Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior?

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Survey and Sample
2.3. Exploratory Nature of this Research
2.4. General Indicators of Problematic Hypersexuality
2.5. Sex Addiction Indicators
2.6. Hypersexual Disorder Indicators
2.7. Compulsive Sexual Behavior Disorder Indicator
2.8. Need for Help
2.9. Covariates
2.10. Statistical Analyses
3. Results
3.1. Characteristics of Participants
3.2. EFA Results
3.3. CFA Results
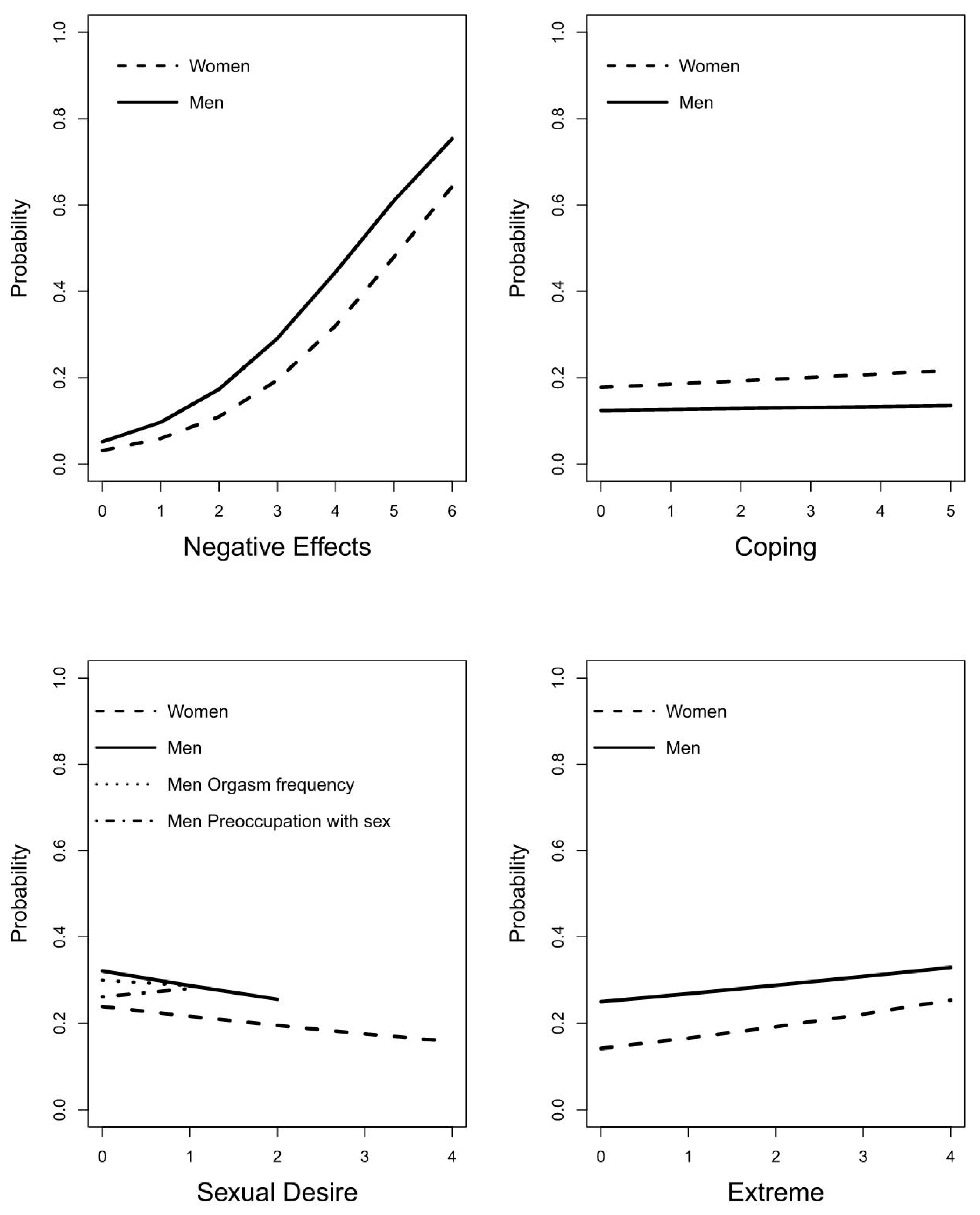
3.4. Logistic Regression Results
3.5. Measure of Severity of PH
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kingston, D.A.; Firestone, P. Problematic Hypersexuality: A review of conceptualization and diagnosis. Sex. Addict. Compulsivity 2008, 4, 284–310. [Google Scholar] [CrossRef]
- Kor, A.; Fogel, Y.; Reid, R.C.; Potenza, M.N. Should Hypersexual Disorder be classified as an addiction? Sex. Addict. Compulsivity 2013, 1–2. [Google Scholar] [CrossRef]
- Skegg, K.; Nada-Raja, S.; Dickson, N.; Paul, C. Perceived “Out of Control” sexual behavior in a cohort of young adults from the dunedin multidisciplinary health and development study. Arch. Sex. Behav. 2009, 4, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Levaque, E.; Sawatsky, M.L.; Lalumière, M.L. Hypersexualité chez les étudiants universitaires hétérosexuels. Can. J. Behav. Sci. 2016, 3, 182–192. [Google Scholar] [CrossRef]
- Kingston, D.A.; Walters, G.D.; Olver, M.E.; Levaque, E.; Sawatsky, M.; Lalumière, M.L. Understanding the latent structure of hypersexuality: A taxometric investigation. Arch. Sex. Behav. 2018, 8, 2207–2221. [Google Scholar] [CrossRef]
- Cashwell, C.S.; Giordano, A.L.; Lewis, T.F.; Wachtel, K.A.; Bartley, J.L. Using the PATHOS questionnaire for screening sexual addiction among college students: A preliminary exploration. Sex. Addict. Compulsivity 2015, 2, 154–166. [Google Scholar] [CrossRef]
- Steele, V.R.; Staley, C.; Fong, T.; Prause, N. Sexual desire, not hypersexuality, is related to neurophysiological responses elicited by sexual images. Socioaffect. Neurosci. Psychol. 2013, 1, 20770. [Google Scholar] [CrossRef]
- Levine, M.P.; Troiden, R.R. The myth of sexual compulsivity. J. Sex Res. 1988, 3, 347–363. [Google Scholar] [CrossRef]
- Ley, D.; Prause, N.; Finn, P. The emperor has no clothes: A review of the ‘pornography addiction’ model. Curr. Sex. Health Rep. 2014, 2, 94–105. [Google Scholar] [CrossRef]
- Moser, C. Hypersexual Disorder: Just more muddled thinking. Arch. Sex. Behav. 2010, 2, 227–229. [Google Scholar] [CrossRef]
- Reay, B.; Attwood, N.; Gooder, C. Inventing sex: The short history of sex addiction. Sex. Cult. 2012, 1, 1–19. [Google Scholar] [CrossRef]
- Derbyshire, K.L.; Grant, J.E. Compulsive sexual behavior: A review of the literature. J. Behav. Addict. 2015, 2, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Karila, L.; Wery, A.; Weinstein, A.; Cottencin, O.; Petit, A.; Reynaud, M.; Billieux, J. Sexual Addiction or Hypersexual Disorder: Different terms for the same problem? A review of the literature. Curr. Pharm. Des. 2014, 25, 4012–4020. [Google Scholar] [CrossRef]
- Montgomery-Graham, S. Conceptualization and assessment of Hypersexual Disorder: A systematic review of the literature. Sex. Med. Rev. 2017, 2, 146–162. [Google Scholar] [CrossRef]
- Moser, C. Hypersexual Disorder: Searching for clarity. Sex. Addict. Compulsivity 2013, 1–2, 48–58. [Google Scholar] [CrossRef]
- Levine, S.B. What is Sexual Addiction? J. Sex Marital Ther. 2010, 3, 261–275. [Google Scholar] [CrossRef]
- Cantor, J.M.; Klein, C.; Lykins, A.; Rullo, J.E.; Thaler, L.; Walling, B.R. A treatment-oriented typology of self-identified hypersexuality referrals. Arch. Sex. Behav. 2013, 5, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, J.; Kaldo, V.; Arver, S.; Dhejne, C.; Jokinen, J.; Öberg, K.G. A randomized controlled study of group-administered cognitive behavioral therapy for Hypersexual Disorder in men. J. Sex. Med. 2019, 5, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Orford, J. Hypersexuality: Implications for a theory of dependence. Addiction 1978, 3, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A. Sexual Addiction: Designation and treatment. J. Sex Marital Ther. 1992, 4, 303–314. [Google Scholar] [CrossRef]
- Goodman, A. What’s in a name? Terminology for designating a syndrome of driven sexual behavior. Sex. Addict. Compulsivity 2001, 3–4, 191–213. [Google Scholar] [CrossRef]
- Wines, D. Exploring the applicability of criteria for substance dependence to sexual addiction. Sex. Addict. Compulsivity 1997, 3, 195–220. [Google Scholar] [CrossRef]
- Carnes, P.J.; Hopkins, T.A.; Green, B.A. Clinical relevance of the proposed sexual addiction diagnostic criteria. J. Addict. Med. 2014, 6, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.; Hajela, R.; Hilton, D.L. Sex Addiction as a disease: Evidence for assessment, diagnosis, and response to critics. Sex. Addict. Compulsivity 2015, 2, 167–192. [Google Scholar] [CrossRef]
- Kafka, M.P. Hypersexual Disorder: A proposed diagnosis for DSM-V. Arch. Sex. Behav. 2009, 2, 377–400. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.C.; Carpenter, B.N.; Hook, J.N.; Garos, S.; Manning, J.C.; Gilliland, R.; Cooper, E.B.; McKittrick, H.; Davtian, M.; Fong, T. Report of findings in a DSM-5 field trial for hypersexual disorder. J. Sex. Med. 2012, 11, 2868–2877. [Google Scholar] [CrossRef]
- Engel, J.; Veit, M.; Sinke, C.; Heitland, I.; Kneer, J.; Hillemacher, T.; Hartmann, U.; Kruger, T. Same same but different: A clinical characterization of men with hypersexual disorder in the Sex@Brain study. J. Clin. Med. 2019, 2, 157. [Google Scholar] [CrossRef]
- Kraus, S.W.; Krueger, R.B.; Briken, P.; First, M.B.; Stein, D.J.; Kaplan, M.S.; Voon, V.; Abdo, C.H.N.; Grant, J.E.; Atalla, E.; et al. Compulsive sexual behaviour disorder in the ICD-11. World Psychiatry 2018, 1, 109–110. [Google Scholar] [CrossRef]
- Kraus, S.W.; Sweeney, P.J. Hitting the target: Considerations for differential diagnosis when treating individuals for problematic use of pornography. Arch. Sex. Behav. 2018, 2, 431–435. [Google Scholar] [CrossRef]
- Bancroft, J.; Vukadinovic, Z. Sexual addiction, sexual compulsivity, sexual impulsivity, or what? Toward a theoretical model. J. Sex Res. 2004, 3, 225–234. [Google Scholar] [CrossRef]
- Kafka, M.P. What happened to hypersexual disorder? Arch. Sex. Behav. 2014, 7, 1259–1261. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.C.; Garos, S.; Carpenter, B.N. Reliability, validity, and psychometric development of the Hypersexual Behavior Inventory in an outpatient sample of men. Sex. Addict. Compulsivity 2011, 1, 30–51. [Google Scholar] [CrossRef]
- Bőthe, B.; Kovács, M.; Tóth-Király, I.; Reid, R.C.; Griffiths, M.D.; Orosz, G.; Demetrovics, Z. The psychometric properties of the Hypersexual Behavior Inventory using a large-scale nonclinical sample. J. Sex Res. 2018, 2, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Kafka, M.P.; Hennen, J. The paraphilia-related disorders: An empirical investigation of nonparaphilic hypersexuality disorders in outpatient males. J. Sex Marital Ther. 1999, 4, 305–319. [Google Scholar] [CrossRef] [PubMed]
- Långström, N.; Hanson, R.K. High rates of sexual behavior in the general population: Correlates and predictors. Arch. Sex. Behav. 2006, 1, 37–52. [Google Scholar] [CrossRef]
- Winters, J.; Christoff, K.; Gorzalka, B.B. Dysregulated sexuality and high sexual desire: Distinct constructs? Arch. Sex. Behav. 2010, 5, 1029–1043. [Google Scholar] [CrossRef]
- Carvalho, J.; Štulhofer, A.; Vieira, A.L.; Jurin, T. Hypersexuality and high sexual desire: Exploring the structure of problematic sexuality. J. Sex. Med. 2015, 6, 1356–1367. [Google Scholar] [CrossRef]
- Štulhofer, A.; Jurin, T.; Briken, P. Is high sexual desire a facet of male hypersexuality? Results from an online study. J. Sex Marital Ther. 2015, 8, 665–680. [Google Scholar] [CrossRef]
- Van Tuijl, P.; Tamminga, A.; Meerkerk, G.-J.; Verboon, P.; Leontjevas, R.; van Lankveld, J. Het seksverslavingsmodel van hyperseksualiteit getoetst: Essentiële kenmerken en hun samenhang met hulpbehoefte. Tijdschr. Voor Seksuol. 2019, 4, 201–213. [Google Scholar]
- Beach, L.R. Cue probabilism and inference behavior. Psychol. Monogr. Gen. Appl. 1964, 5–6, 1–20. [Google Scholar] [CrossRef]
- Reed, S.K. Pattern recognition and categorization. Cogn. Psychol. 1972, 3, 382–407. [Google Scholar] [CrossRef]
- Reid, R.C. How should severity be determined for the DSM-5 proposed classification of Hypersexual Disorder? J. Behav. Addict. 2015, 4, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Vet, H.D.C.W. Measurement in Medicine: A Practical Guide (Practical Guides to Biostatistics and Epidemiology), 1st ed.; Cambridge University Press: Cambridge, UK, 2011; pp. 202–210. [Google Scholar]
- Meerkerk, G.-J.; van den Ende, D.V.M.; Altenburg, M.; Schoenmakers, T.M. De Opwinding Voorbij. Aard, Ernst en Omvang van Gbruik en Problematisch Gebruik van Online Pornografie in Nederland; IVO: Rotterdam, The Netherlands, 2011; pp. 11–14. [Google Scholar]
- Wakefield, J.C. The DSM-5′s proposed new categories of sexual disorder: The problem of false positives in sexual diagnosis. Clin. Soc. Work J. 2011, 2, 213–223. [Google Scholar] [CrossRef]
- Revelle, W. Procedures for Personality and Psychological Research; Northwestern University: Evanston, IL, USA, 2019. [Google Scholar]
- Courtney, M.; Gordon, R. Determining the Number of Factors to Retain in EFA: Using the SPSS R-Menu v2 0 to Make More Judicious Estimations. Pract. Assess. Res. Eval. 2013, 18, 1–15. [Google Scholar] [CrossRef]
- Sakaluk, J.K.; Short, S.D. A methodological review of exploratory factor analysis in sexuality research: Used practices, best practices, and data analysis resources. J. Sex Res. 2016, 1, 1–9. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 1, 1–55. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 1, 77. [Google Scholar]
- Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 2. [Google Scholar] [CrossRef]
- Hosmer, D.W., Jr.; Lemeshow, S.S.R. Applied logistic regression, 3rd ed.; Wiley and sons: Hoboken, NZ, USA, 2013. [Google Scholar]
- Grubbs, J.B.; Perry, S.L.; Wilt, J.A.; Reid, R.C. Pornography problems due to moral incongruence: An integrative model with a systematic review and meta-analysis. Arch. Sex. Behav. 2018, 2, 397–415. [Google Scholar] [CrossRef]
- Perry, S.L.; Davis, J.T. Are pornography users more likely to experience a romantic breakup? Evidence from Longitudinal Data. Sex. Cult. 2017, 4, 1157–1176. [Google Scholar] [CrossRef]
- Ebner-Priemer, U.W.; Trull, T.J. Ecological momentary assessment of mood disorders and mood dysregulation. Psychol. Assess. 2009, 4, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Gilliland, R.; South, M.; Carpenter, B.N.; Hardy, S.A. The roles of shame and guilt in hypersexual behavior. Sex. Addict. Compulsivity 2011, 1, 12–29. [Google Scholar] [CrossRef]
- Kafka, M.P. Hypersexual desire in males: An operational definition and clinical implications for males with paraphilias and paraphilia-related disorders. Arch. Sex. Behav. 1997, 5, 505–526. [Google Scholar] [CrossRef] [PubMed]
- Giles, J. No Such Thing as Excessive Levels of Sexual Behavior. Arch. Sex. Behav. 2006, 6, 641–642. [Google Scholar] [CrossRef] [PubMed]
- De Guzmán, I.N.; Arnau, R.C.; Green, B.A.; Carnes, S.; Carnes, P.; Jore, J. Empirical identification of psychological symptom subgroups of sex addicts: An application of latent profile analysis. Sex. Addict. Compulsivity 2016, 23, 34–55. [Google Scholar] [CrossRef]
- American Medical Association ICD-10-CM 2016: The Complete Official Draft Code Set; American Medical Association: Evanston, IL, USA, 2016.


{kind=link}
| Indicator Variables and Covariates | Experiences the Need for Help for PH. Women: n (%) (of a Total of 958) Men: n (%) (of a Total of 6625) | Does not Want Help for PH. Women: n (%) (of a Total of 6469) Men: n (%) (of a Total of 19,108) | AUC Women Men |
|---|---|---|---|
| Preoccupation with sex | 611 (63.8%) 4736 (71.5%) | 2827 (43.7%) 9700 (50.8%) | 0.60 0.60 |
| Failed to quit | 696 (72.6%) 5401 (81.5%) | 2428 (37.5%) 9232 (48.3%) | 0.68 0.67 |
| Negative consequences | 478 (49.9%) 3826 (57.7%) | 1223 (18.9%) 5205 (27.2%) | 0.66 0.65 |
| Continue despite negative consequences | 759 (79.2%) 5704 (86.1%) | 2392 (37.0%) 9668 (50.6%) | 0.71 0.68 |
| Tolerance | 691 (72.1%) 3439 (51.9%) | 3908 (60.4%) 7702 (40.3%) | 0.56 0.56 |
| Withdrawal (range: 0–4), mean (SD) | 1.92 (1.34) 1.78 (1.19) | 1.08 (1.25) 1.14 (1.19) | 0.68 0.66 |
| Need sex to function | 631 (65.9%) 3615 (54.6%) | 3369 (52.1%) 9277 (48.6%) | 0.57 0.53 |
| Distracted by sex | 679 (70.9%) 3914 (59.1%) | 3982 (61.6%) 9503 (49.7%) | 0.55 0.55 |
| Feel stronger | 454 (47.4%) 1893 (28.6%) | 2376 (36.7%) 4939 (25.8%) | 0.55 0.51 |
| Less depressed | 502 (52.4%) 2479 (37.4%) | 2386 (36.9%) 5492 (28.7%) | 0.58 0.54 |
| Less anxious | 390 (40.7%) 1493 (22.5%) | 1530 (23.7%) 2526 (13.2%) | 0.59 0.54 |
| Better deal with life | 407 (42.5%) 1626 (24.5%) | 2131 (32.9%) 4274 (22.4%) | 0.55 0.51 |
| Loss of pleasure | 513 (53.5%) 3958 (59.7%) | 1496 (23.1%) 6035 (31.6%) | 0.65 0.64 |
| Orgasm frequency | 529 (55.2%) 4174 (63.0%) | 3368 (52.1%) 11,858 (62.1%) | 0.53 0.52 |
| Time spent on porn (hours), mean (SD) | 21 min (20 min) 42 min (37 min) | 15 min (17 min) 32 min (33 min) | 0.59 0.58 |
| Extreme porn (range: 0–3), mean (SD) | 2.02 (1.12) 2.22 (0.77) | 1.70 (1.16) 2.09 (0.79) | 0.58 0.55 |
| Use drugs while watching porn (range: 0–4), mean (SD) | 1.43 (0.87) 1.34 (0.72) | 1.29 (0.76) 1.30 (0.68) | 0.55 0.51 |
| Social pressure | 423 (44.2%) 2136 (32.2%) | 1006 (15.6%) 2760 (14.2%) | 0.64 0.59 |
| Unusual sexual stimuli (range: 0–4), mean (SD) | 0.51 (0.96) 0.37 (0.77) | 0.28 (0.71) 0.23 (0.61) | 0.56 0.54 |
| Age, mean (SD) | 31 years 6 months (8 years y 11 months) 36 years 2 months (11 years 8 months) | 32 years 4 months (9 years 4 months) 36 years 3 months (12 years 4 months) | 0.47 0.50 |
| Potential Indicators of PH | Negative Effects Women/Men | Coping Women/Men | Extreme Women/Men | Sexual Desire Women/Men |
|---|---|---|---|---|
| Fail to quit | 0.69/0.61 | |||
| Negative consequences | 0.65/0.43 | |||
| Continue despite negative effects | 0.86/0.69 | |||
| Loss of pleasure | 0.55/0.51 | |||
| Social pressure | 0.75/0.31 | |||
| Withdrawal | 0.51/0.44 | |||
| Distracted by sex | 0.68/0.44 | |||
| Feel stronger | 0.76/0.41 | |||
| Less depressed | 0.83/0.68 | |||
| Less anxious | 0.90/0.62 | |||
| Better deal with life | 0.61/0.39 | |||
| Extreme porn | 0.80/0.69 | |||
| Time spent on porn | 0.84/0.60 | |||
| Use drugs while watching porn | 0.38/0.30 | |||
| Unusual sexual stimuli | 0.39/0.35 | |||
| Need sex to function | 0.70/0.56 | |||
| Tolerance | 0.52/0.39 | |||
| Preoccupation with sex | 0.41/0.29 | |||
| Orgasm frequency | 0.47/0.22 | |||
| Explained variance | 16.8%/9.6% | 15.6%/7.9% | 10.9%/6.7% | 9.4%/5.5% |
| Total explained variance | Women: 52.8% | Men: 29.7% | ||
| Eigenvalue | 3.19/1.82 | 2.97/1.49 | 2.01/1.28 | 1.79/1.05 |
| Cronbach’s alpha | 0.64/0.62 | 0.76/0.68 | 0.64/0.56 | 0.61/0.46 |
| Factors/Covariates (Range) | Women OR (99% CI) | Women p-Value | Men OR (99% CI) | Men p-Value |
|---|---|---|---|---|
| Intercept | 0.03 (0.02–0.04) | <0.001 | 0.05 (0.04–0.06) | <0.001 |
| Negative Effects (0–6) | 1.95 (1.84–2.10) | <0.001 | 1.95 (1.88–2.01) | <0.001 |
| Coping (0–5) | 1.05 (0.98–1.12) | 0.066 | 1.02 (0.99–1.05) | 0.100 |
| Extreme (0–4) | 1.20 (1.02–1.41) | 0.003 | 1.10 (1.01–1.21) | 0.005 |
| Sexual Desire (0–4/0–2) | 0.87 (0.79–0.97) | <0.001 | 0.85 (0.80–0.91) | <0.001 |
| Preoccupation with sex (0–1) | 1.32 (1.18–1.46) | <0.001 | ||
| Orgasm frequency (0–1) | 0.89 (0.80–0.99) | <0.001 | ||
| Age (0–6) | 1.02 (0.89–1.14) | 0.735 | 1.02 (0.98–1.06) | 0.156 |
| Factors/Covariates | Women AUC (99% CI) | Men AUC (99% CI) |
|---|---|---|
| Negative Effects | 0.80 (0.79–0.83) | 0.78 (0.77–0.78) |
| Coping | 0.60 (0.59–0.62) | 0.57 (0.56–0.58) |
| Extreme | 0.60 (0.58–0.62) | 0.58 (0.57–0.59) |
| Sexual Desire | 0.61 (0.59–0.63) | 0.56 (0.55–0.56) |
| Orgasm frequency (men) | 0.51 (0.50–0.51) | |
| Preoccupation with sex (men) | 0.60 (0.60–0.61) | |
| Age | 0.47 (0.46–0.49) | 0.50 (0.49–0.51) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Tuijl, P.; Tamminga, A.; Meerkerk, G.-J.; Verboon, P.; Leontjevas, R.; van Lankveld, J. Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior? Int. J. Environ. Res. Public Health 2020, 17, 6907. https://doi.org/10.3390/ijerph17186907
van Tuijl P, Tamminga A, Meerkerk G-J, Verboon P, Leontjevas R, van Lankveld J. Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior? International Journal of Environmental Research and Public Health. 2020; 17(18):6907. https://doi.org/10.3390/ijerph17186907
Chicago/Turabian Stylevan Tuijl, Piet, Aerjen Tamminga, Gert-Jan Meerkerk, Peter Verboon, Ruslan Leontjevas, and Jacques van Lankveld. 2020. "Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior?" International Journal of Environmental Research and Public Health 17, no. 18: 6907. https://doi.org/10.3390/ijerph17186907
APA Stylevan Tuijl, P., Tamminga, A., Meerkerk, G.-J., Verboon, P., Leontjevas, R., & van Lankveld, J. (2020). Three Diagnoses for Problematic Hypersexuality; Which Criteria Predict Help-Seeking Behavior? International Journal of Environmental Research and Public Health, 17(18), 6907. https://doi.org/10.3390/ijerph17186907