An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Online Training Intervention
2.2. Assessment of the Online Training Programme
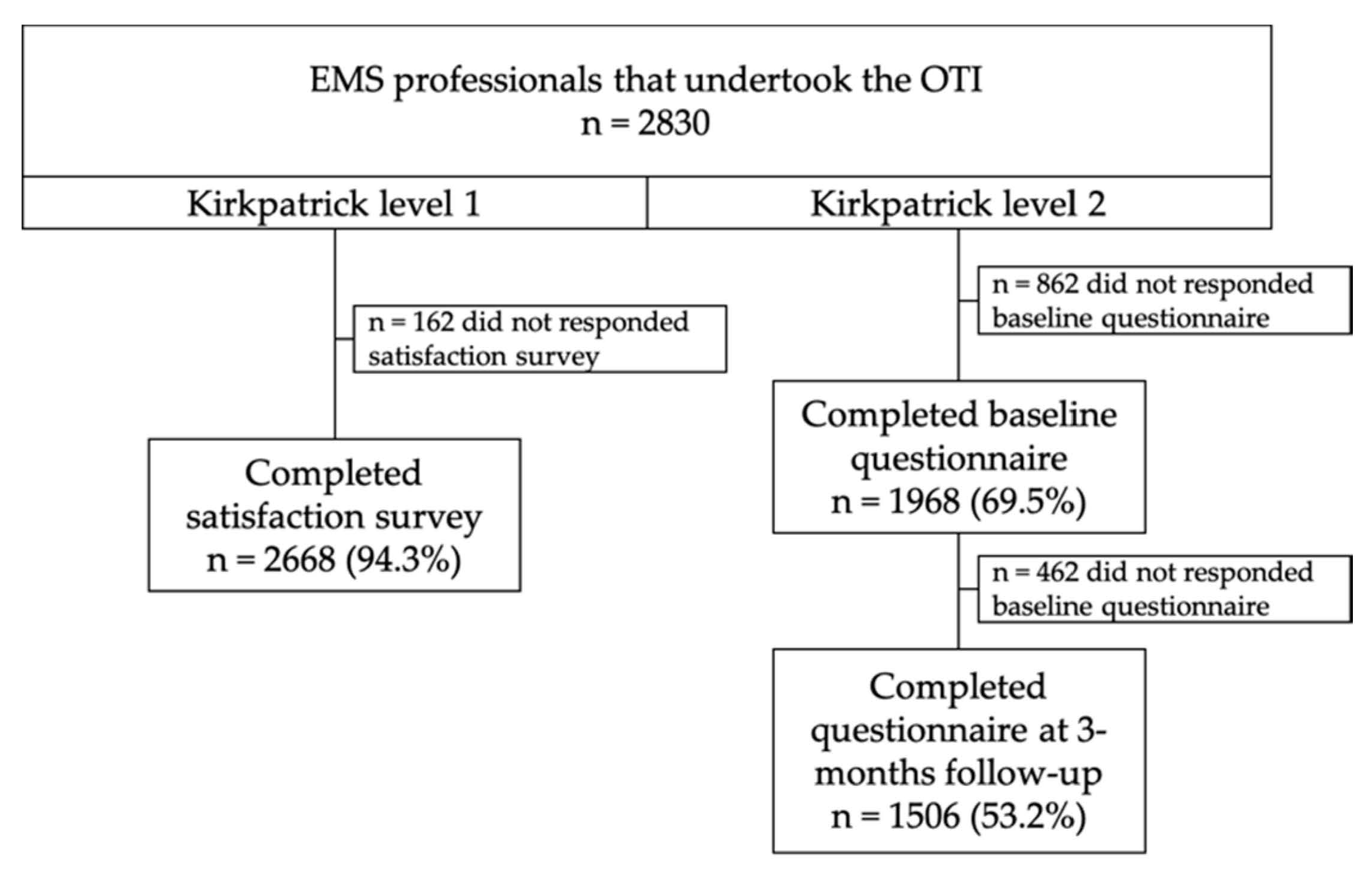
- Kirkpatrick level 1 (reaction): A satisfaction survey (Supplementary material S2) was administered at the end of the training using a five-point Likert scale based on five dimensions. Satisfaction of the aims of the training, the available materials, the RACE scale usefulness in clinical practice, and the faculty, as well as the overall satisfaction regarding the perceived increased in knowledge or competency, were addressed.
- Kirkpatrick level 2 (learning): A knowledge-related multiple-choice questionnaire about knowledge was administered prior to and 3 months after the intervention (Supplementary material S3). A set of 24 questions were used, most of which (i.e., 10) were related to the identification of signs and symptoms of a stroke, as well as available treatment options. Eight questions explored respondents’ knowledge on the SC protocol, prehospital management, and prehospital assessment scales for stroke patients. A final set of six questions were used to analyze the decision-making on acute stroke medical emergencies in clinical scenarios.
- Kirkpatrick level 3 (behavior): The transfer to clinical practice was measured by compliance rates with the EMS prenotification system (i.e., Minimum Data Set register). We observed the notification of the patient’s identification number, the time of the onset of symptoms, anticoagulant treatment, glycaemia, systolic and diastolic blood pressure, and RACE scores.
- Kirkpatrick level 4 (results): The impact of the intervention on prehospital SC was assessed by determining the number of activated codes and the changes in prehospital care times. The observed times were: (a) The alert time, that is, the period between the start and the end of a call; (b) the activation time, that is, the time from the start of a call to the allocation of clinical resources; (c) the response time, that is, the period from resource allocation to the arrival of the EMS team; (d) the care time, that is, the time from the arrival at the place of care to the start of the transfer; (e) the transfer time, that is, the period from the start of the transfer to the arrival at the receiving center; and (f) a global time was also registered.
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Learning Assessment (Kirkpatrick Level 2)
3.2. Transfer to the Clinical Setting (Kirkpatrick Level 3)
3.3. Impact on Prehospital Stroke Code (Kirkpatrick Level 4)
3.3.1. Stroke Code Activation
3.3.2. Time Performance in Stroke Code
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database. Syst. Rev. 2013, 2013, CD000197. [Google Scholar] [CrossRef]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischemic stroke: A meta-analysis of individual patient data from randomized trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.H.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- XLin, Y.; Schulze, V.; Brockmeyer, M.; Parco, C.; Karathanos, A.; Heinen, Y.; Gliem, M.; Hartung, H.P.; Antoch, G.; Jander, S.; et al. Endovascular Thrombectomy as a Means to Improve Survival in Acute Ischemic Stroke: A Meta-analysis. JAMA Neurol. 2019, 6–10. [Google Scholar] [CrossRef]
- De Luca, A.; Toni, D.; Lauria, L.; Sacchetti, M.L.; Giorgi Rossi, P.; Ferri, M.; Puca, E.; Prencipe, M.; Guasticchi, G.; The “IMPLementazione Percorso Clinico Assistenziale ICtus Acuto (IMPLICA) Study Group”. An emergency clinical pathway for stroke patients—Results of a cluster randomized trial (isrctn41456865). BMC Health Serv. Res. 2009, 9, 1–10. [Google Scholar] [CrossRef]
- Baldereschi, M.; Piccardi, B.; Di Carlo, A.; Lucente, G.; Guidetti, D.; Consoli, D.; Toni, D.; Sacchetti, M.L.; Polizzi, B.M.; Inzitari, D.; et al. Relevance of Prehospital Stroke Code Activation for Acute Treatment Measures in Stroke Care: A Review. Cerebrovasc. Dis. 2012, 10, 182–190. [Google Scholar] [CrossRef]
- Crocco, T.J.; Grotta, J.C.; Jauch, E.C.; Kasner, S.E.; Kothari, R.U.; Larmon, B.R.; Saver, J.L.; Sayre, M.R.; Davis, S.M. EMS management of acute stroke—Prehospital triage (resource document to NAEMSP position statement). Prehospital Emerg. Care 2007, 11, 313–317. [Google Scholar] [CrossRef]
- Powers, W.J.; Derdeyn, C.P.; Biller, J.; Coffey, C.S.; Hoh, B.L.; Jauch, E.C.; Johnston, K.C.; Johnston, S.C.; Khalessi, A.A.; Kidwellet, C.S.; et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients with Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2015, 46, 3020–3035. [Google Scholar] [CrossRef]
- Zhelev, Z.; Walker, G.; Henschke, N.; Fridhandler, J.; Yip, S. Prehospital stroke scales as screening tools for early identification of stroke and transient ischemic attack. Cochrane Database Syst. Rev. 2019, 4, CD011427. [Google Scholar] [CrossRef]
- Smith, E.E.; Kent, D.M.; Bulsara, K.R.; Leung, L.Y.; Lichtman, J.H.; Reeve, M.J.; Towfighi, A.; Whiteley, W.N.; Zahuranec, D.B. Accuracy of prediction instruments for diagnosing large vessel occlusion in individuals with suspected stroke: A systematic review for the 2018 guidelines for the early management of patients with acute ischemic stroke. Stroke 2018, 49, e111–e122. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; de Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischaemic StrokeEndorsed by Stroke Alliance for Europe (SAFE). Eur. Stroke J. 2019, 4, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.B.; Peterson, E.D.; Smith, E.E.; Saver, J.L.; Liang, L.; Xian, Y.; Olson, M.D.; Shah, B.R.; Hernandez, A.F.; Schwamm, L.H.; et al. Emergency medical service hospital prenotification is associated with improved evaluation and treatment of acute ischemic stroke. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Jauch, E.C.; Saver, J.L.; Chair, V.; Adams, H.P.; Bruno, A.; Connors, J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; et al. AHA/ASA Guidelines for the Early Management of Patients With Acute Ischemic Stroke A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Am. Hear. Assoc Stroke Counc. 2013, 44, 870–947. [Google Scholar] [CrossRef]
- Kobayashi, A.; Czlonkowska, A.; Ford, G.A.; Fonseca, A.C.; Luijckx, G.J.; Korv, J.; Pérez de la Ossa, N.; Price, C.; Russell, D.; Tsiskaridze, A.; et al. European Academy of Neurology and European Stroke Organization consensus statement and practical guidance for pre-hospital management of stroke. Eur. J. Neurol. 2018, 25, 425–433. [Google Scholar] [CrossRef]
- Boulanger, J.M.; Lindsay, M.P.; Gubitz, G.; Smith, E.E.; Stotts, G.; Foley, N.; Bhogal, S.; Boyle, K.; Braun, L.; Goddard, T.; et al. Canadian Stroke Best Practice Recommendations for Acute Stroke Management: Prehospital, Emergency Department, and Acute Inpatient Stroke Care, 6th Edition, Update 2018. Int. J. Stroke 2018, 13, 949–984. [Google Scholar] [CrossRef]
- De La Ossa, N.P.; Carrera, D.; Gorchs, M.; Querol, M.; Millán, M.; Gomis, M.; Dorado, L.; López-Cancio, E.; Hernández-Pérez, M.; Chicharro, V.; et al. Design and validation of a prehospital stroke scale to predict large arterial occlusion: The rapid arterial occlusion evaluation scale. Stroke 2014, 45, 87–91. [Google Scholar] [CrossRef]
- Pride, G.L.; Fraser, J.F.; Gupta, R.; Alberts, M.J.; Rutledge, J.N.; Fowler, R.; Ansari, S.A.; Abruzzo, T.; Albani, B.; Arthur, A.; et al. Prehospital care delivery and triage of stroke with emergent large vessel occlusion (ELVO): Report of the Standards and Guidelines Committee of the Society of Neurointerventional Surgery. J. Neurointerv. Surg. 2017, 9, 802–812. [Google Scholar] [CrossRef]
- Fiehler, J.; Cognard, C.; Gallitelli, M.; Jansen, O.; Kobayashi, A.; Heinrich, P.; Mattle, H.P.; Keith, W.; Muir, K.W.; Mikael Mazighi, M.; et al. European Recommendations on Organisation of Interventional Care in Acute Stroke (EROICAS). Int. J. Stroke 2016, 11, 701–716. [Google Scholar] [CrossRef]
- Ruiz, J.G.; Mintzer, M.J.; Leipzig, R.M. The impact of e-learning in medical education. Acad Med. 2006, 81, 207–212. [Google Scholar] [CrossRef]
- Kirkpatrick, D.L. Evaluating Training Programs. The Four Levels; Berrett-Koehler: Philadelphia, PA, USA, 1998. [Google Scholar]
- Acker, J.E.; Pancioli, A.M.; Crocco, T.J.; Eckstein, M.K.; Jauch, E.C.; Larrabee, H.; Meltzer, N.M.; Mergendahl, W.C.; Munn, J.W.; Prentiss, S.M.; et al. Implementation strategies for emergency medical services within stroke systems of care: A policy statement from the American Heart Association/American Stroke Association expert panel on emergency medical services systems and the stroke council. Stroke 2007, 38, 3097–3115. [Google Scholar] [CrossRef]
- King’s College London. The Burden of Stroke in Europe. London. 2017. Available online: http://www.strokeeurope.eu/downloads/TheBurdenOfStrokeInEuropeReport.pdf (accessed on 29 October 2018).
- Hsieh, H.-C.; Hsieh, C.-Y.; Lin, C.-H.; Sung, P.-S.; Li, C.-Y.; Chi, C.-H.; Chen, C.H. Development of an Educational Program for Staffs of Emergency Medical Service to Improve Their Awareness of Stroke within 3 Hours of Symptom Onset: A Pilot Study. Acta Neurol. Taiwan 2013, 22, 4–12. [Google Scholar] [PubMed]
- Shire, F.; Kasim, Z.; Alrukn, S.; Khan, M. Stroke awareness among Dubai emergency medical service staff and impact of an educational intervention. BMC Res. Notes 2017, 10, 255. [Google Scholar] [CrossRef] [PubMed]
- DiBiasio, E.L.; Jayaraman, M.V.; Oliver, L.; Paolucci, G.; Clark, M.; Watkins, C.; DeLisi, K.; Wilks, A.; Yaghi, S.; Morgan Hemendinger, M.; et al. Emergency medical systems education may improve knowledge of pre-hospital stroke triage protocols. J. Neurointerv. Surg. 2020, 12, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.P.; Miller, C.; Gibson, J.M.E.; Cook, J.; Price, C.; Watkins, C.L. The impact of education and training interventions for nurses and other health care staff involved in the delivery of stroke care: An integrative review. Nurse Educ. Today 2017. [Google Scholar] [CrossRef]
- Jones, S.; McLoughlin, A.; Watkins, C. Acute stroke management: An online course. J. Paramed. Pract. 2011, 3, 322–327. [Google Scholar] [CrossRef]
- Oostema, J.A.; Nasiri, M.; Chassee, T.; Reeves, M.J. The quality of prehospital ischemic stroke care: Compliance with guidelines and impact on in-hospital stroke response. J. Stroke Cerebrovasc. Dis. 2014, 23, 2773–2779. [Google Scholar] [CrossRef]
- Oostema, J.A.; Chassee, T.; Baer, W.; Edberg, A.; Reeves, M.J. Brief Educational Intervention Improves Emergency Medical Services Stroke Recognition. Stroke 2019, 50, 1193–1200. [Google Scholar] [CrossRef]
- Bae, H.J.; Kim, D.H.; Yoo, N.T.; Choi, J.H.; Huh, J.T.; Cha, J.K.; Kim, S.K.; Choi, J.S.; Kim, J.W. Prehospital notification from the emergency medical service reduces the transfer and intra-hospital processing times for acute stroke patients. J. Clin. Neurol. 2010, 6, 138–142. [Google Scholar] [CrossRef]
- Mckinney, J.S.; Mylavarapu, K.; Lane, J.; Roberts, V.; Ohman-Strickland, P.; Merlin, M.A. Hospital prenotification of stroke patients by emergency medical services improves stroke time targets. J. Stroke Cerebrovasc. Dis. 2013, 22. [Google Scholar] [CrossRef]
- Teleb, M.S.; Ver Hage, A.; Carter, J.; Jayaraman, M.V.; McTaggart, R.A. Stroke vision, aphasia, neglect (VAN) assessment-a novel emergent large vessel occlusion screening tool: Pilot study and comparison with current clinical severity indices. J. Neurointerv. Surg. 2017, 9, 122–126. [Google Scholar] [CrossRef]
- Schlemm, L.; Ebinger, M.; Nolte, C.H.; Endres, M. Impact of prehospital triage scales to detect large vessel occlusion on resource utilization and time to treatment. Stroke 2018, 49, 439–446. [Google Scholar] [CrossRef]
- Noorian, A.R.; Sanossian, N.; Shkirkova, K.; Liebeskind, D.S.; Eckstein, M.; Stratton, S.J.; Pratt, F.D.; Conwit, R.; Chatfield, F.; Sharma, L.K.; et al. Los Angeles Motor Scale to identify large vessel occlusion: Prehospital validation and comparison with other screens. Stroke 2018, 49, 565–572. [Google Scholar] [CrossRef]
- American Heart Association. American Heart Association Mission Lifeline: Stroke Severity-Based Stroke Triage Algorithm for EMS. 2018. Available online: https://www.heart.org/HEARTORG/Professional/MissionLifelineHomePage/MissionLifeline-Stroke_UCM_491623_SubHomePage.jsp (accessed on 26 December 2019).
- Ahmed, N.; Steiner, T.; Caso, V.; Wahlgren, N. ESO-KSU session participants. Recommendations from the ESO-Karolinska Stroke Update Conference, Stockholm, 13–15 November 2016. Eur Stroke J. 2017, 2, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, 344–418. [Google Scholar] [CrossRef]
- Jumaa, M.A.; Castonguay, A.C.; Salahuddin, H.; Shawver, J.; Saju, L.; Burgess, R.; Kung, V.; Slawski, D.E.; Tietjen, G.; Parquette, B.; et al. Long-term implementation of a prehospital severity scale for EMS triage of acute stroke: A real-world experience. J. NeuroIntervent. Surg. 2020, 12, 19–24. [Google Scholar] [CrossRef]
- Bray, J.E.; Martin, J.; Cooper, G.; Barger, B.; Bernard, S.; Bladin, C. An interventional study to improve paramedic diagnosis of stroke. Prehosp. Emerg. Care 2005, 9, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Price, C.I.; Shaw, L.; Dodd, P.; Exley, C.; Flynn, D.; Francis, R.; Islam, S.; Javanbakht, M.; Lakey, R.; Lally, J.; et al. Paramedic Acute Stroke Treatment Assessment (PASTA): Study protocol for a randomised controlled trial. Trials 2019, 20, 121. [Google Scholar] [CrossRef] [PubMed]
- Watkins, C.L.; Leathley, M.J.; Jones, S.P.; Ford, G.A.; Quinn, T.; Chris, J.; Sutton, C.J. Training emergency services’ dispatchers to recognise stroke: An interrupted time-series analysis. BMC Health Serv. Res. 2013, 13, 318. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Topics | Baseline (n = 1968) | After Training (n = 1506) | p-Value |
|---|---|---|---|
| (% Correct) | (% Correct) | (* <0.05) | |
| Signs and symptoms of a stroke | 1960 (99.6) | 1500 (99.7) | 0.97 |
| Ischemic stroke etiology | 1934 (98.3) | 1483 (98.5) | 0.645 |
| Hemorrhagic stroke etiology | 1891 (96.1) | 1491 (99.1) | <0.001 * |
| Left hemisphere stroke signs/symptoms | 1029 (5.2) | 925 (61.4) | <0.001 * |
| Right hemispheres stroke signs/symptoms | 267 (13.7) | 615 (40.9) | <0.001 * |
| Transient ischemic attack definition | 1272 (64.6) | 1024 (68.0) | 0.038 * |
| Brainstem stroke signs/symptoms | 1245 (63.2) | 1240 (82.3) | <0.001 * |
| Window for thrombolysis | 689 (35.0) | 774 (51.4) | <0.001 * |
| Endovascular indications | 974 (49.5) | 1022 (67.9) | <0.001 * |
| Benefits of stroke treatment | 1027 (52.2) | 1209 (80.3) | <0.001 * |
| Aim of the stroke code | 1833 (93.1) | 1446 (96.0) | <0.001 * |
| Target age for the stroke code | 1510 (76.7) | 1430 (95.0) | <0.001 * |
| Time criteria from onset to code activation | 1247 (63.3) | 1322 (87.8) | <0.001 * |
| Criteria for activation of the stoke code | 1251 (63.6) | 1341 (89.1) | <0.001 * |
| Recognition of comorbidity scales | 403 (40.1) | 906 (60.2) | <0.001 * |
| Recognition of stroke diagnostic scales | 1186 (50.3) | 1393 (92.5) | <0.001 * |
| RAPID 1 scale recognition | 1033 (52.5) | 1236 (82.1) | <0.001 * |
| RANCOM 2 scale recognition | 1616 (82.1) | 1390 (92.3) | <0.001 * |
| Hypertension and nausea | 1298 (65.9) | 961 (63.8) | 0.189 |
| Transient ischemic attack | 1534 (77.9) | 1277 (84.8) | <0.001 * |
| 90 years. 5 h start of symptoms | 1515 (77.0) | 1364 (90.6) | <0.001 * |
| Treatment with anticoagulants | 1560 (79.3) | 1288 (85.5) | <0.001 * |
| Awakening stroke | 1644 (83.5) | 1430 (95.0) | <0.001 * |
| RANCOM 2 scale | 1309 (66.5) | 1145 (76.0) | <0.001 * |
| Item | Baseline (2014) | Immediately after Training (2014 Q4) | Immediately after Training (2014 Q4) | 1–2 Years after Training (2015–2016) | 1–2 Years after Training (2015–2016) | 3–4 Years after Training (2017–2018) | |||
|---|---|---|---|---|---|---|---|---|---|
| n = 834 | n = 965 | n = 965 | n = 7261 | n = 7261 | n = 8075 | ||||
| n (%) | n (%) | p-Value | n (%) | n (%) | p-Value | n (%) | n (%) | p-Value | |
| Patient identification no. | 460 (55.2%) | 632 (65.5%) | <0.001 * | 632 (65.5%) | 4998 (68.8%) | 0.036 * | 4998 (68.8%) | 6904 (85.5%) | <0.001 * |
| Time from onset of symptoms | 714 (85.6%) | 759 (78.7%) | <0.001 * | 759 (78.7%) | 5305 (73.1%) | <0.001 * | 5305 (73.1%) | 6211 (76.9%) | <0.001 * |
| Anticoagulant therapy | 704 (84.4%) | 809 (83.8%) | 0.738 | 809 (83.8%) | 6237 (85.9%) | 0.086 | 6237 (85.9%) | 6327 (78.3%) | <0.001 * |
| Glycaemia | 246 (29.5%) | 672 (69.6%) | <0.001 * | 672 (69.6%) | 4922 (67.8%) | 0.247 | 4922 (67.8%) | 6524 (80.8%) | <0.001 * |
| Systolic blood pressure | 255 (30.6%) | 711 (73.7%) | <0.00 1* | 711 (73.7%) | 5043 (69.5%) | 0.009 * | 5043 (69.5%) | 7007 (86.8%) | <0.001 * |
| Diastolic blood pressure | 254 (30.5%) | 711 (73.7%) | <0.001 * | 711 (73.7%) | 5044 (69.5%) | 0.007 * | 5044 (69.5%) | 6516 (80.7%) | <0.001 * |
| RACE scores | --------------- | 588 (60.9%) | 588 (60.9%) | 5165 (71.1%) | <0.001 * | 5165 (71.1%) | 7350 (91.0) | <0.001 * |
| Item | Baseline (2014 Q1) n = 834 | Immediately after Training (2014 Q4) n = 965 | 1–2 Years after Training (2015–2016) n = 7261 | 3–4 Years after Training (2017–2018) n = 8075 | 95%CI of the Difference | p-Value |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||
| Alert time 1 | 3.10 (6.7) | 2.96 (5.6) | 2.90 (5.8) | 3.13 (6.1) | −0.25 to 0.56 | 0.877 |
| Activation time 2 | 4.78 (7.1) | 4.97 (6.7) | 4.86 (7.0) | 5.35 (7.6) | −1.64 to 0.73 | 0.053 |
| Response time 3 | 8.08 (4.9) | 8.68 (5.3) | 8.57 (5.6) | 8.70 (6.0) | −0.34 to 1.23 | 0.083 |
| Clinical care time 4 | 21.51 (8.4) | 21.87 (8.3) | 22.24 (8.9) | 24.32 (8.9) | 0.75 to 3.27 | 0.034 * |
| Transfer time 5 | 12.29 (10.1) | 13.11 (10.6) | 12.73 (10.3) | 12.86 (11.2) | −1.51 to 1.66 | 0.402 |
| Overall time 6 | 48.9 (19.9) | 51.60 (19.5) | 51.52 (19.6) | 53.62 (20.0) | 1.04 to 5.33 | 0.015 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorchs-Molist, M.; Solà-Muñoz, S.; Enjo-Perez, I.; Querol-Gil, M.; Carrera-Giraldo, D.; Nicolàs-Arfelis, J.M.; Jiménez-Fàbrega, F.X.; Pérez de la Ossa, N. An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals. Int. J. Environ. Res. Public Health 2020, 17, 6183. https://doi.org/10.3390/ijerph17176183
Gorchs-Molist M, Solà-Muñoz S, Enjo-Perez I, Querol-Gil M, Carrera-Giraldo D, Nicolàs-Arfelis JM, Jiménez-Fàbrega FX, Pérez de la Ossa N. An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals. International Journal of Environmental Research and Public Health. 2020; 17(17):6183. https://doi.org/10.3390/ijerph17176183
Chicago/Turabian StyleGorchs-Molist, Montse, Silvia Solà-Muñoz, Iago Enjo-Perez, Marisol Querol-Gil, David Carrera-Giraldo, Jose María Nicolàs-Arfelis, Francesc Xavier Jiménez-Fàbrega, and Natalia Pérez de la Ossa. 2020. "An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals" International Journal of Environmental Research and Public Health 17, no. 17: 6183. https://doi.org/10.3390/ijerph17176183
APA StyleGorchs-Molist, M., Solà-Muñoz, S., Enjo-Perez, I., Querol-Gil, M., Carrera-Giraldo, D., Nicolàs-Arfelis, J. M., Jiménez-Fàbrega, F. X., & Pérez de la Ossa, N. (2020). An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals. International Journal of Environmental Research and Public Health, 17(17), 6183. https://doi.org/10.3390/ijerph17176183