Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status


 ,
,  , ,
, ,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach
2.2. Participants
2.3. Urine Sampling
2.4. Biochemical Determinations
2.5. Statistical Analysis
3. Results
3.1. Physical Activity Modifies Hydration Status in Professional Athletes
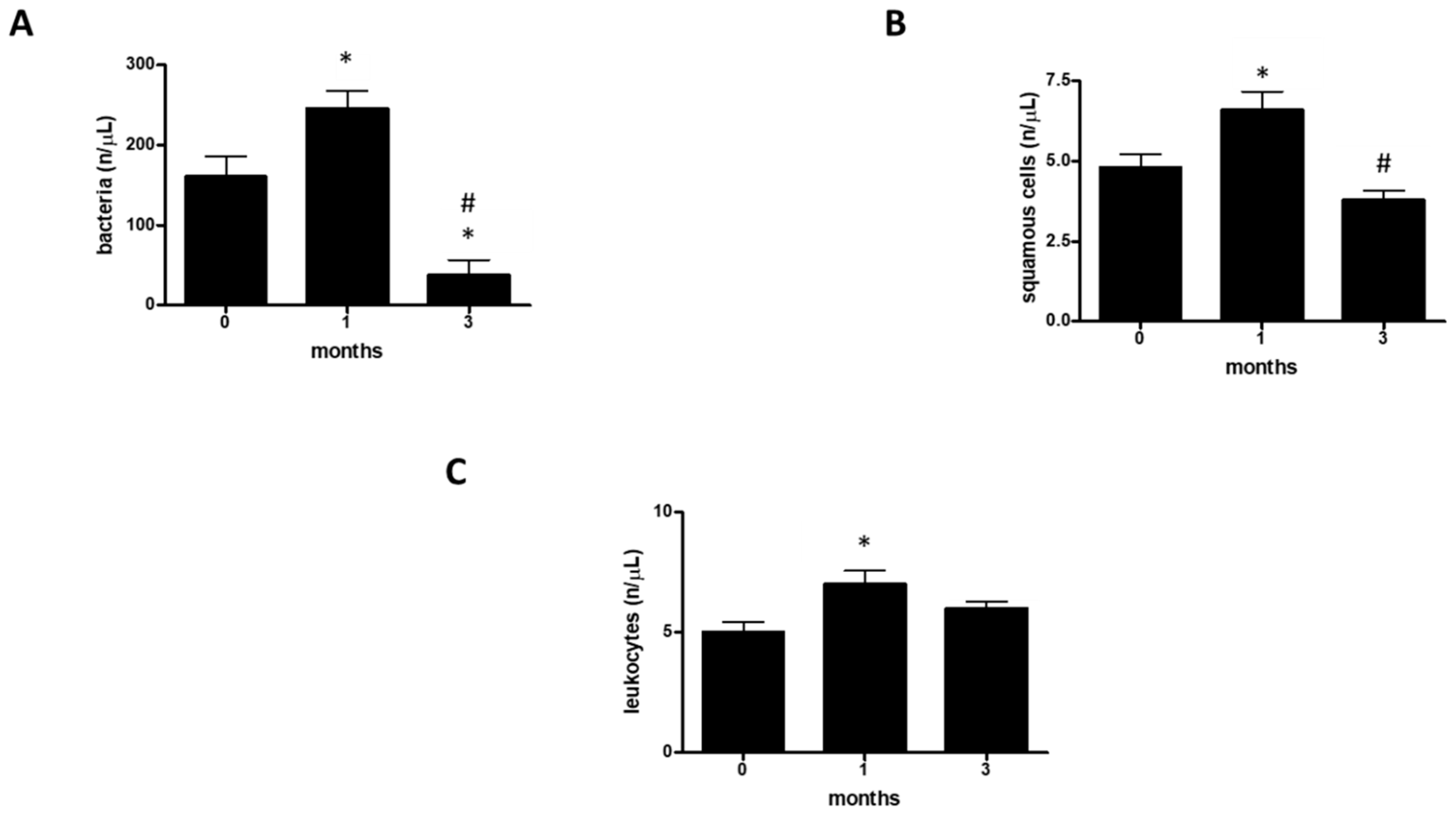
3.2. Physical Activity Modifies Susceptibility to Urinary Infections
3.3. Physical Activity Modifies Hematuria and Proteinuria in Professional Athletes
3.4. Physical Activity Does Not Affect Urinary Parameters in Professional Athletes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lombardo, B.; Izzo, V.; Terracciano, D.; Ranieri, A.; Mazzaccara, C.; Fimiani, F.; Cesaro, A.; Gentile, L.; Leggiero, E.; Pero, R.; et al. Laboratory medicine: Health evaluation in elite athletes. Clin. Chem. Lab. Med. 2019, 57, 1450–1473. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Wagener, G.; Zhu, Y.; Wang, S.; Lee, H.T. Urinary Biomarkers in the Early Detection of Acute Kidney Injury after Cardiac Surgery. Clin. J. Am. Soc. Nephrol. 2009, 4, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S. Biomarkers of cardiovascular disease molecular basis and practical considerations. Circulation 2006, 113, 2335–2362. [Google Scholar] [CrossRef] [PubMed]
- Poste, G. Bring on the biomarkers. Nature 2011, 469, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Update on hypothetical model of Alzheimer’s disease biomarkers. Lancet Neurol. 2013, 12, 207. [Google Scholar] [CrossRef] [Green Version]
- Papa, L.; Ramia, M.M.; Edwards, D.; Johnson, B.D.; Slobounov, S.M. Systematic Review of Clinical Studies Examining Biomarkers of Brain Injury in Athletes after Sports-Related Concussion. J. Neurotrauma 2015, 32, 661–673. [Google Scholar] [CrossRef] [Green Version]
- Finsterer, J. Biomarkers of peripheral muscle fatigue during exercise. BMC Musculoskelet. Disord. 2012, 13, 218. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.-A.; Park, K.D.; Ahn, J.; Park, Y.-B.; Kim, Y.-J. Comparison of Changes in Biochemical Markers for Skeletal Muscles, Hepatic Metabolism, and Renal Function after Three Types of Long-distance Running: Observational Study. Medicine 2016, 95, e3657. [Google Scholar] [CrossRef]
- Ragozzino, E.; Brancaccio, M.; Di Costanzo, A.; Scalabrì, F.; Andolfi, G.; Wanderlingh, L.G.; Patriarca, E.J.; Minchiotti, G.; Altamura, S.; Summa, V.; et al. 6-Bromoindirubin-3′-oxime intercepts GSK3 signaling to promote and enhance skeletal muscle differentiation affecting miR-206 expression in mice. Sci. Rep. 2019, 9, 1–17. [Google Scholar] [CrossRef]
- Querques, F.; Cantilena, B.; Cozzolino, C.; Esposito, M.T.; Passaro, F.; Parisi, S.; Lombardo, B.; Russo, T.; Pastore, L. Angiotensin receptor I stimulates osteoprogenitor proliferation through TGFβ-mediated signaling. J. Cell. Physiol. 2015, 230, 1466–1474. [Google Scholar] [CrossRef]
- Kirkland, E.B.; Adams, B.B. Methicillin-resistant Staphylococcus aureus and athletes. J. Am. Acad. Dermatol. 2008, 59, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Scudiero, O.; Brancaccio, M.; Mennitti, C.; Laneri, S.; Lombardo, B.; De Biasi, M.G.; De Gregorio, E.; Pagliuca, C.; Colicchio, R.; Salvatore, P.; et al. Human Defensins: A Novel Approach in the Fight against Skin Colonizing Staphylococcus aureus. Antibiotics 2020, 9, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, A.; Delgado, L.; Moreira, P.; Haahtela, T. Does exercise increase the risk of upper respiratory tract infections? Br. Med. Bull. 2009, 90, 111–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaccarino, G.; Trimarco, B. Gene-environment interactions and vitamin D effects on cardiovascular risk. BMC Med. 2019, 17, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hull, C.M.; Harris, J.A. Venous Thromboembolism and Marathon Athletes. Circulation 2013, 128, e469–e471. [Google Scholar] [CrossRef]
- Girolami, F.; Frisso, G.; Benelli, M.; Crotti, L.; Iascone, M.; Mango, R.; Mazzaccara, C.; Pilichou, K.; Arbustini, E.; Tomberli, B.; et al. Contemporary genetic testing in inherited cardiac disease. J. Cardiovasc. Med. 2018, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Detta, N.; Frisso, G.; Limongelli, G.; Marzullo, M.; Calabrŏ, R.; Salvatore, F. Genetic analysis in a family affected by sick sinus syndrome may reduce the sudden death risk in a young aspiring competitive athlete. Int. J. Cardiol. 2014, 170, e63–e65. [Google Scholar] [CrossRef] [Green Version]
- Zebisch, A.; Schulz, E.; Grosso, M.; Lombardo, B.; Acierno, G.; Sill, H.; Iolascon, A. Identification of a novel variant of epsilon-gamma-delta-beta thalassemia highlights limitations of next generation sequencing. Am. J. Hematol. 2015, 90, E52–E54. [Google Scholar] [CrossRef]
- Hughes, R.L. A Review of the Role of the Gut Microbiome in Personalized Sports Nutrition. Front. Nutr. 2019, 6, 191. [Google Scholar] [CrossRef]
- Coretti, L.; Cuomo, M.; Florio, E.; Palumbo, D.; Keller, S.; Pero, R.; Chiariotti, L.; Lembo, F.; Cafiero, C. Subgingival dysbiosis in smoker and non-smoker patients with chronic periodontitis. Mol. Med. Rep. 2017, 15, 2007–2014. [Google Scholar] [CrossRef] [Green Version]
- Keller, S.; Angrisano, T.; Florio, E.; Pero, R.; Decaussin-Petrucci, M.; Troncone, G.; Capasso, M.; Lembo, F.; Fusco, A.; Chiariotti, L. DNA methylation state of the galectin-3 gene represents a potential new marker of thyroid malignancy. Oncol. Lett. 2013, 6, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Coretti, L.; Natale, A.; Cuomo, M.; Florio, E.; Keller, S.; Lembo, F.; Chiariotti, L.; Pero, R. The Interplay between Defensins and Microbiota in Crohn’s Disease. Mediat. Inflamm. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.; Errico, F.; Zarrilli, F.; Florio, E.; Punzo, D.; Mansueto, S.; Angrisano, T.; Pero, R.; Lembo, F.; Castaldo, G.; et al. DNA methylation state of BDNF gene is not altered in prefrontal cortex and striatum of schizophrenia subjects. Psychiatry Res. 2014, 220, 1147–1150. [Google Scholar] [CrossRef] [PubMed]
- Angrisano, T.; Pero, R.; Brancaccio, M.; Coretti, L.; Florio, E.; Pezone, A.; Calabrò, V.; Falco, G.; Keller, S.; Lembo, F.; et al. Cyclical DNA Methylation and Histone Changes Are Induced by LPS to Activate COX-2 in Human Intestinal Epithelial Cells. PLoS ONE 2016, 11, e0156671. [Google Scholar] [CrossRef] [PubMed]
- Chiariotti, L.; Coretti, L.; Pero, R.; Lembo, F. Epigenetic Alterations Induced by Bacterial Lipopolysaccharides. Adv. Exp. Med. Biol. 2016, 879, 91–105. [Google Scholar] [CrossRef]
- Pero, R.; Brancaccio, M.; Laneri, S.; De Biasi, M.G.; Lombardo, B.; Scudiero, O. A Novel View of Human Helicobacter pylori Infections: Interplay between Microbiota and Beta-Defensins. Biomolecules 2019, 9, 237. [Google Scholar] [CrossRef] [Green Version]
- Pero, R.; Coretti, L.; Nigro, E.; Lembo, F.; Laneri, S.; Lombardo, B.; Daniele, A.; Scudiero, O. β-Defensins in the Fight against Helicobacter pylori. Molecules 2017, 22, 424. [Google Scholar] [CrossRef]
- Colavita, I.; Nigro, E.; Sarnataro, D.; Scudiero, O.; Granata, V.; Daniele, A.; Zagari, A.; Pessi, A.; Salvatore, F. Membrane protein 4F2/CD98 is a cell surface receptor involved in the internalization and trafficking of human β-Defensin 3 in epithelial cells. Chem. Biol. 2015, 2, 217–228. [Google Scholar] [CrossRef] [Green Version]
- Falanga, A.; Valiante, S.; Galdiero, E.; Franci, G.; Scudiero, O.; Morelli, G.; Galdiero, M. Dimerization in tailoring uptake efficacy of the HSV-1 derived membranotropic peptide gH625. Sci. Rep. 2017, 7, 9434. [Google Scholar] [CrossRef] [Green Version]
- Nigro, E.; Colavita, I.; Sarnataro, D.; Scudiero, O.; Zambrano, G.; Granata, V.; Daniele, A.; Carotenuto, A.; Galdiero, S.; Folliero, V.; et al. An ancestral host defence peptide within human β-defensin 3 recapitulates the antibacterial and antiviral activity of the full-length molecule. Sci. Rep. 2015, 5, 18450. [Google Scholar] [CrossRef] [Green Version]
- Djaoui, L.; Haddad, M.; Chamari, K.; Dellal, A. Monitoring training load and fatigue in soccer players with physiological markers. Physiol. Behav. 2017, 181, 86–94. [Google Scholar] [CrossRef] [PubMed]
- McTaggart, M.P.; Lindsay, F.J.; Kearney, F.E.M. Replacing Urine Protein Electrophoresis With Serum Free Light Chain Analysis as a First-Line Test for Detecting Plasma Cell Disorders Offers Increased Diagnostic Accuracy and Potential Health Benefit to Patients. Am. J. Clin. Pathol. 2013, 140, 890–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samudrala, D.; Geurts, B.; Brown, P.A.; Szymańska, E.; Mandon, J.; Jansen, J.; Buydens, L.; Harren, F.F.; Cristescu, S.M. Changes in urine headspace composition as an effect of strenuous walking. Metabolomics 2015, 11, 1656–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Kim, J. Urinary proteomics and metabolomics studies to monitor bladder health and urological diseases. BMC Urol. 2016, 16, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladell, W.S.S. The effects of water and salt intake upon the performance of men working in hot and humid environments. J. Physiol. 1955, 127, 11–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.C.; Fragala, M.S.; Kavouras, S.A.; Queen, R.M.; Pryor, J.L.; Casa, D.J. Biomarkers in Sports and Exercise: Tracking Health, Performance, and Recovery in Athletes. J. Strength Cond. Res. 2017, 31, 2920–2937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, G.; Lin, W.; McAinch, A.J.; Yan, X.; Weng, X. Identification of Urinary Biomarkers for Exercise-Induced Immunosuppression by iTRAQ Proteomics. BioMed Res. Int. 2020, 2020, 3030793. [Google Scholar] [CrossRef] [Green Version]
- Montain, S.J.; Coyle, E.F. Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. J. Appl. Physiol. 1992, 73, 1340–1350. [Google Scholar] [CrossRef]
- Pitts, G.C.; Johnson, R.E.; Consolazio, F.C. Work in the heat as affected by intake of water, salt and glucose. Am. J. Physiol. Content 1944, 142, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Sawka, M.N.; Francesconi, R.P.; Young, A.J.; Pandolf, K.B. Influence of Hydration Level and Body Fluids on Exercise Performance in the Heat. JAMA 1984, 252, 1165. [Google Scholar] [CrossRef]
- Svendsen, I.S.; Gleeson, M.; Haugen, T.A.; Tønnessen, E. Effect of an intense period of competition on race performance and self-reported illness in elite cross-country skiers. Scand. J. Med. Sci. Sports 2015, 25, 846–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieman, D. Is infection risk linked to exercise workload? Med. Sci. Sports Exerc. 2000, 32, S406–S411. [Google Scholar] [CrossRef] [PubMed]
- Hellard, P.; Avalos, M.; Guimaraes, F.; Toussaint, J.-F.; Pyne, D.B. Training-Related Risk of Common Illnesses in Elite Swimmers over a 4-yr Period. Med. Sci. Sports Exerc. 2015, 47, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Dielubanza, E.J.; Schaeffer, A.J. Urinary Tract Infections in Women. Med. Clin. 1998, 25, 685–701. [Google Scholar] [CrossRef]
- Neugent, M.L.; Hulyalkar, N.V.; Nguyen, V.H.; Zimmern, P.E.; De Nisco, N.J. Advances in Understanding the Human Urinary Microbiome and Its Potential Role in Urinary Tract Infection. mBio 2020, 11, 1–15. [Google Scholar] [CrossRef]
- Ahmadinejad, Z.; Alijani, N.; Mansori, S.; Ziaee, V. Common Sports-Related Infections: A Review on Clinical Pictures, Management and Time to Return to Sports. Asian J. Sports Med. 2014, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wagenlehner, F.M.E.; Naber, K.G. Urinary Tract Infections—General. Antimicrobe. Available online: http://www.antimicrobe.org/e4a.asp (accessed on 19 August 2020).
- Lewis, A.J.; Richards, A.C.; Mulvey, M. Invasion of Host Cells and Tissues by Uropathogenic Bacteria. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Khasriya, R.; Sathiananthamoorthy, S.; Ismail, S.; Kelsey, M.; Wilson, M.; Rohn, J.L.; Malone-Lee, J. Spectrum of Bacterial Colonization Associated with Urothelial Cells from Patients with Chronic Lower Urinary Tract Symptoms. J. Clin. Microbiol. 2013, 51, 2054–2062. [Google Scholar] [CrossRef] [Green Version]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Jaworski, C.A.; Rygiel, V. Acute Illness in the Athlete. Clin. Sports Med. 2019, 38, 577–595. [Google Scholar] [CrossRef]
- Orenstein, R.; Wong, E.S. Urinary tract infections in adults. Am. Fam. Physician 1999, 59, 1225–1234. [Google Scholar] [PubMed]
- Lindsay, E.N. Prophylaxis: Recurrent infections in women. Infection 1992, 20, S203–S205. [Google Scholar]
- Kuo, H.-C.; Jhang, J.-F. Recent advances in recurrent urinary tract infection from pathogenesis and biomarkers to prevention. Ci Ji Yi Xue Za Zhi 2017, 29, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLellan, L.; Hunstad, D.A. Urinary Tract Infection: Pathogenesis and Outlook. Trends Mol. Med. 2016, 22, 946–957. [Google Scholar] [CrossRef] [Green Version]
- Irving, R.; Noakes, T.D.; Van Zyl-Smit, R.; Irving, G. The Immediate and Delayed Effects of Marathon Running on Renal function. J. Urol. 1986, 136, 1176–1180. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Rampaer, L.; Wolfs, J.-C. Renal protein excretion after exercise in man. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 58, 476–480. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Labilloy, D. The influence of work intensity on post-exercise proteinuria. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 57, 260–263. [Google Scholar] [CrossRef]
- Groop, L.; Stenman, S.; Groop, P.H.; Makipernaa, A.; Teppo, A.M. The effect of exercise on urinary excretion of different size proteins in patients with ins μL in-dependent diabetes mellitus. Scand. J. Clin. Lab. Investig. 1990, 50, 525–532. [Google Scholar] [CrossRef]
- Cruz, H.M.; Cruz, J.; Castro, M.C.; Marcondes, M. Effect of posture and physical activity on urinary protein excretion by patients with glomerular proteinuria diseases. Braz. J. Med. Biol. Res. 1989, 22, 1191–1194. [Google Scholar]
- Poortmans, J.R.; Hermans, L.; Vandervliet, A.; Niset, G.; Godefroid, C. Renal responses to exercise in heart and kidney transplant patients. Transpl. Int. 1997, 10, 323–327. [Google Scholar] [CrossRef]
- Tietze, D.C.; Borchers, J. Exertional Rhabdomyolysis in the Athlete: A Clinical Review. Sports Health 2014, 6, 336–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Lee, J.; Kim, S.; Ryu, H.Y.; Cha, K.S.; Sung, D.J. Exercise-induced rhabdomyolysis mechanisms and prevention: A literature review. J. Sport Health Sci. 2016, 5, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariani, A.J.; Mariani, M.C.; Macchioni, C.; Stams, U.K.; Hariharan, A.; Moriera, A. The Significance of Adult Hematuria: 1,000 Hematuria Evaluations Including a Risk-Benefit and Cost-Effectiveness Analysis. J. Urol. 1989, 141, 350–355. [Google Scholar] [CrossRef]
- Jones, G.R.; Newhouse, I. Sport-Related Hematuria: A Review. Clin. J. Sport Med. 1997, 7, 119–125. [Google Scholar] [CrossRef]
- Zbgniew, S. Erythrocytic system under the influence of physical exercise and training. Sports Med. 1990, 10, 181–197. [Google Scholar]
- Sjödin, B.; Westing, Y.H.; Apple, F.S. Biochemical Mechanisms for Oxygen Free Radical Formation During Exercise. Sports Med. 1990, 10, 236–254. [Google Scholar] [CrossRef] [PubMed]
- Faraonio, R.; Vergara, P.; Di Marzo, D.; Napolitano, M.; Russo, T.; Cimino, F.; Cimino, F. Transcription Regulation in NIH3T3 Cell Clones Resistant to Diethylmaleate-Induced Oxidative Stress and Apoptosis. Antioxid. Redox Signal. 2006, 8, 365–374. [Google Scholar] [CrossRef]
- Bergey, D.H.; Holt, J.G. Bergey’s Manual of Determinative Bacteriology, 9th ed.; Williams & Wilkins: Baltimora, MD, USA, 1994. [Google Scholar]
- Barcella, L.; Barbaro, A.P.; Rogolino, S.B. Colonial morphology of Escherichia coli: Impact of detection in clinical specimens. Microbiol. Med. 2016, 31, 2. [Google Scholar] [CrossRef] [Green Version]
- Baker, S.B. The Blood Supply of the Renal Papilla. Br. J. Urol. 1959, 31, 53–59. [Google Scholar] [CrossRef]
- Mennitti, C.; Brancaccio, M.; Gentile, L.; Ranieri, A.; Terracciano, D.; Cennamo, M.; La Civita, E.; Liotti, A.; D’Alicandro, G.; Mazzaccara, C.; et al. Athlete’s Passport: Prevention of Infections, Inflammations, Injuries and Cardiovascular Diseases. J. Clin. Med. 2020, 9, 2540. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Values | 0 Months | 1 Months | 3 Months |
|---|---|---|---|---|
| pH | ≥5 | 50% | 31% | 59% |
| ≥6 | 33% | 38% | 8% | |
| ≥7 | 17% | 31% | 33% | |
| Specific Weight | ≥1005 | 10% | 10% | |
| ≥1018 | 50% | 60% | 50% | |
| ≥1030 | 40% | 30% | 50% | |
| Color | Amber | 8% | 17% | |
| Straw yellow | 92% | 83% | 100% | |
| Appearance | Clear | 83% | 75% | 100% |
| Opalescent | 9% | 8% | ||
| Turbid | 8% | 17% |
| Parameters | Values | 0 Months | 1 Months | 3 Months |
|---|---|---|---|---|
| Bacteria | 0–200 n/µL | 83% | 67% | 100% |
| 201–500 n/µL | 9% | 8% | ||
| 501–1000 n/µl | 8% | 25% | ||
| Squamous Cells | 0–5 n/μL | 75% | 50% | 75% |
| 6–10 n/µL | 8% | 25% | 17% | |
| 11–20 n/μL | 17% | 25% | 8% | |
| Leucocytes | 0–4 n/μL | 58% | 50% | 67% |
| 5–9 n/µL | 17% | 8% | 8% | |
| 10–18 n/µL | 25% | 42% | 25% |
| Parameters | Values | 0 Months | 1 Months | 3 Months |
|---|---|---|---|---|
| Erythrocytes | 0–3 n/μL | 50% | 50% | 75% |
| 4–7 n/μL | 33% | 25% | 17% | |
| 8–14 n/μL | 17% | 25% | 8% | |
| Protein | 0–15 mg/dL | 75% | 75% | 75% |
| 16–50 mg/dL | 17% | 8% | 25% | |
| 51–100 mg/dL | 8% | 17% |
| Variables | 0 Months | 1 Month | 3 Months |
|---|---|---|---|
| Glucose | absent | absent | Absent |
| Ketones | negative | negative | Negative |
| Bilirubin | absent | absent | Absent |
| Hemoglobin | absent | absent | Absent |
| Nitrite | absent | absent | Absent |
| Leukocyte esterase | absent | absent | Absent |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pero, R.; Brancaccio, M.; Mennitti, C.; Gentile, L.; Arpino, S.; De Falco, R.; Leggiero, E.; Ranieri, A.; Pagliuca, C.; Colicchio, R.; et al. Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status. Int. J. Environ. Res. Public Health 2020, 17, 6065. https://doi.org/10.3390/ijerph17176065
Pero R, Brancaccio M, Mennitti C, Gentile L, Arpino S, De Falco R, Leggiero E, Ranieri A, Pagliuca C, Colicchio R, et al. Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status. International Journal of Environmental Research and Public Health. 2020; 17(17):6065. https://doi.org/10.3390/ijerph17176065
Chicago/Turabian StylePero, Raffaela, Mariarita Brancaccio, Cristina Mennitti, Luca Gentile, Sergio Arpino, Renato De Falco, Eleonora Leggiero, Annaluisa Ranieri, Chiara Pagliuca, Roberta Colicchio, and et al. 2020. "Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status" International Journal of Environmental Research and Public Health 17, no. 17: 6065. https://doi.org/10.3390/ijerph17176065
APA StylePero, R., Brancaccio, M., Mennitti, C., Gentile, L., Arpino, S., De Falco, R., Leggiero, E., Ranieri, A., Pagliuca, C., Colicchio, R., Salvatore, P., D’Alicandro, G., Frisso, G., Lombardo, B., Mazzaccara, C., Faraonio, R., & Scudiero, O. (2020). Urinary Biomarkers: Diagnostic Tools for Monitoring Athletes’ Health Status. International Journal of Environmental Research and Public Health, 17(17), 6065. https://doi.org/10.3390/ijerph17176065