A Combination of Full Pulpotomy and Chairside CAD/CAM Endocrown to Treat Teeth with Deep Carious Lesions and Pulpitis in a Single Session: A Preliminary Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Patients
2.3. Pulpotomy and Restoration Procedures
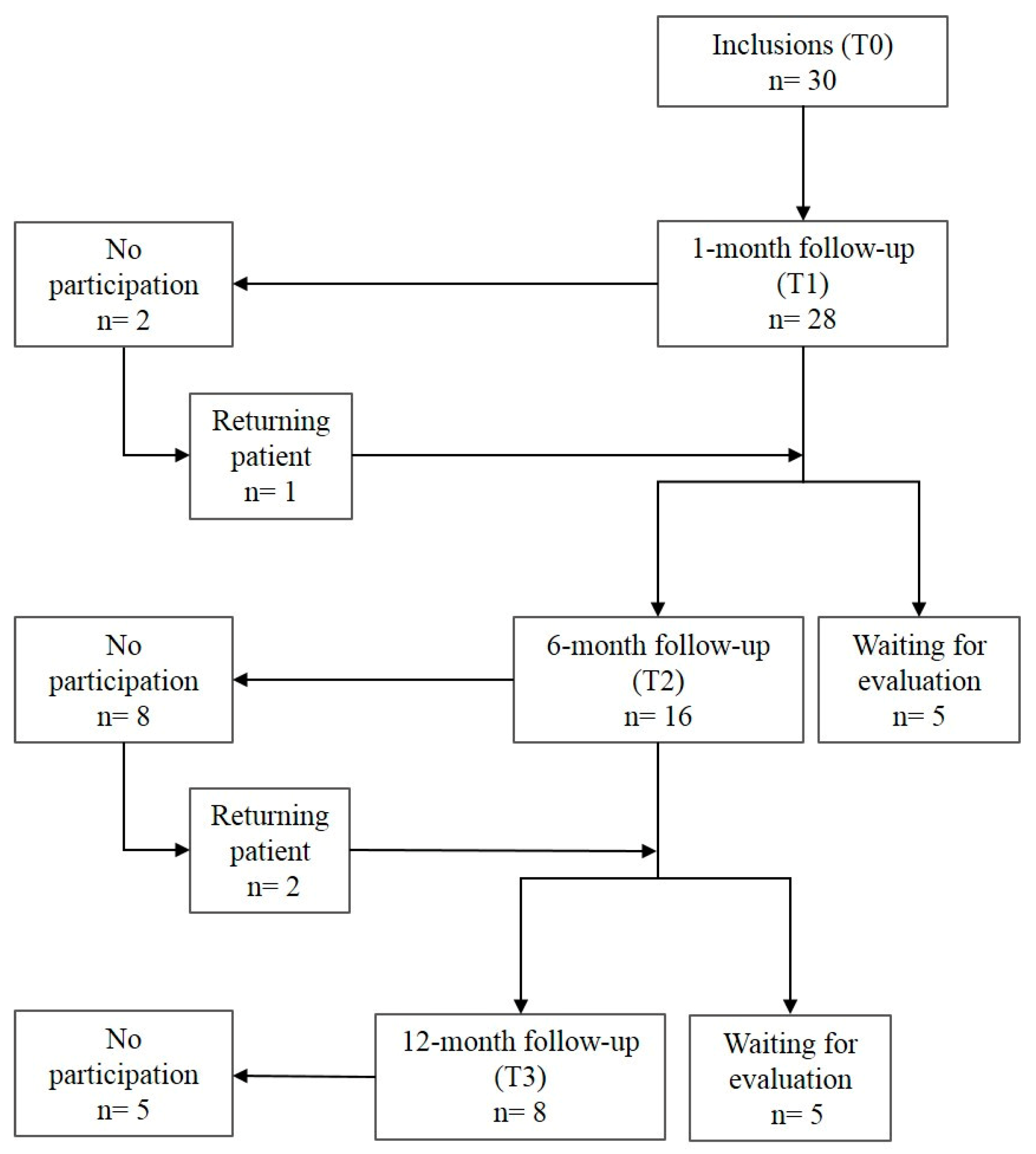
2.4. Follow up Evaluations
2.5. Study Criteria
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; Van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing carious lesions: Consensus recommendations on carious tissue removal. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Wolters, W.J.; Duncan, H.F.; Tomson, P.L.; Karim, I.E.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; Van Der Sluis, L.W.M. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 2017, 50, 825–829. [Google Scholar] [CrossRef]
- Bjørndal, L.; Reit, C.; Bruun, G.; Markvart, M.; Kjaeldgaard, M.; Näsman, P.; Thordrup, M.; Dige, I.; Nyvad, B.; Fransson, H.; et al. Treatment of deep caries lesions in adults: Randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur. J. Oral Sci. 2010, 118, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Maltz, M.; Koppe, B.; Jardim, J.J.; Alves, L.S.; De Paula, L.M.; Yamaguti, P.M.; Almeida, J.C.F.; Moura, M.S.; Mestrinho, H.D. Partial caries removal in deep caries lesions: A 5-year multicenter randomized controlled trial. Clin. Oral Investig. 2018, 22, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Fujitani, M.; Yamaki, C.; Momoi, Y. Ways of enhancing pulp preservation by stepwise excavation—A systematic review. J. Dent. 2011, 39, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Pérard, M.; Zanini, M.; Smith, A.J.; Charpentier, E.; Djole, S.X.; Lumley, P.J. Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughts. Int. Endod. J. 2013, 46, 79–87. [Google Scholar] [CrossRef]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of Mineral Trioxide Aggregate pulpotomy in mature permanent teeth with carious exposures. Int. Endod. J. 2017, 50, 117–125. [Google Scholar] [CrossRef]
- Zanini, M.; Hennequin, M.; Cousson, P. Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? A systematic review. Acta Odontol. Scand. 2019, 77, 541–551. [Google Scholar] [CrossRef]
- Taha, N.A.; Abdelkhader, S.Z. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int. Endod. J. 2018, 51, 819–828. [Google Scholar] [CrossRef]
- Cousson, P.-Y.; Nicolas, E.; Hennequin, M. A follow-up study of pulpotomies and root canal treatments performed under general anaesthesia. Clin. Oral Investig. 2014, 18, 1155–1163. [Google Scholar] [CrossRef]
- Aguilar, P.; Linsuwanont, P. Vital Pulp Therapy in Vital Permanent Teeth with Cariously Exposed Pulp: A Systematic Review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Awawdeh, L.; Al-Qudah, A.; Hamouri, H.; Chakra, R.J. Outcomes of Vital Pulp Therapy Using Mineral Trioxide Aggregate or Biodentine: A Prospective Randomized Clinical Trial. J. Endod. 2018, 44, 1603–1609. [Google Scholar] [CrossRef]
- Kunert, G.G.; Kunert, I.R.; Filho, L.C.D.C.; De Figueiredo, J.A.P. Permanent teeth pulpotomy survival analysis: Retrospective follow-up. J. Dent. 2015, 43, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Barthel, C.R.; Rosenkranz, B.; Leuenberg, A.; Roulet, J.F. Pulp Capping of Carious Exposures: Treatment Outcome after 5 and 10 Years: A Retrospective Study. J. Endod. 2000, 26, 525–528. [Google Scholar] [CrossRef]
- Dalpino, P.H.P.; E Francischone, C.; Ishikiriama, A.; Franco, E.B. Fracture resistance of teeth directly and indirectly restored with composite resin and indirectly restored with ceramic materials. Am. J. Dent. 2002, 15, 389–394. [Google Scholar] [PubMed]
- Dammaschke, T.; Nykiel, K.; Sagheri, D.; Schäfer, E. Influence of coronal restorations on the fracture resistance of root canal-treated premolar and molar teeth: A retrospective study. Aust. Endod. J. 2012, 39, 48–56. [Google Scholar] [CrossRef]
- Desai, P.; Das, U.; Pd, D.; Uk, D. Comparison of fracture resistance of teeth restored with ceramic inlay and resin composite: An in vitro study. Indian J. Dent. Res. 2011, 22, 877. [Google Scholar] [CrossRef]
- Liberman, R.; Ben-Amar, A.; Herteanu, L.; Judes, H. Marginal seal of composite inlays using different polymerization techniques. J. Oral Rehabilitation 1997, 24, 26–29. [Google Scholar] [CrossRef]
- Duquia, R.C.S.; Osinaga, P.W.R.; Demarco, F.F.; Habekost, L.V.; Conceição, E.N. Cervical Microleakage in MOD Restorations: In Vitro Comparison of Indirect and Direct Composite. Oper. Dent. 2006, 31, 682–687. [Google Scholar] [CrossRef]
- Manhart, J.; Neuerer, P.; Scheibenbogen-Fuchsbrunner, A.; Hickel, R. Three-year clinical evaluation of direct and indirect composite restorations in posterior teeth. J. Prosthet. Dent. 2000, 84, 289–296. [Google Scholar] [CrossRef]
- Manhart, J.; Chen, H.; Hamm, G.; Hickel, R. Buonocore Memorial Lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper. Dent. 2004, 29, 481–508. [Google Scholar]
- Bjørndal, L.; Simon, S.; Tomson, P.L.; Duncan, H.F. Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 949–973. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Zanini, M.; Hennequin, M.; Cousson, P.-Y. A Review of Criteria for the Evaluation of Pulpotomy Outcomes in Mature Permanent Teeth. J. Endod. 2016, 42, 1167–1174. [Google Scholar] [CrossRef]
- Hashem, D.; Mannocci, F.; Patel, S.; Manoharan, A.; Brown, J.; Watson, T.; Banerjee, A. Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: A randomized controlled clinical trial. J. Dent. Res. 2015, 94, 562–568. [Google Scholar] [CrossRef]
- Dummer, P.M.H.; Hicks, R.; Huws, D. Clinical signs and symptoms in pulp disease. Int. Endod. J. 1980, 13, 27–35. [Google Scholar] [CrossRef]
- Mejàre, I.; Axelsson, S.; Davidson, T.; Frisk, F.; Hakeberg, M.; Kvist, T.; Norlund, A.; Petersson, A.; Portenier, I.; Sandberg, H.; et al. Diagnosis of the condition of the dental pulp: A systematic review. Int. Endod. J. 2012, 45, 597–613. [Google Scholar] [CrossRef]
- Garfunkel, A.; Sela, J.; Ulmansky, M. Dental pulp pathosis. Clinicopathologic correlations based on 109 cases. Oral Surg. Oral Med. Oral Pathol. 1973, 35, 110–117. [Google Scholar] [CrossRef]
- Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; Markvart, M.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar]
- Marshall, G.W.; Habelitz, S.; Gallagher, R.; Balooch, M.; Balooch, G.; Marshall, S. Nanomechanical properties of hydrated carious human dentin. J. Dent. Res. 2001, 80, 1768–1771. [Google Scholar] [CrossRef]
- Isolan, C.P.; Sarkis-Onofre, R.; Lima, G.S.; Moraes, R.R. Bonding to Sound and Caries-Affected Dentin: A Systematic Review and Meta-Analysis. J. Adhes Dent 2018, 20, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Fages, M.; Bennasar, B. The endocrown: A different type of all-ceramic reconstruction for molars. J. Canadian Dent. Assoc. 2013, 79, d140. [Google Scholar]
- Biacchi, G.R.; Mello, B.; Basting, R.T. The Endocrown: An Alternative Approach for Restoring Extensively Damaged Molars. J. Esthet. Restor. Dent. 2013, 25, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Dogui, H.; Abdelmalek, F.; Amor, A.; Douki, N. Endocrown: An Alternative Approach for Restoring Endodontically Treated Molars with Large Coronal Destruction. Case Rep. Dent. 2018, 2018, 1581952. [Google Scholar] [CrossRef]
- Palma, P.; Marques, J.; Falacho, R.I.; Vinagre, A.; Santos, J.M.; Ramos, J.C. Does Delayed Restoration Improve Shear Bond Strength of Different Restorative Protocols to Calcium Silicate-Based Cements? Materials 2018, 11, 2216. [Google Scholar] [CrossRef]
- Kusumvalli, S.; Diwan, A.; Pasha, S.; Devale, M.R.; Chowdhary, C.D.; Saikia, P. Clinical evaluation of biodentine: Its efficacy in the management of deep dental caries. Indian J. Dent. Res. 2019, 30, 191–195. [Google Scholar] [CrossRef]
- Pham, C.-L.; Kratunova, E.; Marion, I.; da Fonseca, M.A.; Alapati, S.B. Effect of Overlying Material on Final Setting of Biodentine ® in Primary Molar Pulpotomies. Pediatr. Dent. 2019, 41, 140–145. [Google Scholar]
- Lander, E.; Dietschi, D. Endocrowns: A clinical report. Quintessence Int. 2008, 39, 99–106. [Google Scholar]
- Dejak, B.; Mlotkowski, A.; Romanowicz, M. Strength estimation of different designs of ceramic inlays and onlays in molars based on the Tsai-Wu failure criterion. J. Prosthet. Dent. 2007, 98, 89–100. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria | - Related to the patient
|
- Related to the tooth
| |
- Related to the pulpal status
| |
| Exclusion criteria | - Related to the patient
|
- Related to the tooth
| |
- Related to the pulpal status
| |
- Extemporaneous exclusion criteria
|
| Outcome of Pulpotomy | Clinical Criteria | Radiographic Criteria | |
|---|---|---|---|
| Functional Tooth | Noninfected Tooth | ||
| Success, effective pulpotomy | Lack of pain declaration and Presence of the tooth and Sealing properties of the restoration | Absence of spontaneous pain and Absence of pain on chewing and Lack of swelling and Lack of swelling and sinus tract and Negative response to axial percussion test and Negative response to apical palpation test and Periodontal probing <2mm | PAI at T0 = 1 and PAI at Tx = 1, PAI at T0 = 2 and PAI at Tx ≤ 2, or PAI at T0 3 and PAI at Tx ≤ 2 and lack of radicular lacunae |
| Uncertain outcome | Lack of pain declaration and Presence of the tooth and Sealing properties of the restoration | Absence of spontaneous pain and Absence of pain on chewing and Lack of swelling and Lack of swelling and sinus tract and Negative response to axial percussion test and Negative response to apical palpation test and Periodontal probing <2mm | PAI at T0 = 1 and PAI at Tx = 2, PAI = 3 at both T0 and Tx, and lack of radicular lacunae |
| Failure, ineffective pulpotomy | Lack of pain declaration and/or Presence of the tooth and/or Sealing properties of the restoration | Absence of spontaneous pain and/or Absence of pain on chewing and/or Lack of swelling and Lack of swelling and sinus tract and/or Negative response to axial percussion test and/or Negative response to apical palpation test and/or Periodontal probing <2mm | PAI at T0 = 1 or 2 and PAI at Tx 3, PAI at T0 3 and PAI at Tx > 3 and/or presence of radicular lacunae |
| Descriptive Criteria | Initial Evaluation (T0) | 12 Month Follow-Up (T3) |
|---|---|---|
| Diagnosis | ||
| Reversible pulpitis | 23 | 5 |
| Irreversible pulpitis | 2 | 1 |
| Chronic pulpitis | 5 | 2 |
| Total | 30 | 8 |
| Bjørndal classification | ||
| Deep carious lesion | 14 | 4 |
| Extremely deep carious lesion | 14 | 4 |
| No carious lesion | 2 | |
| Total | 30 | 8 |
| Endocrown material | ||
| IPS e.max® CAD | 15 | 2 |
| Enamic® | 15 | 6 |
| Total | 30 | 8 |
| Outcome | Follow-up Time | Clinical Criteria | Radiographic Criteria | Total | |
|---|---|---|---|---|---|
| Functional Tooth | Non-Infected Tooth | ||||
| Effective outcome | T1 | 28 (100%) | 24 (86%) | 27 (96%) | 23 |
| T2 | 16 (100%) | 16 (100%) | 15 (94%) | 15 | |
| T3 | 8 (100%) | 8 (100%) | 8 (100%) | 8 | |
| Uncertain | T1 | 0 | 4 (14%) * | 1 (4%) | 5 |
| T2 | 0 | 0 | 1 (6%) | 1 | |
| T3 | 0 | 0 | 0 | 0 | |
| Ineffective outcome | T1 | 0 | 0 | 0 | 0 |
| T2 | 0 | 0 | 0 | 0 | |
| T3 | 0 | 0 | 0 | 0 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munoz-Sanchez, M.-L.; Linas, N.; Decerle, N.; Nicolas, E.; Hennequin, M.; Cousson, P.-Y. A Combination of Full Pulpotomy and Chairside CAD/CAM Endocrown to Treat Teeth with Deep Carious Lesions and Pulpitis in a Single Session: A Preliminary Study. Int. J. Environ. Res. Public Health 2020, 17, 6340. https://doi.org/10.3390/ijerph17176340
Munoz-Sanchez M-L, Linas N, Decerle N, Nicolas E, Hennequin M, Cousson P-Y. A Combination of Full Pulpotomy and Chairside CAD/CAM Endocrown to Treat Teeth with Deep Carious Lesions and Pulpitis in a Single Session: A Preliminary Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6340. https://doi.org/10.3390/ijerph17176340
Chicago/Turabian StyleMunoz-Sanchez, Marie-Laure, Natacha Linas, Nicolas Decerle, Emmanuel Nicolas, Martine Hennequin, and Pierre-Yves Cousson. 2020. "A Combination of Full Pulpotomy and Chairside CAD/CAM Endocrown to Treat Teeth with Deep Carious Lesions and Pulpitis in a Single Session: A Preliminary Study" International Journal of Environmental Research and Public Health 17, no. 17: 6340. https://doi.org/10.3390/ijerph17176340
APA StyleMunoz-Sanchez, M.-L., Linas, N., Decerle, N., Nicolas, E., Hennequin, M., & Cousson, P.-Y. (2020). A Combination of Full Pulpotomy and Chairside CAD/CAM Endocrown to Treat Teeth with Deep Carious Lesions and Pulpitis in a Single Session: A Preliminary Study. International Journal of Environmental Research and Public Health, 17(17), 6340. https://doi.org/10.3390/ijerph17176340