Sochas, L.; Channon, A.A.; Nam, S. Counting indirect crisis-related deaths in the context of a low-resilience health system: The case of maternal and neonatal health during the Ebola epidemic in Sierra Leone. Health Policy Plan. 2017, 32, iii32–iii39. [Google Scholar] [CrossRef]
- Streifel, C. How Did Ebola Impact Maternal and Child Health in Liberia and Sierra Leone; A Report of the CSIS Global Health Policy Center; Center for Strategic & International Studies: Washington, DC, USA, 2015. [Google Scholar]
- Masresha, B.G.; Luce, R., Jr.; Weldegebriel, G.; Katsande, R.; Gasasira, A.; Mihigo, R. The impact of a prolonged ebola outbreak on measles elimination activities in Guinea, Liberia and Sierra Leone, 2014–2015. Pan Afr. Med. J. 2020, 35 (Suppl. S1), 8. [Google Scholar] [CrossRef]
- United Nations. Policy Brief: The Impact of COVID-19 on Children; United Nations: New York, NY, USA, 2020; Available online: https://unsdg.un.org/sites/default/files/2020-04/160420_Covid_Children_Policy_Brief.pdf (accessed on 14 July 2020).
- Corburn, J.; Vlahov, D.; Mberu, B.; Riley, L.; Caiaffa, W.T.; Rashid, S.F.; Ko, A.; Patel, S.; Jukur, S.; Martínez-Herrera, E. Slum health: Arresting COVID-19 and improving well-being in urban informal settlements. J. Urban Health 2020, 97, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Development Initiatives. Socioeconomic Impacts of Covid-19 in Kenya. Background Paper; Development Initiatives: Bristol, UK, 2020; Available online: https://devinit.org/resources/socioeconomic-impacts-covid-19-kenya/ (accessed on 22 July 2020).
- Akim, A.-M.; Ayivodji, F. Interaction Effect of Lockdown with Economic and Fiscal Measures against COVID-19 on Social-Distancing Compliance: Evidence from Africa. SSRN 2020. [Google Scholar] [CrossRef]
- Wafula, P. Over one million rendered jobless in Kenya as Covid-19 takes toll on businesses. East African. 5 June 2020. Available online: https://www.theeastafrican.co.ke/tea/business/over-one-million-rendered-jobless-in-kenya-as-covid-19-takes-toll-on-businesses-1442672 (accessed on 17 July 2020).
- Kenya National Bureau of Statistics. Survey on Socio Economic Impact of COVID-19 on Households Report; Kenya National Bureau of Statistics: Nairobi, Kenya, 2020; Available online: https://t.co/zRheAaYKwi?amp (accessed on 24 July 2020).
- Austrian, K.; Pinchoff, J.; Tidwell, J.B.; White, C.; Abuya, T.; Kangwana, B.; Ochako, R.; Wanyungu, J.; Muluve, E.; Mbushi, F. COVID-19 related knowledge, attitudes, practices and needs of households in informal settlements in Nairobi, Kenya. Bull. World Health Organ. 2020. [Google Scholar] [CrossRef]
- Senghore, M.; Savi, M.K.; Gnangnon, B.; Hanage, W.P.; Okeke, I.N. Leveraging Africa’s preparedness towards the next phase of the COVID-19 pandemic. Lancet Glob. Health 2020. [Google Scholar] [CrossRef]
- Ooko, S. Protecting Children from Abuse during the COVID-19 Pandemic. Available online: https://www.wvi.org/stories/coronavirus-health-crisis/protecting-children-abuse-during-covid-19-pandemic (accessed on 10 July 2020).
- Bhalla, N. Kenya Orders Probe into Rise in Violence against Women and Girls during Pandemic; Reuters: Nairobi, Kenya, 2020. [Google Scholar]
- Odhiambo, A. Tackling Kenya’s Domestic Violence amid COVID-19 Crisis: Lockdown Measures Increase Risks for Women and Girls; Human Rights Wach: New York, NY, USA, 2020; Available online: https://www.hrw.org/news/2020/04/08/tackling-kenyas-domestic-violence-amid-covid-19-crisis (accessed on 19 July 2020).
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.-Y.; Nair, M.; Halpern, R.; Kuper, H.; Breinbauer, C.; De Vries, P.J.; Gladstone, M. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef]
- Berkes, J.; Raikes, A.; Bouguen, A.; Filmer, D. Joint roles of parenting and nutritional status for child development: Evidence from rural Cambodia. Dev. Sci. 2019, 22, e12874. [Google Scholar] [CrossRef]
- Scherer, E.; Hagaman, A.; Chung, E.; Rahman, A.; O’Donnell, K.; Maselko, J. The relationship between responsive caregiving and child outcomes: Evidence from direct observations of mother-child dyads in Pakistan. BMC Public Health 2019, 19, 252. [Google Scholar] [CrossRef]
- Mackes, N.K.; Golm, D.; Sarkar, S.; Kumsta, R.; Rutter, M.; Fairchild, G.; Mehta, M.A.; Sonuga-Barke, E.J. Early childhood deprivation is associated with alterations in adult brain structure despite subsequent environmental enrichment. Proc. Natl. Acad. Sci. USA 2020, 117, 641–649. [Google Scholar] [CrossRef]
- Butler, A.S.; Panzer, A.M.; Goldfrank, L.R. Understanding the Psychological Consequences of Traumatic Events, Disasters, and Terrorism. In Preparing for the Psychological Consequences of Terrorism: A Public Health Strategy; National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- Sloth-Nielsen, J. Kenya Takes Next Steps to Replace Children’s Homes with Family Care; The Conversation: Nairobi, Kenya, 2019. [Google Scholar]
- Kassa, G.M.; Arowojolu, A.; Odukogbe, A.; Yalew, A.W. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and meta-analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef]
- Kenya National Bureau of Statistics. Kenya Demographic and Health Survey 2014; Kenya National Bureau of Statistics: Nairobi, Kenya, 2015. [Google Scholar]
- Ajayi, A.; Mwoka, M. The Potential Impact of COVID-19 on Teenage Pregnancy in Kenya. Available online: https://aphrc.org/blogarticle/the-potential-impacts-of-covid-19-on-teenage-pregnancy-in-kenya/ (accessed on 29 July 2020).
- Moraa, O. Sex for sanitary towels, food: Covid-19 pushing girls to engage in transactional sex. Daily Nation. 2 June 2020. Available online: https://www.nation.co.ke/kenya/gender/sex-for-sanitary-towels-food-487232 (accessed on 13 July 2020).
- Mulvihill, N. The Impact of COVID-19 on Sex Workers. Available online: https://blogs.lse.ac.uk/covid19/2020/06/08/the-impact-of-covid-19-on-sex-workers/ (accessed on 18 July 2020).
- Waweru, M. Schoolgirls’ Access to Sanitary Pads Compromised during COVID-19. Available online: https://www.capitalfm.co.ke/news/2020/04/schoolgirls-access-to-sanitary-pads-compromised-during-covid-19/ (accessed on 19 July 2020).
- World Health Organization. Adolescent Pregnancy; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/en/news-room/fact-sheets/detail/adolescent-pregnancy (accessed on 23 July 2020).
- Neal, S.; Matthews, Z.; Frost, M.; Fogstad, H.; Camacho, A.V.; Laski, L. Childbearing in adolescents aged 12–15 years in low resource countries: A neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstet. Gynecol. Scand. 2012, 91, 1114–1118. [Google Scholar] [CrossRef] [PubMed]
- Mayrhofer, B. Teenage Pregnancy: Right to Childhood; Development and Cooperation: Frankfurt am Main, Germany, 2013; Available online: https://www.dandc.eu/en/article/long-term-impacts-teenage-pregnancies-girls-and-society (accessed on 12 July 2020).
- Yakubu, I.; Salisu, W.J. Determinants of adolescent pregnancy in sub-Saharan Africa: A systematic review. Reprod. Health 2018, 15, 15. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Dubey, M.J.; Chatterjee, S.; Dubey, S. Impact of COVID-19 on children: Special focus on psychosocial aspect. Minerva Pediatr. 2020, 72. [Google Scholar] [CrossRef]
- Kobuthi-Kuria, J. Domestic Violence: The Shadow Pandemic. Available online: https://www.amnestykenya.org/domestic-violence-the-shadow-pandemic/ (accessed on 28 July 2020).
- Hofferth, S.L. Risking the Future: Adolescent Sexuality, Pregnancy, and Childbearing; National Academies Press: Washington, DC, USA, 1987; Volume 1. [Google Scholar]
- Shaw, M.; Lawlor, D.A.; Najman, J.M. Teenage children of teenage mothers: Psychological, behavioural and health outcomes from an Australian prospective longitudinal study. Soc. Sci. Med. 2006, 62, 2526–2539. [Google Scholar] [CrossRef]
- Wanzala, O. CS Magoha cancels KCPE, KCSE exams as Covid-19 bites. Daily Nation. 7 July 2020. Available online: https://www.nation.co.ke/kenya/news/education/cs-magoha-cancels-kcpe-kcse-exams-as-covid-19-bites-1446342 (accessed on 9 July 2020).
- Fatinato, D. We must mitigate teenage pregnancy crisis amidst Covid-19. Star. 13 June 2020. Available online: https://www.the-star.co.ke/siasa/2020-06-13-we-must-mitigate-teenage-pregnancy-crisis-amidst-covid-19/ (accessed on 9 July 2020).
- UNESCO; UNICEF; WFP; World Bank Group. Framework for Reopening Schools; UNICEF: New York, NY, USA, 2020; Available online: https://www.unicef.org/sites/default/files/2020-06/Framework-for-reopening-schools-2020.pdf (accessed on 27 July 2020).
- Caddy, E. There Are at Least 2700 Informal Child Daycares in Nairobi-Tiny Totos Is Working to Help Them Upgrade Their Services. Available online: https://theirworld.org/voices/tiny-totos-kenya-helping-informal-daycares-in-nairobi-upgrade-services (accessed on 10 August 2020).
- Ministry of Education. National Pre-Primary Education Policy; Ministry of Education: Nairobi, Kenya, 2017; Available online: https://www.education.go.ke/index.php/downloads/file/545-national-pre-primary-education-policy (accessed on 9 July 2020).
- Britton, J.R. The assessment of satisfaction with care in the perinatal period. J. Psychosom. Obstet. Gynecol. 2012, 33, 37–44. [Google Scholar] [CrossRef]
- Attipoe-Dorcoo, S.; Delgado, R.; Gupta, A.; Bennet, J.; Oriol, N.E.; Jain, S.H. Mobile health clinic model in the COVID-19 pandemic: Lessons learned and opportunities for policy changes and innovation. Int. J. Equity Health 2020, 19, 1–5. [Google Scholar] [CrossRef]
- Mboye, P. Health Educator Uses a Mobile Van to Educate Communities about COVID-19; UNICEF: New York, NY, USA, 2020; Available online: https://www.unicef.org/uganda/stories/health-educator-uses-mobile-van-educate-communities-about-covid-19 (accessed on 9 July 2020).
- Hughes, R.; Wasunna, B.; Omedo, D.; Rashid, N. mThrive: A nurturing care app that supports community health workers. Early Chilhood Matters 2019. [Google Scholar]
- Cooper, J.E.; Benmarhnia, T.; Koski, A.; King, N.B. Cash transfer programs have differential effects on health: A review of the literature from low and middle-income countries. Soc. Sci. Med. 2020, 247, 112806. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Moore, C.M. The Cash Dividend: The Rise of Cash Transfer Programs in Sub-Saharan Africa; The World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Bliss, J.; Golden, K.; Bourahla, L.; Stoltzfus, R.; Pelletier, D. An emergency cash transfer program promotes weight gain and reduces acute malnutrition risk among children 6-24 months old during a food crisis in Niger. J. Glob. Health 2018, 8, 010410. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.A. Romania’s Abandoned Children; Harvard University Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Lucas, J.E.; Richter, L.M.; Daelmans, B. Care for Child Development: An intervention in support of responsive caregiving and early child development. Child Care Health Dev. 2018, 44, 41–49. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shumba, C.; Maina, R.; Mbuthia, G.; Kimani, R.; Mbugua, S.; Shah, S.; Abubakar, A.; Luchters, S.; Shaibu, S.; Ndirangu, E. Reorienting Nurturing Care for Early Childhood Development during the COVID-19 Pandemic in Kenya: A Review. Int. J. Environ. Res. Public Health 2020, 17, 7028. https://doi.org/10.3390/ijerph17197028
Shumba C, Maina R, Mbuthia G, Kimani R, Mbugua S, Shah S, Abubakar A, Luchters S, Shaibu S, Ndirangu E. Reorienting Nurturing Care for Early Childhood Development during the COVID-19 Pandemic in Kenya: A Review. International Journal of Environmental Research and Public Health. 2020; 17(19):7028. https://doi.org/10.3390/ijerph17197028
Chicago/Turabian StyleShumba, Constance, Rose Maina, Gladys Mbuthia, Rachel Kimani, Stella Mbugua, Sweta Shah, Amina Abubakar, Stanley Luchters, Sheila Shaibu, and Eunice Ndirangu. 2020. "Reorienting Nurturing Care for Early Childhood Development during the COVID-19 Pandemic in Kenya: A Review" International Journal of Environmental Research and Public Health 17, no. 19: 7028. https://doi.org/10.3390/ijerph17197028
APA StyleShumba, C., Maina, R., Mbuthia, G., Kimani, R., Mbugua, S., Shah, S., Abubakar, A., Luchters, S., Shaibu, S., & Ndirangu, E. (2020). Reorienting Nurturing Care for Early Childhood Development during the COVID-19 Pandemic in Kenya: A Review. International Journal of Environmental Research and Public Health, 17(19), 7028. https://doi.org/10.3390/ijerph17197028