Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes




Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Procedures
2.2. Questionnaire
2.3. Anthropometric Measurements
2.4. Fitness Measurements
2.5. Statistical Analyses
3. Results
3.1. Group Characteristics
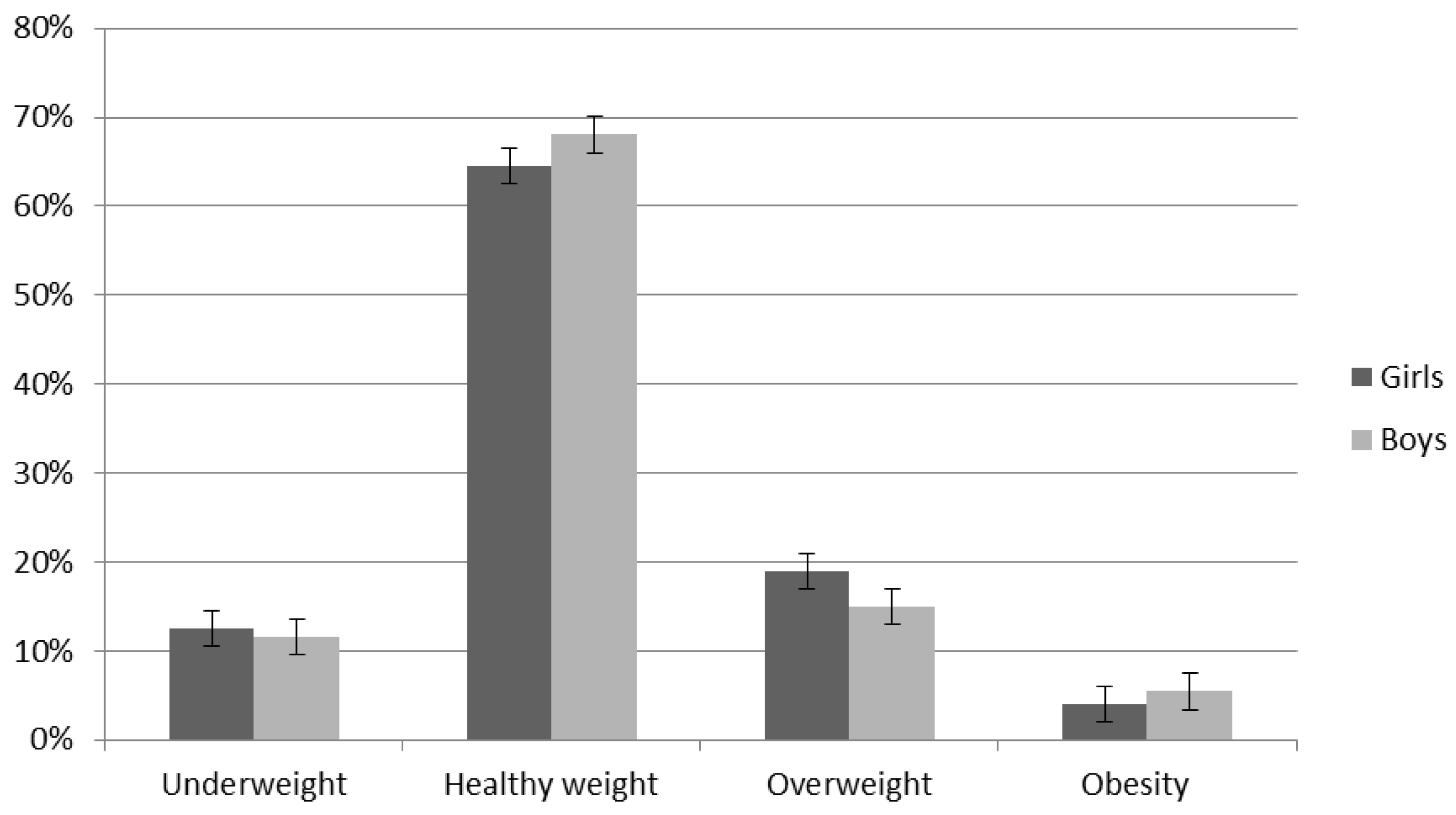
3.2. BMI
3.3. Eating Behaviour
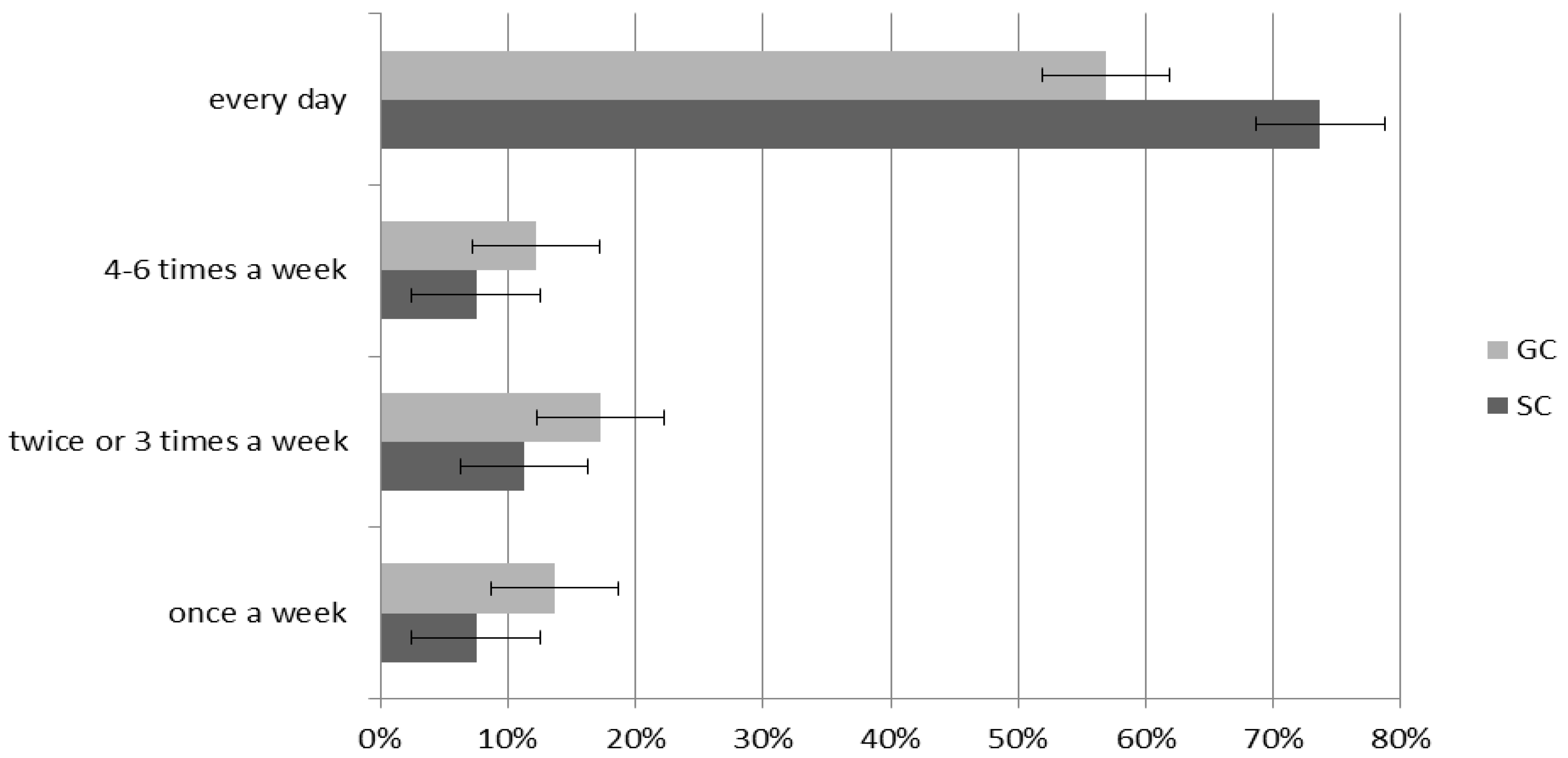
3.4. Extra-Curricular Sports Activity
3.5. Fitness Measurements
4. Discussions
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cairney, J.; Clark, H.J.; Kwan, M.Y.W.; Bruner, M.W.; Tamminen, K.A. Measuring sport experiences in children and youth to better understand the impact of sport on health and positive youth development: Designing a brief measure for population health surveys. BMC Public Health 2018, 18, 446. [Google Scholar] [CrossRef]
- Tabacchi, G.; López-Sánchez, G.F.; Sahin, F.N.; Kizilyalli, M.; Genchi, R.; Basile, M.; Kirkar, M.; Silva, C.; Loureiro, N.; Teixeira, E.; et al. Field-Based Tests for the Assessment of Physical Fitness in Children and Adolescents Practicing Sport: A Systematic Review within the ESA Program. Sustainability 2019, 11, 7187. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2007, 32, 1–11. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef]
- Vanhelst, J.; Ternynck, C.; Ovigneur, H.; Deschamps, T. Normative health-related fitness values for French children: The Diagnoform Programme. Scand. J. Med. Sci. Sports 2019, 30, 690–699. [Google Scholar] [CrossRef]
- Galan-Lopez, P.; Ries, F.; Gísladóttír, T.; Domínguez, R.; Sánchez-Oliver, A.J. Healthy Lifestyle: Relationship between Mediterranean Diet, Body Composition and Physical Fitness in 13 to 16-Years Old Icelandic Students. Int. J. Environ. Res. Public Health 2018, 15, 2632. [Google Scholar] [CrossRef]
- Žeželj, S.P.; Jovanović, G.K.; Dragaš-Zubalj, N.; Micovic, V.; Sesar, Ž. Associations between Adherence to the Mediterranean Diet and Lifestyle Assessed with the MEDLIFE Index among the Working Population. Int. J. Environ. Res. Public Health 2018, 15, 2126. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Román-Viñas, B.; Sanchez-Villegas, A.; Guasch-Ferre, M.; Corella, L.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol. Asp. Med. 2019, 67, 1–55. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Buja, A.; Grotto, G.; Brocadello, F.; Sperotto, M.; Baldo, V. Primary school children and nutrition: Lifestyles and behavioral traits associated with a poor-to-moderate adherence to the Mediterranean diet. A cross-sectional study. Eur. J. Nucl. Med. Mol. Imaging 2020, 179, 1–8. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Clavel, I.; Gallardo, L.; Garcia-Unanue, J. Relationship between Adherence to the Mediterranean Diet and Body Composition with Physical Fitness Parameters in a Young Active Population. Int. J. Environ. Res. Public Health 2020, 17, 3337. [Google Scholar] [CrossRef]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E.C.L. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef]
- Farajian, P.; Risvas, G.; Karasouli, K.; Pounis, G.; Kastorini, C.M.; Panagiotakos, D.; Zampelas, A. Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children: The GRECO study. Atherosclerosis 2011, 217, 525–530. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Mountjoy, M.; Andersen, L.B.; Armstrong, N.; Biddle, S.J.; Boreham, C.; Bedenbeck, H.-P.B.; Ekelund, U.; Engebretsen, L.; Hardman, K.; Hills, A.P.; et al. International Olympic Committee consensus statement on the health and fitness of young people through physical activity and sport. Br. J. Sports Med. 2011, 45, 839–848. [Google Scholar] [CrossRef]
- Lee, J.E.; Pope, Z.; Gao, Z. The Role of Youth Sports in Promoting Children’s Physical Activity and Preventing Pediatric Obesity: A Systematic Review. Behav. Med. 2016, 44, 62–76. [Google Scholar] [CrossRef]
- Park, J.-W.; Park, S.-H.; Koo, C.-M.; Eun, D.; Kim, K.-H.; Lee, C.-B.; Ham, J.-H.; Jang, J.-H.; Jee, Y.-S. Regular physical education class enhances sociality and physical fitness while reducing psychological problems in children of multicultural families. J. Exerc. Rehabil. 2017, 13, 168–178. [Google Scholar] [CrossRef]
- Patton, M.M.; Manore, M.M.; Branscum, A.J.; Meng, Y.; Wong, S.S. Changes in Sport Nutrition Knowledge, Attitudes/Beliefs and Behaviors Following a Two-Year Sport Nutrition Education and Life-Skills Intervention among High School Soccer Players. Nutrients 2018, 10, 1636. [Google Scholar] [CrossRef]
- Korcz, A.; Monyeki, M.A. Association Between Sport Participation, Body Composition, Physical Fitness, and Social Correlates Among Adolescents: The PAHL Study. Int. J. Environ. Res. Public Health 2018, 15, 2793. [Google Scholar] [CrossRef]
- Baptista, F.; Santos, D.A.; Silva, A.M.; Mota, J.; Santos, R.; Vale, S.; Ferreira, J.P.; Raimundo, A.M.; Moreira, M.H.R.; Sardinha, L. Prevalence of the Portuguese Population Attaining Sufficient Physical Activity. Med. Sci. Sports Exerc. 2012, 44, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Ekelund, U.; Sardinha, L. Associations between organized sports participation and objectively measured physical activity, sedentary time and weight status in youth. J. Sci. Med. Sport 2015, 19, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann-Sloutskis, D.; Wanner, M.; Zimmermann, E.; Martin, B.W. Physical activity levels and determinants of change in young adults: A longitudinal panel study. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Tremblay, M.; Barnes, J.D.; González, S.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef]
- Bergeron, M.F.; Mountjoy, M.; Armstrong, N.; Chia, M.; Côté, J.; Emery, C.; Faigenbaum, A.; Hall, G.; Kriemler, S.; Léglise, M.; et al. International Olympic Committee consensus statement on youth athletic development. Br. J. Sports Med. 2015, 49, 843–851. [Google Scholar] [CrossRef]
- Ørntoft, C.; Larsen, M.N.; Madsen, M.; Sandager, L.; Lundager, I.; Møller, A.; Hansen, L.; Madsen, E.E.; Elbe, A.-M.; Ottesen, L.; et al. Physical Fitness and Body Composition in 10–12-Year-Old Danish Children in Relation to Leisure-Time Club-Based Sporting Activities. BioMed Res. Int. 2018, 2018, 9807569. [Google Scholar] [CrossRef]
- Cvejic, D.; Pejovic, T.; Ostojic, S. Assessment of physical fitness in children and adolescents. Phys. Educ. Sport 2013, 11, 135–145. [Google Scholar]
- Council of Europe. Eurofit: Handbook for the Eurofit Tests of Physical Fitness; Council of Europe: Rome, Italy, 1988. [Google Scholar]
- Kemper, H.C.; Van Mechelen, W. Physical Fitness Testing of Children: A European Perspective. Pediatr. Exerc. Sci. 1996, 8, 201–214. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Olds, T.S.; Borms, J. Who are the Eurofittest? Med Sport Sci. 2007, 50, 104–128. [Google Scholar] [CrossRef]
- Lang, J.J.; Tremblay, M.S.; Ortega, F.B.; Ruiz, J.R.; Tomkinson, G.R. Review of criterion-referenced standards for cardiorespiratory fitness: What percentage of 1 142 026 international children and youth are apparently healthy? Br. J. Sports Med. 2017, 53, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.J.; Tremblay, M.S.; Léger, L.; Olds, T.S.; Tomkinson, G.R. International variability in 20 m shuttle run performance in children and youth: Who are the fittest from a 50-country comparison? A systematic literature review with pooling of aggregate results. Br. J. Sports Med. 2016, 52, 276. [Google Scholar] [CrossRef] [PubMed]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Inverse But Independent Trends in Obesity and Fitness Levels among Greek Children: A Time-Series Analysis from 1997 to 2007. Obes. Facts 2011, 4, 165–174. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Office of Research. Child Well-Being in Rich Countries: A Comparative Overview; UNICEF Office of Research: Florence, Italy, 2013; Innocenti Report Card 11. [Google Scholar]
- Regulation of the Ministry of National Education. Regulation of the Ministry of National Education of 27 March 2017 on sports branches and schools and sports championship branches and schools. J. Laws Repub. Pol. 2017, 671, 1–3. [Google Scholar]
- CZD. Percentile Grids for Children and Adolescents Aged 3–18 Years. CZD. Available online: http://www.czd.pl/index.php?option=com_content&view=article&id=1717&Itemid=538 (accessed on 9 April 2020).
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 2018, 52, 1445–1456. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; Leblanc, A.G.; Belanger, K.; Ortega, F.B.; Léger, L. International normative 20 m shuttle run values from 1 142 026 children and youth representing 50 countries. Br. J. Sports Med. 2016, 51, 1545–1554. [Google Scholar] [CrossRef]
- Ortega, F.B.; Artero, E.G.; Ruiz, J.R.; España-Romero, V.; Jiménez-Pavón, D.; Vicente-Rodriguez, G.; Moreno, L.A.; Manios, Y.; Béghin, L.; Ottevaere, C.; et al. Physical fitness levels among European adolescents: The HELENA study. Br. J. Sports Med. 2009, 45, 20–29. [Google Scholar] [CrossRef]
- Catley, M.J.; Tomkinson, G.R. Normative health-related fitness values for children: Analysis of 85347 test results on 9–17-year-old Australians since 1985. Br. J. Sports Med. 2011, 47, 98–108. [Google Scholar] [CrossRef]
- El Ghoch, M.; Soave, F.; Calugi, S.; Grave, R.D. Eating Disorders, Physical Fitness and Sport Performance: A Systematic Review. Nutrients 2013, 5, 5140–5160. [Google Scholar] [CrossRef]
- Bailey-Davis, L.; Poulsen, M.N.; Hirsch, A.G.; Pollak, J.; Glass, T.A.; Schwartz, B.S. Home Food Rules in Relation to Youth Eating Behaviors, Body Mass Index, Waist Circumference, and Percent Body Fat. J. Adolesc. Health 2016, 60, 270–276. [Google Scholar] [CrossRef]
- Somerset, S.; Hoare, D.J. Barriers to voluntary participation in sport for children: A systematic review. BMC Pediatr. 2018, 18, 47. [Google Scholar] [CrossRef] [PubMed]
- Arnaoutis, G.; Georgoulis, M.; Psarra, G.; Milkonidou, A.; Panagiotakos, D.B.; Kyriakou, D.; Bellou, E.; Tambalis, K.D.; Sidossis, L.S. Association of Anthropometric and Lifestyle Parameters with Fitness Levels in Greek Schoolchildren: Results from the EYZHN Program. Front. Nutr. 2018, 5, 10. [Google Scholar] [CrossRef]
- Bi, C.; Yang, J.; Sun, J.; Song, Y.; Wu, X.; Zhang, F. Benefits of normal body mass index on physical fitness: A cross-sectional study among children and adolescents in Xinjiang Uyghur Autonomous Region, China. PLoS ONE 2019, 14, e0220863. [Google Scholar] [CrossRef] [PubMed]
- Słowik, J.; Grochowska-Niedworok, E.; Maciejewska-Paszek, I.; Kardas, M.; Niewiadomska, E.; Szostak-Trybuś, M.; Palka-Słowik, M.; Irzyniec, T. Nutritional Status Assessment in Children and Adolescents with Various Levels of Physical Activity in Aspect of Obesity. Obes. Facts 2019, 12, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Shirreffs, S.M. Nutrition and hydration concerns of the female football player. Br. J. Sports Med. 2007, 41, i60–i63. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolaček, S.; Koletzko, B.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; Shamir, R.; Szajewska, H.; et al. Role of Dietary Factors and Food Habits in the Development of Childhood Obesity: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Gacek, M. Analysis of Dietetary habits among junior and senior soccer players as seen qualitative recommendations for athletes. Probl. Hig. Epidemiol. 2018, 99, 289–293. [Google Scholar]
- Abbey, E.L.; Wright, C.J.; Kirkpatrick, C.M. Nutrition practices and knowledge among NCAA Division III football players. J. Int. Soc. Sports Nutr. 2017, 14, 13. [Google Scholar] [CrossRef]
- Diethelm, K.; Jankovic, N.; Moreno, L.A.; Huybrechts, I.; De Henauw, S.; De Vriendt, T.; González-Gross, M.; Leclercq, C.; Gottrand, F.; Gilbert, C.C.; et al. Food intake of European adolescents in the light of different food-based dietary guidelines: Results of the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Heal. Nutr. 2011, 15, 386–398. [Google Scholar] [CrossRef]
- Purcell, L.K.; Canadian Paediatric Society; Paediatric Sports and Exercise Medicine Section. Sport nutrition for young athletes. Paediatr. Child Health 2013, 18, 200–202. [Google Scholar] [CrossRef]
- Grao-Cruces, A.; Fernández-Martínez, A.; Nuviala, A. Association of Fitness With Life Satisfaction, Health Risk Behaviors, and Adherence to the Mediterranean Diet in Spanish Adolescents. J. Strength Cond. Res. 2014, 28, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, L.M.; Nansel, T.R.; Haynie, D.; Liu, D.; Li, K.; Pratt, C.A.; Iannotti, R.J.; Dempster, K.; Simons-Morton, B. Diet quality of US adolescents during the transition to adulthood: Changes and predictors. Am. J. Clin. Nutr. 2017, 105, 1424–1432. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Rodrigues, A.P.; Silveira, E.A. Sport Types and Time Spent Playing Sport Are Associated with Eating Pattern Among Young Brazilian Athletes. Asian J. Sports Med. 2019, 10, 96561. [Google Scholar] [CrossRef]
- Całyniuk, B.; Kiciak, A.; Grochowska-Niedworok, E. Health- and nutrition-related behaviour of pupils attending sports schools in relation to their gender and body mass index—Preliminary report. Med. Og. Nauk. Zdr. 2014, 20, 186–191. [Google Scholar] [CrossRef]
- Dortch, K.S.; Gay, J.; Springer, A.; Kohl, H.W.; Sharma, S.; Saxton, D.; Wilson, K.; Hoelscher, D. The Association between Sport Participation and Dietary Behaviors among Fourth Graders in the School Physical Activity and Nutrition Survey, 2009–2010. Am. J. Heal. Promot. 2014, 29, 99–106. [Google Scholar] [CrossRef]
- Ministry of Health. Food and Nutrition Guidelines for Healthy Children and Young People (Aged 2–18 years): Background Paper—Revised February 2015; Ministry of Health: Wellington, New Zealand, 2015; pp. 1–190. [Google Scholar]
- Lake, A.A.; Mathers, J.C.; Rugg-Gunn, A.J.; Adamson, A.J. Longitudinal change in food habits between adolescence (11–12 years) and adulthood (32–33 years): The ASH30 study. J. Public Health 2006, 28, 10–16. [Google Scholar] [CrossRef]
- Cabrera, S.G.; Fernández, N.H.; Hernández, C.R.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. Kidmed Test: Prevalence of Low Adherence to the Mediterranean Diet in Children and Young: A Systematic Review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Evaristo, O.S.; Moreira, C.M.M.; Lopes, L.; Abreu, S.; Agostinis-Sobrinho, C.; Oliveira-Santos, J.; Póvoas, S.; Oliveira, A.; Santos, R.; Mota, J. Associations between physical fitness and adherence to the Mediterranean diet with health-related quality of life in adolescents: Results from the LabMed Physical Activity Study. Eur. J. Public Health 2018, 28, 631–635. [Google Scholar] [CrossRef]
- Moral-García, J.E.; Agraso-López, A.D.; Ramos-Morcillo, A.J.; Jiménez, A.; Jiménez-Eguizábal, A. The Influence of Physical Activity, Diet, Weight Status and Substance Abuse on Students’ Self-Perceived Health. Int. J. Environ. Res. Public Health 2020, 17, 1387. [Google Scholar] [CrossRef]
- Pino-Ortega, J.; De La Cruz-Sánchez, E.; Martínez-Santos, R. Health-related fitness in school children: Compliance with physical activity recommendations and its relationship with body mass index and diet quality. Arch. Latinoam. Nutr. 2010, 60, 374–379. [Google Scholar]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight Status, Adherence to the Mediterranean Diet, and Physical Fitness in Spanish Children and Adolescents: The Active Health Study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef] [PubMed]
- Steene-Johannessen, J.; Hansen, B.H.; Dalene, K.E.; Kolle, E.; Northstone, K.; Møller, N.C.; Grøntved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.S.; et al. Variations in accelerometry measured physical activity and sedentary time across Europe—Harmonized analyses of 47,497 children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Golle, K.; Granacher, U.; Hoffmann, M.; Wick, D.; Muehlbauer, T. Effect of living area and sports club participation on physical fitness in children: A 4 year longitudinal study. BMC Public Health 2014, 14, 499. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.N.; Nielsen, C.M.; Ørntoft, C.Ø.; Randers, M.; Manniche, V.; Hansen, L.; Hansen, T.; Bangsbo, J.; Krustrup, P. Physical Fitness and Body Composition in 8–10-Year-Old Danish Children Are Associated With Sports Club Participation. J. Strength Cond. Res. 2017, 31, 3425–3434. [Google Scholar] [CrossRef]
- Vänttinen, T.; Blomqvist, M.; Nyman, K.; Häkkinen, K. Changes in Body Composition, Hormonal Status, and Physical Fitness in 11-, 13-, and 15-Year-Old Finnish Regional Youth Soccer Players During a Two-Year Follow-Up. J. Strength Cond. Res. 2011, 25, 3342–3351. [Google Scholar] [CrossRef]
- Granacher, U.; Borde, R. Effects of Sport-Specific Training during the Early Stages of Long-Term Athlete Development on Physical Fitness, Body Composition, Cognitive, and Academic Performances. Front. Physiol. 2017, 8, 810. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Class | Average | Median | Min. | Max. | SD * | p |
|---|---|---|---|---|---|---|---|
| Body Weight | SC | 38.98 | 37.60 | 15.60 | 63.20 | 8.54 | p = 0.097 |
| GC | 41.60 | 39.40 | 25.70 | 90.00 | 11.65 | ||
| Height | SC | 146.03 | 145.00 | 128.00 | 168.00 | 6.60 | p = 0.182 |
| GC | 147.23 | 146.00 | 129.00 | 170.00 | 7.90 |
| Variable | Class | Average | Median | Min. | Max. | SD * | p |
|---|---|---|---|---|---|---|---|
| BMI | SC | 18.21 | 17.80 | 13.20 | 25.20 | 2.90 | p = 0.061 |
| GC | 18.96 | 18.20 | 13.30 | 33.90 | 3.79 | ||
| BMI Girls | SC | 18.23 | 18.00 | 13.20 | 24.80 | 2.95 | p = 0.437 |
| GC | 18.65 | 18.15 | 14.30 | 25.90 | 2.96 | ||
| BMI Boys | SC | 18.19 | 17.65 | 13.80 | 25.20 | 2.88 | p = 0.100 |
| GC | 19.21 | 18.40 | 13.30 | 33.90 | 4.35 |
| Variable | Underweight | Healthy Weight | Overweight | Obesity | ||||
|---|---|---|---|---|---|---|---|---|
| SC | ||||||||
| % | p | % | p | % | p | p | ||
| Total Population | 12.85 | - | 68.97 | - | 14.37 | - | 3.80 | - |
| Girls | 14.28 | 0.019 | 65.09 | 0.782 | 15.87 | 0.161 | 4.76 | 0.095 |
| Boys | 11.43 | 72.85 | 12.87 | 2.85 | ||||
| GC | ||||||||
| Total Population | 9.88 | - | 64.88 | - | 19.73 | - | 5.51 | - |
| Girls | 8.07 | 0.589 | 66.13 | 0.491 | 22.58 | 0.297 | 3.22 | 0.132 |
| Boys | 11.69 | 63.63 | 16.88 | 7.80 | ||||
| Lp. | Nutritional Behaviour n = 272 | SC | GC | χ2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ranks in a 5-Point Scale (% of Particular Ranks in the Group) * | ||||||||||||
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||
| 1. | Number of meals eaten during the day | 0.00 | 0.00 | 7.52 | 54.89 | 37.59 | 0.00 | 0.00 | 10.79 | 54.70 | 34.50 | χ2 = 0.96, df = 2, p = 0.616 VC = 0.05 |
| 2. | Type of food eaten between main meals | 24.81 | 18.80 | 0.00 | 41.35 | 15.04 | 33.81 | 26.62 | 0.00 | 35.97 | 3.60 | χ2 = 13.88, df = 3, p = 0.003 VC = 0.22 |
| 3. | Eating of milk and dairy products | 0.00 | 0.00 | 6.77 | 22.56 | 70.68 | 0.00 | 6.47 | 14.39 | 25.18 | 53.96 | χ2 = 15.95, df = 5, p = 0.006 VC = 0.24 |
| 4. | Eating of vegetables | 12.78 | 0.00 | 4.51 | 33.08 | 49.62 | 14.39 | 0.00 | 8.63 | 34.53 | 42.45 | χ2 = 2.67, df = 3, p = 0.044 VC = 0.09 |
| 5. | Eating of fruit | 0.00 | 0.00 | 3.01 | 22.56 | 74.44 | 0.00 | 0.00 | 9.35 | 17.99 | 72.66 | χ2 = 5.10, df = 3, p = 0.163 VC = 0.13 |
| 6. | Eating of white bread | 0.00 | 11.28 | 12.78 | 19.55 | 56.39 | 0.00 | 7.19 | 12.23 | 15.83 | 64.75 | χ2 = 2.56, df = 4, p = 0.632 VC = 0.09 |
| 7. | Eating of wholemeal bread | 22.56 | 6.02 | 33.83 | 11.28 | 26.32 | 25.90 | 21.58 | 28.78 | 5.04 | 18.71 | χ2 = 17.69, df = 4, p = 0.001 VC = 0.25 |
| 8. | Eating of thick groats, wholegrain pasta etc. | 11.28 | 14.29 | 45.11 | 18.05 | 11.28 | 18.00 | 6.47 | 48.20 | 18.71 | 8.63 | χ2 = 6.74, df = 4, p = 0.015 VC = 0.15 |
| 9. | Eating of small groats, ordinary pasta etc. | 0.00 | 0.00 | 17.30 | 22.56 | 60.15 | 0.00 | 0.00 | 19.42 | 18.71 | 61.87 | χ2 = 0.69, df = 4, p = 0.952 VC = 0.05 |
| 10. | Eating of poultry meat | 8.27 | 11.28 | 21.05 | 12.03 | 47.37 | 10.79 | 7.91 | 25.18 | 14.39 | 41.73 | χ2 = 2.52, df = 4, p = 0.639 VC= 0.09 |
| 11. | Eating of red meat | 11.28 | 8.27 | 33.83 | 30.08 | 16.54 | 12.59 | 6.47 | 20.14 | 34.53 | 25.90 | χ2 = 8.41, df = 4, p = 0.000 VC = 0.17 |
| 12. | Eating of fish | 9.02 | 23.31 | 67.67 | 0.00 | 0.00 | 20.14 | 17.99 | 61.87 | 0.00 | 0.00 | χ2 = 10.76, df = 4, p = 0.013 VC = 0.160 |
| 13. | Beverages | 13.53 | 14.29 | 22.56 | 0.00 | 49.62 | 21.58 | 20.14 | 15.83 | 0.00 | 42.44 | χ2 = 6.30, df = 5, p = 0.278 VC = 0.15 |
| 14. | Eating of fast food | 22.56 | 67.67 | 9.77 | 0.00 | 0.00 | 20.86 | 63.31 | 15.83 | 0.00 | 0.00 | χ2 = 2.22, df = 4, p = 0.695 VC = 0.09 |
| Mean | 9.72 | 12.51 | 20.40 | 20.57 | 36.78 | 12.69 | 13.15 | 20.76 | 19.68 | 33.65 | ||
| Variable | Class | Average | Median | Min. | Max. | SD * | p |
|---|---|---|---|---|---|---|---|
| 10 × 5 m Shuttle Run (s) | SC | 21.62 | 21.70 | 17.00 | 29.03 | 2.24 | p = 0.000 |
| GC | 23.02 | 22.66 | 17.89 | 32.09 | 2.70 | ||
| Standing Long Jump (cm) | SC | 141.03 | 140.00 | 100.00 | 195.00 | 19.85 | p = 0.022 |
| GC | 135.02 | 135.00 | 98.00 | 180.00 | 22.93 | ||
| sit-ups in 30 (n/30 s) | SC | 22.58 | 22.00 | 15.00 | 32.00 | 2.72 | p = 0.000 |
| GC | 20.05 | 20.00 | 2.00 | 27.00 | 4.00 |
| Variable | Sex Class | Average | Median | Min. | Max. | SD * | p |
|---|---|---|---|---|---|---|---|
| 10 × 5 m Shuttle Run (s). | Girls SC | 23.40 | 23.39 | 20.18 | 29.03 | 1.60 | p = 0.159 |
| Girls GC | 23.98 | 23.81 | 18.95 | 32.09 | 2.84 | ||
| Boys SC | 21.12 | 21.30 | 16.35 | 26.60 | 2.08 | p = 0.003 | |
| Boys GC | 22.21 | 21.850 | 17.89 | 32.00 | 2.30 | ||
| Standing Long Jump (cm). | Girls SC | 139.53 | 140.00 | 100.00 | 195.00 | 19.45 | p = 0.005 |
| Girls GC | 130.17 | 130.00 | 88.00 | 170.00 | 17.82 | ||
| Boys SC | 142.37 | 140.00 | 100.00 | 190.00 | 20.24 | p = 0.321 | |
| Boys GC | 138.61 | 140.00 | 0.98 | 180.00 | 25.07 | ||
| Sit-Ups in 30 s (n/30 s). | Girls SC | 22.30 | 22.00 | 15.00 | 29.00 | 2.42 | p = 0.000 |
| Girls GC | 18.43 | 18.00 | 6.00 | 25.00 | 3.51 | ||
| Boys SC | 22.84 | 22.500 | 18.00 | 32.00 | 2.95 | p = 0.008 | |
| Boys GC | 21.31 | 22.00 | 2.00 | 27.00 | 3.91 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ługowska, K.; Kolanowski, W.; Trafialek, J. Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes. Int. J. Environ. Res. Public Health 2020, 17, 6467. https://doi.org/10.3390/ijerph17186467
Ługowska K, Kolanowski W, Trafialek J. Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes. International Journal of Environmental Research and Public Health. 2020; 17(18):6467. https://doi.org/10.3390/ijerph17186467
Chicago/Turabian StyleŁugowska, Katarzyna, Wojciech Kolanowski, and Joanna Trafialek. 2020. "Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes" International Journal of Environmental Research and Public Health 17, no. 18: 6467. https://doi.org/10.3390/ijerph17186467
APA StyleŁugowska, K., Kolanowski, W., & Trafialek, J. (2020). Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes. International Journal of Environmental Research and Public Health, 17(18), 6467. https://doi.org/10.3390/ijerph17186467