Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. General Interview
2.3. General Health Assessment
2.4. Neurological System Assessment
2.5. Respiratory Function Assessment Using a Spirometer
2.6. Analysis of Hg and Other Heavy Metals in the Hair
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Participants and Results of the General Interview
3.2. Result of General Interview
3.3. Clinical Findings and Analysis of Heavy Metal
3.4. Spirometry Test and Analysis of Lung Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Artisanal and Small-Scale Gold Mining and Health- Technical Paper #1, Environmental and Occupational Health Hazards Associated with Artisanal and Small-Scale Gold Mining; World Health Organization: Geneva, Switzerland, 2016; pp. 1–26. [Google Scholar]
- United Nations Environment Programme (UNEP). United Nations Environment Programme Global Mercury Assessment 2013: Sources, Emissions, Releases and Environmental Transport.; UNEP Division of Technology, Industry and Economics, Chemicals Branch International Environment House: Geneva, Switzerland, 2015; pp. 1–38. [Google Scholar]
- World Health Organization (WHO); United Nations Environmental programme (UNEP). Guidance for Identifying Populations at Risk from Mercury Exposure; UNEP: Geneva, Switzerland, 2008; pp. 1–176. [Google Scholar]
- Gibb, H.; O’Leary, K.G. Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: A comprehensive review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Exposure to mercury: A major public health concern—Preventing disease through healthy environments; Public Health and Environment, World Health Organization: Geneva, Switzerland, 2007; pp. 1–4. Available online: https://www.who.int/phe/news/Mercury-flyer.pdf (accessed on 10 April 2020).
- Steckling, N.; Bose-O’Reilly, S.; Pinheiro, P.; Plass, D.; Shoko, D.; Drasch, G.; Bernaudat, L.; Siebert, U.; Hornberg, C. The burden of chronic mercury intoxication in artisanal small-scale gold mining in Zimbabwe: Data availability and preliminary estimates. Environ. Health A Glob. Access Sci. Source 2014, 13, 111. [Google Scholar] [CrossRef]
- Yard, E.E.; Horton, J.; Schier, J.G.; Caldwell, K.; Sanchez, C.; Lewis, L.; Gastaňaga, C. Mercury exposure among artisanal gold miners in Madre de Dios, Peru: A cross-sectional study. J. Med. Toxicol. 2012, 8, 441–448. [Google Scholar] [CrossRef]
- Harari, R.; Harari, F.; Gerhardsson, L.; Lundh, T.; Skerfving, S.; Strömberg, U.; Broberg, K. Exposure and toxic effects of elemental mercury in gold-mining activities in Ecuador. Toxicol. Lett. 2012, 213, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Tomicic, C.; Vernez, D.; Belem, T.; Berode, M. Human mercury exposure associated with small-scale gold mining in Burkina Faso. Int. Arch. Occup. Environ. Health 2011, 84, 539–546. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Drasch, G.; Beinhoff, C.; Tesha, A.; Drasch, K.; Roider, G.; Taylor, H.; Appleton, D.; Siebert, U. Health assessment of artisanal gold miners in Tanzania. Sci. Total Environ. 2010, 408, 796–805. [Google Scholar] [CrossRef]
- Gardner, R.M.; Nyland, J.F.; Silva, I.A.; Ventura, A.M.; de Souza, J.M.; Silbergeld, E.K. Mercury exposure, serum antinuclear/antinucleolar antibodies, and serum cytokine levels in mining populations in Amazonian Brazil: A cross-sectional study. Environ. Res. 2010, 110, 345–354. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Lettmeier, B.; Gothe, R.M.; Beinhoff, C.; Siebert, U.; Drasch, G. Mercury as a serious health hazard for children in gold mining areas. Environ. Res. 2008, 107, 89–97. [Google Scholar] [CrossRef]
- Silva, I.A.; Nyland, J.F.; Gorman, A.; Perisse, A.; Ventura, A.M.; Santos, E.C.; De Souza, J.M.; Burek, C.L.; Rose, N.R.; Silbergeld, E.K. Mercury exposure, malaria, and serum antinuclear/antinucleolar antibodies in amazon populations in Brazil: A cross-sectional study. Environ. Health A Glob. Access Sci. Source 2004, 3, 11. [Google Scholar] [CrossRef]
- Drake, P.L.; Rojas, M.; Reh, C.M.; Mueller, C.A.; Jenkins, F.M. Occupational exposure to airborne mercury during gold mining operations near el Callo, Venezuela. Int. Arch. Occup. Environ. Health 2001, 74, 206–212. [Google Scholar] [CrossRef]
- Drasch, G.; Böse-O’Reilly, S.; Beinhoff, C.; Roider, G.; Maydl, S. The Mt. Diwata study on the Philippines 1999—Assessing mercury intoxication of the population by small scale gold mining. Sci. Total Environ. 2001, 267, 151–168. [Google Scholar] [CrossRef]
- Ross, M.H.; Murray, J. Occupational respiratory disease in mining. Occup. Med. 2004, 54, 304–310. [Google Scholar] [CrossRef]
- Rajaee, M.; Yee, A.K.; Long, R.N.; Renne, E.P.; Robins, T.G.; Basu, N. Pulmonary function and respiratory health of rural farmers and artisanal and small scale gold miners in Ghana. Environ. Res. 2017, 158, 522–530. [Google Scholar] [CrossRef]
- Pateda, S.M.; Sakakibara, M.; Sera, K. Lung function assessment as an early biomonitor of mercury-induced health disorders in artisanal and small-scale gold mining areas in Indonesia. Int. J. Environ. Res. Public Health 2018, 15, 2480. [Google Scholar] [CrossRef]
- Osawa, T.; Hatsukawa, Y. Artisanal and small-scale gold mining in Myanmar: Preliminary research for environmental mercury contamination. Int. J. Hum. Cult. Stud. 2015, 25, 221–230. [Google Scholar] [CrossRef]
- Kawakami, T.; Konishi, M.; Imai, Y.; Soe, P.S. Diffusion of mercury from artisanal small-scale gold mining (ASGM) sites in Myanmar. GEOMATE 2019, 17, 228–235. [Google Scholar] [CrossRef]
- MCRB. Sector Wide Impact Assessment of Limestone, Gold and Tin Mining in Myanmar. Available online: https://www.myanmar-responsiblebusiness.org/pdf/SWIA/Mining/00-Myanmar-Mining-Sector-Wide-Assessment.pdf (accessed on 27 August 2020).
- Schulz, C.; Angerer, J.; Ewers, U.; Kolossa-Gehring, M. The German Human Biomonitorng Commission. Int. J. Hyg. Environ. Health 2007, 210, 373–382. [Google Scholar] [CrossRef]
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef]
- Glezos, J.D.; Albrecht, J.E.; Gair, R.D. Pneumonitis after Inhalatiion of mercury Vapours. Can. Respir. J. 2006, 13, 150–152. [Google Scholar] [CrossRef]
- Lim, H.E.; Shim, J.J.; Lee, S.Y.; Lee, S.H.; Kang, S.Y.; Jo, J.Y.; In, K.H.; Kim, H.G.; Yoo, S.H.; Kang, K.H. Mercury inhalation poisoning and acute lung injury. Korean J. Intern. Med. 1998, 13, 127–130. [Google Scholar] [CrossRef]
- Rowens, B.; Guerrero-Betancourt, D.; Gottlieb, C.A.; Boyes, R.J.; Eichenhorn, M.S. Respiratory failure and death following acute inhalation of mercury vapor: A clinical and histologic perspective. Chest 1991, 99, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Divecha, C.; Agarwal, S.; Tullu, M.S.; Deshmukh, C.T.; Agrawal, M.; Shaikh, S.S.A. Acute respiratory distress syndrome caused by mercury inhalation: A case report. J. Pediatric Intensive Care 2015, 4, 168–170. [Google Scholar]
- Park, J.-D.; Zheng, W. Human exposure and health effects of inorganic and elemental mercury. J. Prev. Med. Public Health 2012, 45, 344–352. [Google Scholar] [CrossRef]
- Friberg, L.; Mottet, N.K. Accumulation of methylmercury and inorganic mercury in the brain. Biol. Trace Elem. Res. 1989, 21, 201–206. [Google Scholar] [CrossRef]
- Klaassen, C.D. Casarett and Doull’s Toxicology and Basic Science of Poisoning, 8th ed.; McGraw-Hill Education: New York, NY, USA, 2013; p. 55. [Google Scholar]
- McDowell, M.A.; Dillon, C.F.; Osterloh, J.; Bolger, P.M.; Pellizzari, E.; Fernando, R.; de Oca, R.M.; Schober, S.E.; Sinks, T.; Jones, R.L.; et al. Hair mercury levels in U.S. children and women of childbearing age: Reference range data from NHANES 1999–2000. Environ. Health Perspect. 2004, 112, 1165–1171. [Google Scholar]
- International Programme on Chemical Safety (IPCS). Human Exposure Assessment. Environ. Health Criteria 214; World Health Organization: Geneva, Switzerland, 2000; Available online: http://www.inchem.org/documents/ehc/ehc/ehc214.htm (accessed on 15 July 2020).
- Tun, A.Z.; Wongsasuluk, P.; Siriwong, W. Heavy metals in the soils of placer small-scale gold mining sites in Myanmar. J. Health Pollut. 2020, 10, 1–12. [Google Scholar]
- Godt, J.; Scheidig, F.; Grosse-Siestrup, C.; Esche, V.; Brandenburg, P.; Reich, A.; Groneberg, D.A. The toxicity of cadmium and resulting hazards for human health. J. Occup. Med. Toxicol. 2006, 1, 22. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Von Schirnding, Y.E.; Prapamontol, T. Environmental lead exposure: A public health problem with global dimensions. Bull. World Health Organ. 2000, 78, 1068–1077. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Miners | Non-Miners | P Value |
|---|---|---|---|
| Number of respondents | 18 | 11 | |
| Sex | 12 male | 6 male | 0.51 |
| 6 female | 5 female | ||
| Age, y (mean ± SD) | 37.6 ± 15.2 | 56.1 ± 13.9 | 0.01 |
| BMI (mean ± SD) | 20.9 ± 4.6 | 25.4 ± 2.9 | 0.01 |
| Heavy Metals | Miners | Non-Miners |
|---|---|---|
| Hg, μg/g * | 0.93 (0.72–1.44) | 0.63 (0.53–0.67) |
| Pb, μg/g | 6.09 (3.67–17.61) | 5.26 (2.08–8.77) |
| As, μg/g | 0.20 (0.12–0.33) | 0.16 (0.11–0.24) |
| Cd, μg/g | 0.04 (0.01–0.10) | 0.05 (0.02–0.17) |
| Cu, μg/g | 11.09 (10.11–13.27) | 11.92 (10.82–15.09) |
| Respiratory Assessment | Miners | Non-Miners |
|---|---|---|
| Smoking status, n | ||
| Smoker | 8 | 2 |
| Nonsmoker | 10 | 9 |
| Duration of smoking, y median (IQR) | 18.5 (9.3–34.3) | 39.5 (34.3–44.8) |
| No. of cigarettes smoked per day median (IQR) | 4.0 (1.6–5.0) | 1.5 (1.3–1.8) |
| Brinkman index median (IQR) | 82.0 (6.5–171.3) | 54.0 (52.0–56.0) |
| FVC, L median (IQR) | 2.89 (2.26–3.37) | 2.11 (1.77–2.59) |
| % Prediction of FVC median (IQR) | 75.5 (64.5–86.8) | 77.0 (55.5–80.0) |
| FEV1, L median (IQR) | 2.49 (2.06–3.35) | 2.01 (1.71–2.51) |
| % Prediction of FEV1 median (IQR) | 81.5 (71.3–90.8) | 83.0 (64.5–91.5) |
| Spirometry interpretation, n (%) | ||
| Normal | 7 (38.9%) | 3 (27.3%) |
| Mild | 5 (27.8%) | 3 (27.3%) |
| Moderate/moderately severe | 5 (27.8%) | 5 (45.5%) |
| Severe | 1 (5.6%) | - |
| Variables | ||||
|---|---|---|---|---|
| FVC | FEV1 | Hg level of scalp hair | Pb level of scalp hair | |
| P value | 0.05 | 0.07 | 0.01 | 0.58 |
| Classification | Miners | Non-miners |
|---|---|---|
| FVC and age | 0.001 Δ | 0.001 Δ |
| FEV1 and age | 0.001 Δ | 0.001 Δ |
| FVC and smoking | 0.26 Δ | 0.01 Δ |
| FEV1 and smoking | 0.004 Δ | 0.01 Δ |
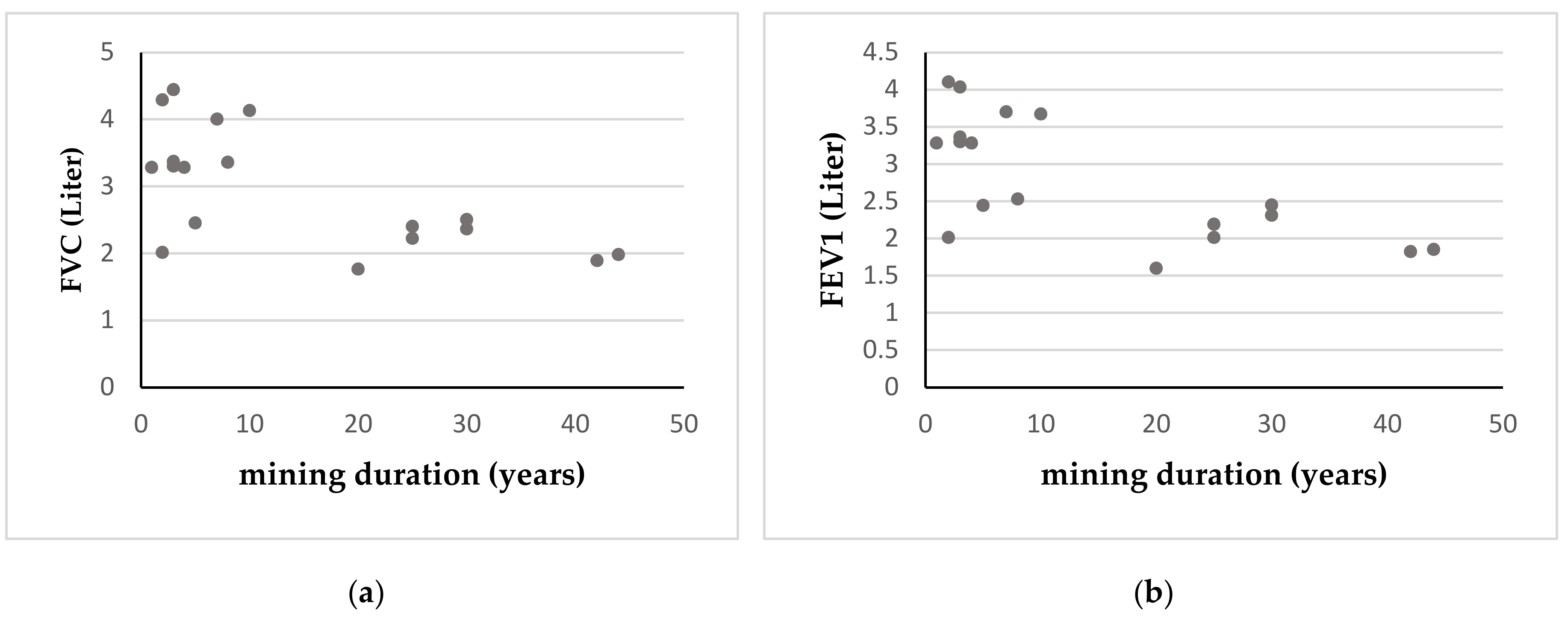
| FVC and mining duration | 0.001 ∗ | - |
| FEV1 and mining duration | 0.007 ∗ | - |
| FVC and Hg level | 0.68 ∗ | 0.80 ∗ |
| FEV1 and Hg level | 0.74 ∗ | 0.80 ∗ |
| FVC and Pb level | 0.12 ∗ | 0.70 ∗ |
| FEV1 and Pb level | 0.06 ∗ | 0.70 ∗ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyaw, W.T.; Kuang, X.; Sakakibara, M. Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research. Int. J. Environ. Res. Public Health 2020, 17, 6757. https://doi.org/10.3390/ijerph17186757
Kyaw WT, Kuang X, Sakakibara M. Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research. International Journal of Environmental Research and Public Health. 2020; 17(18):6757. https://doi.org/10.3390/ijerph17186757
Chicago/Turabian StyleKyaw, Win Thiri, Xiaoxu Kuang, and Masayuki Sakakibara. 2020. "Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research" International Journal of Environmental Research and Public Health 17, no. 18: 6757. https://doi.org/10.3390/ijerph17186757
APA StyleKyaw, W. T., Kuang, X., & Sakakibara, M. (2020). Health Impact Assessment of Artisanal and Small-Scale Gold Mining Area in Myanmar, Mandalay Region: Preliminary Research. International Journal of Environmental Research and Public Health, 17(18), 6757. https://doi.org/10.3390/ijerph17186757