Self-Acceptance and Interdependence Promote Longevity: Evidence From a 20-year Prospective Cohort Study


Abstract
1. Introduction
1.1. Self-Acceptance, Longevity Expectation, Longevity
1.2. Interdependence, Serenity towards Death, Longevity
1.3. Potential Confounders
1.4. Present Study
2. Materials and Methods
2.1. Data and Participants
2.2. Measures
2.3. Analytic Strategy
3. Results
3.1. Confirmatory Factor Analysis
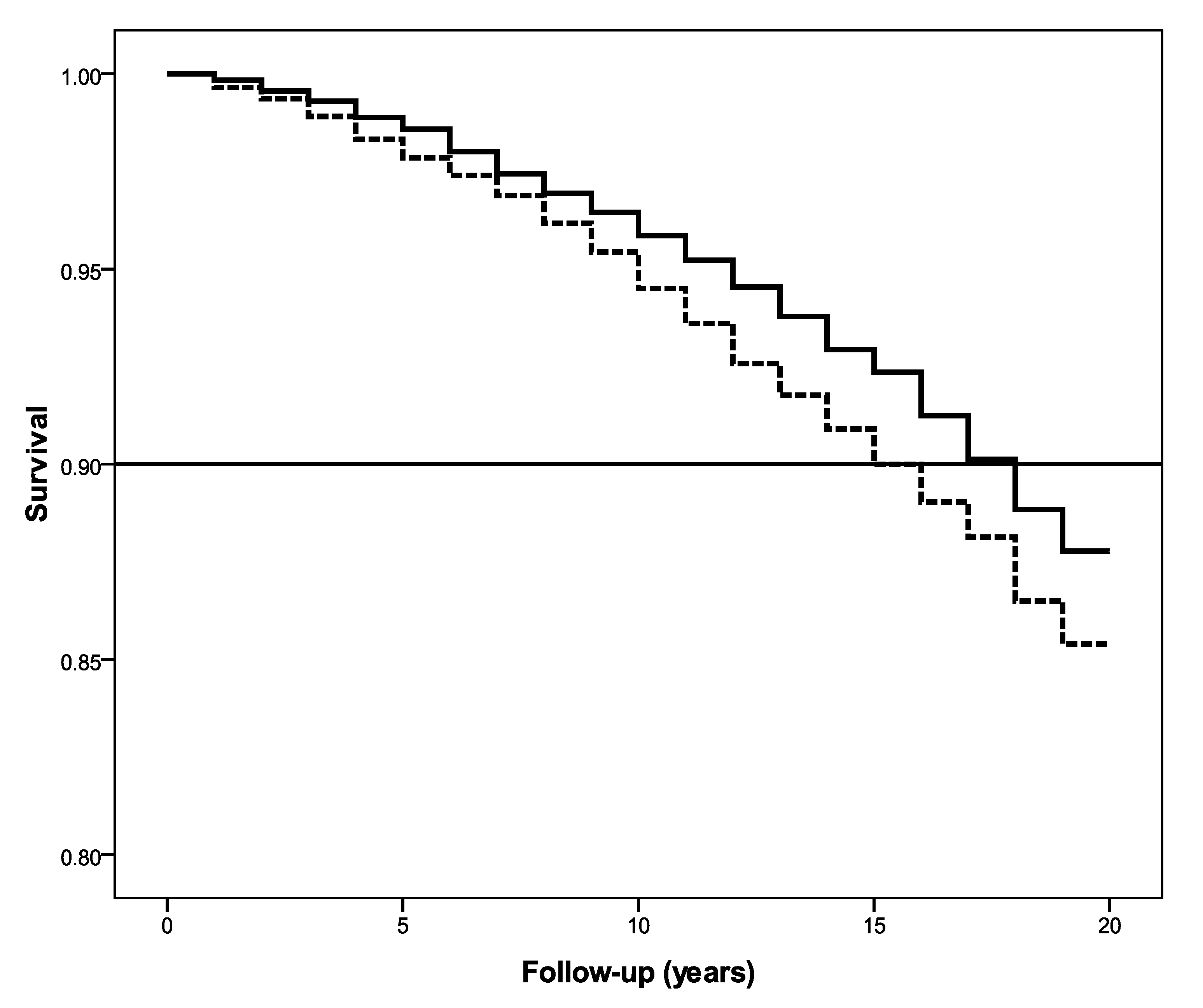
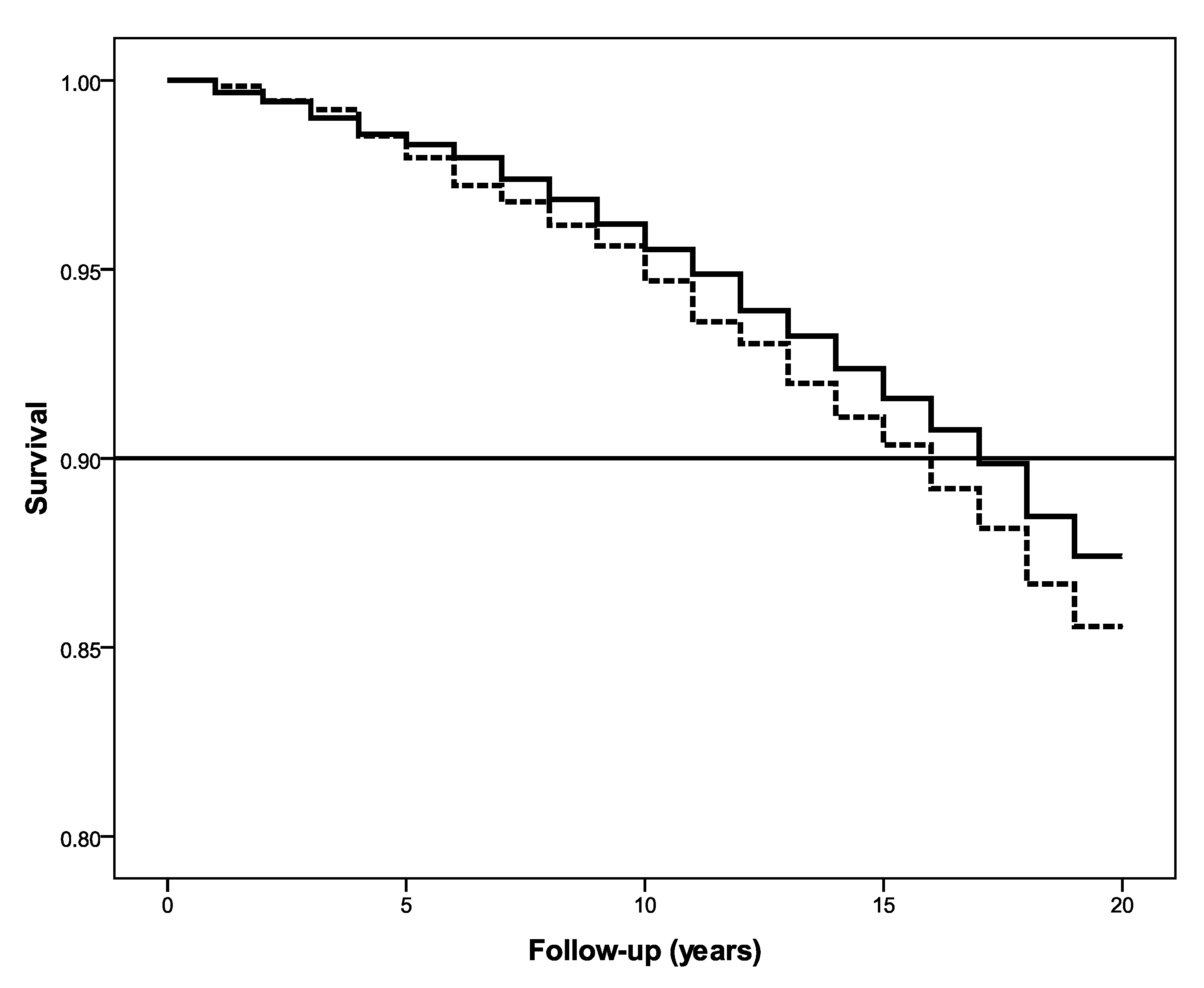
3.2. Kaplan–Meier Analysis
3.3. Cox Regression with Time-Varying Covariates
3.4. Mediational Analysis: Acceptance–Longevity Expectation–Mortality
3.5. Mediational Analysis: Interdependence–Serenity–Mortality
4. Discussion
4.1. Theoretical Implications
4.2. Practical Implications
4.3. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Roy, B.; Riley, C.; Sears, L.; Rula, E.Y. Collective Well-Being to Improve Population Health Outcomes: An Actionable Conceptual Model and Review of the Literature. Am. J. Health Promot. 2018, 32, 1800–1813. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.D. Pathways Linking Positive Emotion and Health in Later Life. Curr. Dir. Psychol. Sci. 2010, 19, 358–362. [Google Scholar] [CrossRef]
- Wisconsin Longitudinal Study-Data Documentation. Available online: https://www.ssc.wisc.edu/wlsresearch/documentation/ (accessed on 1 August 2020).
- Ryff, C.D. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Burns, R.A.; Machin, M.A. Investigating the Structural Validity of Ryff’s Psychological Well-Being Scales across Two Samples. Soc. Indic. Res. 2009, 93, 359–375. [Google Scholar] [CrossRef]
- Martín-María, N.; Lara, E.; Cresswell-Smith, J.; Forsman, A.K.; Kalseth, J.; Donisi, V.; Amaddeo, F.; Wahlbeck, K.; Miret, M. Instruments to Evaluate Mental Well-Being in Old Age: A Systematic Review. Aging Ment. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Barker, V.E.; Abrams, J.R.; Tiyaamornwong, V.; Seibold, D.R.; Duggan, A.; Park, H.S.; Sebastian, M. New Contexts for Relational Communication in Groups. Small Group Res. 2000, 31, 470–503. [Google Scholar] [CrossRef]
- Roth, A.E.; Willis, S.L.; Schaie, K.W. Consistency in Congruence Types over a Fourteen-Year Period: Relationship with Cognitive Performance and Rigidity/Flexibility. Gerontologist 2001, 41, 221–226. [Google Scholar]
- Buhler, C.; Massarik, F. The Course of Human Life: A Study of Goals in the Humanistic Perspective; Springer: New York, NY, USA, 1968; p. 422. [Google Scholar]
- Archibald, M.; Lawless, M.; Ambagtsheer, R.C.; Kitson, A. Older Adults’ Understandings and Perspectives on Frailty in Community and Residential Aged Care: An Interpretive Description. BMJ Open 2020, 10, e035339. [Google Scholar] [CrossRef]
- Tibubos, A.N.; Köber, C.; Habermas, T.; Rohrmann, S. Does Self-Acceptance Captured by Life Narratives and Self-Report Predict Mental Health? a Longitudinal Multi-Method Approach. J. Res. Personal. 2019, 79, 13–23. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B. The Contours of Positive Human Health. Psychol. Inq. 1998, 9, 1–28. [Google Scholar] [CrossRef]
- Levy, B.R.; Slade, M.D.; Kunkel, S.R.; Kasl, S.V. Longevity Increased by Positive Self-Perceptions of Aging. J. Personal. Soc. Psychol. 2002, 83, 261–270. [Google Scholar] [CrossRef]
- Phillips, D.; Smith, D. Postponement of Death until Symbolically Meaningful Occasions. JAMA 1990, 263, 1947–1951. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.; Bradley, E.H.; Kasl, S.V. Self-Rated Life Expectancy as a Predictor of Mortality: Evidence from the HRS and AHEAD Surveys. Gerontology 2003, 49, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Philipov, D.; Scherbov, S. Subjective Length of Life of European Individuals at Older Ages: Temporal and Gender Distinctions. PLoS ONE 2020, 15, e0229975. [Google Scholar] [CrossRef]
- Post, T.; Hanewald, K. Longevity Risk, Subjective Survival Expectations, and Individual Saving Behavior. J. Econ. Behav. Organ. 2013, 86, 200–220. [Google Scholar] [CrossRef]
- Custers, A.F.J.; Westerhof, G.J.; Kuin, Y.; Gerritsen, D.L.; Riksen-Walraven, J.M. Relatedness, Autonomy, and Competence in the Caring Relationship: The Perspective of Nursing Home Residents. J. Aging Stud. 2012, 26, 319–326. [Google Scholar] [CrossRef]
- Clarke, P.J.; Marshall, V.W.; Ryff, C.D.; Wheaton, B. Measuring Psychological Well-Being in the Canadian Study of Health and Aging. Int. Psychogeriatr. 2001, 13, 79–90. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Niemiec, C.P. It’s Not Just the Amount That Counts: Balanced Need Satisfaction Also Affects Well-Being. J. Personal. Soc. Psychol. 2006, 91, 331–341. [Google Scholar] [CrossRef]
- Levy, B.R.; Zonderman, A.B.; Slade, M.D.; Ferrucci, L. Age Stereotypes Held Earlier in Life Predict Cardiovascular Events in Later Life. Psychol. Sci. 2009, 20, 296–298. [Google Scholar] [CrossRef]
- Mok, E.; Wong, F.; Wong, D. The Meaning of Spirituality and Spiritual Care among the Hong Kong Chinese Terminally Ill. J. Adv. Nurs. 2010, 66, 360–370. [Google Scholar] [CrossRef]
- Elias, A.C.A.; Giglio, J.S.; Pimenta, C.A.d.M. Analysis of the Nature of Spiritual Pain in Terminal Patients and the Resignification Process through the Relaxation, Mental Images and Spirituality (RIME) Intervention. Rev. Lat. Am. de Enferm. 2008, 16, 959–965. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kruse, B.G. The Lived Experience of Serenity: Using Parse’s Research Method. Nurs. Sci. Q. 1999, 12, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Barham, D. The Last 48 Hours of Life: A Case Study of Symptom Control for a Patient Taking a Buddhist Approach to Dying. Int. J. Palliat. Nurs. 2003, 9, 245–251. [Google Scholar] [CrossRef]
- Kocher, B. Approaching Death with Serenity. Krankenpfl. Soins Infirm. 1994, 87, 62–64. [Google Scholar] [PubMed]
- Friedman, H.S.; Kern, M.L.; Reynolds, C.A. Personality and Health, Subjective Well-Being, and Longevity. J. Personal. 2010, 78, 179–216. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Costa, P. Domain and Facet Personality Predictors of All-Cause Mortality Among Medicare Patients Aged 65 to 100. Psychosom. Med. 2005, 67, 724–733. [Google Scholar] [CrossRef]
- Wilson, R.S.; de Leon, C.F.M.; Bienias, J.L.; Evans, D.A.; Bennett, D.A. Personality and Mortality in Old Age. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2004, 59, P110–P116. [Google Scholar] [CrossRef]
- Surtees, P.G.; Wainwright, N.W.J.; Luben, R.; Khaw, K.-T.; Day, N.E. Mastery, Sense of Coherence, and Mortality: Evidence of Independent Associations from the EPIC-Norfolk Prospective Cohort Study. Health Psychol. 2006, 25, 102–110. [Google Scholar] [CrossRef]
- Gadalla, T.M. Sense of Mastery, Social Support, and Health in Elderly Canadians. J. Aging Health 2009, 21, 581–595. [Google Scholar] [CrossRef]
- Boyle, P.A.; Barnes, L.L.; Buchman, A.S.; Bennett, D.A. Purpose in Life Is Associated with Mortality among Community-Dwelling Older Persons. Psychosom. Med. 2009, 71, 574–579. [Google Scholar] [CrossRef]
- Sirri, L.; Potena, L.; Masetti, M.; Tossani, E.; Magelli, C.; Grandi, S. Psychological Predictors of Mortality in Heart Transplanted Patients: A Prospective, 6-Year Follow-up Study. Transplantation 2010, 89, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Nishi, A.; Kondo, K.; Hirai, H.; Kawachi, I. Cohort Profile: The AGES 2003 Cohort Study in Aichi, Japan. J. Epidemiol. 2011, 21, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Taubman-Ben-Ari, O.; Eherenfreund-Hager, A.; Findler, L. Mortality Salience and Positive Affect Influence Adolescents’ Attitudes toward Peers with Physical Disabilities: Terror Management and Broaden and Build Theories. Death Stud. 2011, 35, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Sewell, W.H.; Hauser, R.M.; Springer, K.W.; Hauser, T.S. As We Age: A Review of the Wisconsin Longitudinal Study, 1957–2001. Res. Soc. Stratif. Mobil. 2003, 20, 3–111. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L.M. The Structure of Psychological Well-Being Revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B.H. Best News yet on the Six-Factor Model of Well-Being. Soc. Sci. Res. 2006, 35, 1103–1119. [Google Scholar] [CrossRef]
- John, O.P. The “Big Five” Factor Taxonomy: Dimensions of Personality in the Natural Language and in Questionnaires. In Handbook of Personality: Theory and Research; The Guilford Press: New York, NY, USA, 1990; pp. 66–100. [Google Scholar]
- Arbuckle, J.L. AMOS: A Structural Equation Modeling Software; SmallWaters Corporation: Chicago, IL, USA, 2007. [Google Scholar]
- Springer, K.W.; Hauser, R.M. An Assessment of the Construct Validity of Ryff’s Scales of Psychological Well-Being: Method, Mode, and Measurement Effects. Soc. Sci. Res. 2006, 35, 1080–1102. [Google Scholar] [CrossRef]
- Hu, L.-T.; Bentler, P.M. Evaluating Model Fit. In Structural Equation Modeling: Concepts, Issues, and Applications; Sage: Thousand Oaks, CA, USA, 1995; pp. 76–99. [Google Scholar]
- Steiger, J.H. Statistically Based Tests for the Number of Common Factors. In Proceedings of the Annual Meeting of the Psychometric Society, Iowa City, IA, USA, 28 May 1980. [Google Scholar]
- Browne, M.W.; Cudeck, R. Single Sample Cross-Validation Indices for Covariance Structures. Multivar. Behav. Res. 1989, 24, 445–455. [Google Scholar] [CrossRef]
- Allison, P.D. Survival Analysis Using SAS: A Practical Guide; SAS Institute: Cary, NC, USA, 1995. [Google Scholar]
- MacKinnon, D.P.; Fritz, M.S.; Williams, J.; Lockwood, C.M. Distribution of the Product Confidence Limits for the Indirect Effect: Program PRODCLIN. Behav. Res. Methods 2007, 39, 384–389. [Google Scholar] [CrossRef]
- Wegener, D.T.; Fabrigar, L.R. Analysis and Desgin for Nonexperimental Data: Addressing Causal and Noncausal Hypothesis. In Handbook of Research Methods in Social and Personality Psychology; Cambridge University Press: New York, NY, USA, 2000; pp. 412–450. [Google Scholar]
- Shrout, P.E.; Bolger, N. Mediation in Experimental and Nonexperimental Studies: New Procedures and Recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef]
- Morera, O.F.; Castro, F.G. Important Considerations in Conducting Statistical Mediation Analyses. Am. J. Public Health 2013, 103, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Ng, R.; Ong, E.L.; Lin, P.K.F. Different Mediators for the Age, Sex, and Attitude Similarity Effects in Interpersonal Attraction. Basic Appl. Soc. Psychol. 2008, 30, 1–17. [Google Scholar] [CrossRef]
- Levy, B.R.; Leifheit-Limson, E. The Stereotype-Matching Effect: Greater Influence on Functioning When Age Stereotypes Correspond to Outcomes. Psychol. Aging 2009, 24, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.R.; Hausdorff, J.M.; Hencke, R.; Wei, J.Y. Reducing Cardiovascular Stress with Positive Self-Stereotypes of Aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 2000, 55, P205–P213. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D. Psychological Well-Being in Adult Life. Curr. Dir. Psychol. Sci. 1995, 4, 99–104. [Google Scholar] [CrossRef]
- van Dierendonck, D. The Construct Validity of Ryff’s Scales of Psychological Well-Being and Its Extension with Spiritual Well-Being. Personal. Individ. Differ. 2004, 36, 629–643. [Google Scholar] [CrossRef]
- Cloninger, C.R. The Science of Well-Being: An Integrated Approach to Mental Health and Its Disorders. World Psychiatry 2006, 5, 71–76. [Google Scholar]
- Heidekrueger, P.I.; Szpalski, C.; Weichman, K.; Juran, S.; Ng, R.; Claussen, C.; Ninkovic, M.; Broer, P.N. Lip Attractiveness: A Cross-Cultural Analysis. Aesthet. Surg. J. 2017, 37, 828–836. [Google Scholar] [CrossRef]
- Broer, P.N.; Juran, S.; Walker, M.E.; Ng, R.; Weichman, K.; Tanna, N.; Liu, Y.-J.; Shah, A.; Patel, A.; Persing, J.A.; et al. Aesthetic Breast Shape Preferences Among Plastic Surgeons. Ann. Plast. Surg. 2015, 74, 639–644. [Google Scholar] [CrossRef]
- Heidekrueger, P.I.; Sinno, S.; Tanna, N.; Szpalski, C.; Juran, S.; Schmauss, D.; Ehrl, D.; Ng, R.; Ninkovic, M.; Broer, P.N. The Ideal Buttock Size: A Sociodemographic Morphometric Evaluation. Plast. Reconstr. Surg. 2017, 140, 20e–32e. [Google Scholar] [CrossRef]
- Ng, R.; Levy, B. Pettiness: Conceptualization, measurement and cross-cultural differences. PLOS ONE 2018, 13, e0191252. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Allore, H.G.; Monin, J.K.; Levy, B.R. Retirement as Meaningful: Positive Retirement Stereotypes Associated with Longevity. J. Soc. Issues 2016, 72, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Allore, H.G.; Trentalange, M.; Monin, J.K.; Levy, B.R. Increasing Negativity of Age Stereotypes across 200 Years: Evidence from a Database of 400 Million Words. PLoS ONE 2015, 10, e0117086. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Lim, S.Q.; Saw, S.Y.; Tan, K.B. 40-Year Projections of Disability and Social Isolation of Older Adults for Long-Range Policy Planning in Singapore. Int. J. Environ. Res. Public Health 2020, 17, 4950. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Psychological Well-Being | Model 4 | Model 3 | Model 2 | Model 1 | ||||
|---|---|---|---|---|---|---|---|---|
| HR 1 (95% CI 2) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Self-acceptance | 0.81 (0.69, 0.96) | 0.015 | 0.83 (0.71, 0.98) | 0.024 | 0.87 (0.77, 0.99) | 0.036 | 0.88 (0.78, 0.99) | 0.039 |
| Sense of purpose | 0.89 (0.75, 1.06) | 0.19 | 0.90 (0.78, 1.06) | 0.22 | 0.93 (0.82, 1.06) | 0.27 | 0.90 (0.80, 1.01) | 0.081 |
| Positive relations | 1.05 (0.91, 1.20) | 0.51 | 1.05 (0.92, 1.19) | 0.49 | 0.98 (0.89, 1.08) | 0.70 | 0.99 (0.91, 1.08) | 0.84 |
| Personal growth | 1.10 (0.93, 1.30) | 0.27 | 1.09 (0.93, 1.29) | 0.28 | 1.09 (0.96, 1.23) | 0.20 | 1.04 (0.92, 1.17) | 0.51 |
| Environmental mastery | 1.06 (0.88, 1.28) | 0.51 | 1.07 (0.89, 1.28) | 0.47 | 1.04 (0.90, 1.19) | 0.63 | 1.04 (0.91, 1.18) | 0.60 |
| Interdependence | 0.83 (0.66, 0.99) | 0.029 | 0.83 (0.66, 0.98) | 0.019 | 0.87 (0.75, 0.98) | 0.022 | 0.86 (0.74, 0.96) | 0.008 |
| Demographics | ||||||||
| Age | 1.20 (1.02, 1.42) | 0.028 | 1.19 (1.01, 1.39) | 0.034 | 1.17 (1.02, 1.33) | 0.020 | ||
| Gender | ||||||||
| Male | Reference | |||||||
| Female | 0.80 (0.67, 0.96) | 0.018 | 0.76 (0.64, 0.91) | 0.0023 | 0.73 (0.63, 0.83) | <0.001 | ||
| Education | ||||||||
| No college | Reference | |||||||
| Attended college | 0.73 (0.60, 0.87) | <0.001 | 0.74 (0.62, 0.88) | <0.001 | 0.74 (0.64, 0.85) | <0.001 | ||
| Race | ||||||||
| Whites | Reference | |||||||
| Blacks | 3.72 (1.38, 10.01) | 0.0093 | 3.53 (1.31, 9.47) | 0.013 | 2.62 (1.08, 6.31) | 0.032 | ||
| Marriage | ||||||||
| Married | Reference | |||||||
| Single | 1.81 (1.27, 2.60) | 0.0011 | 1.69 (1.19, 2.40) | 0.0036 | 1.66 (1.24, 2.22) | <0.001 | ||
| Divorced/separated | 1.85 (1.48, 2.31) | <0.001 | 1.74 (1.41, 2.16) | <0.001 | 1.68 (1.41, 2.01) | <0.001 | ||
| Psychological Covariates | ||||||||
| Openness | 0.91 (0.80, 1.04) | 0.16 | 0.94 (0.83, 1.06) | 0.30 | ||||
| Neuroticism | 0.97 (0.87, 1.08) | 0.54 | 0.95 (0.86, 1.06) | 0.36 | ||||
| Conscientiousness | 0.90 (0.78, 1.04) | 0.17 | 0.88 (0.77, 1.01) | 0.07 | ||||
| Agreeableness | 1.02 (0.89, 1.16) | 0.80 | 1.01 (0.89, 1.15) | 0.83 | ||||
| Extroversion | 0.98 (0.87, 1.09) | 0.68 | 0.96 (0.86, 1.06) | 0.39 | ||||
| Depression | 0.99 (0.94, 1.04) | 0.64 | 0.99 (0.94, 1.04) | 0.63 | ||||
| Self-rated health | 0.99 (0.86, 1.14) | 0.89 | 1.01 (0.89, 1.15) | 0.89 | ||||
| Physical Covariates | ||||||||
| Smoking | ||||||||
| No | Reference | |||||||
| Yes | 1.00 (0.77, 1.28) | 0.99 | ||||||
| Illness count 3 | 1.01 (0.96, 1.08) | 0.62 | ||||||
| Body mass index 4 | 0.99 (0.97, 1.01) | 0.27 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, R.; Allore, H.G.; Levy, B.R. Self-Acceptance and Interdependence Promote Longevity: Evidence From a 20-year Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 5980. https://doi.org/10.3390/ijerph17165980
Ng R, Allore HG, Levy BR. Self-Acceptance and Interdependence Promote Longevity: Evidence From a 20-year Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5980. https://doi.org/10.3390/ijerph17165980
Chicago/Turabian StyleNg, Reuben, Heather G. Allore, and Becca R. Levy. 2020. "Self-Acceptance and Interdependence Promote Longevity: Evidence From a 20-year Prospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 16: 5980. https://doi.org/10.3390/ijerph17165980
APA StyleNg, R., Allore, H. G., & Levy, B. R. (2020). Self-Acceptance and Interdependence Promote Longevity: Evidence From a 20-year Prospective Cohort Study. International Journal of Environmental Research and Public Health, 17(16), 5980. https://doi.org/10.3390/ijerph17165980