Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population


 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
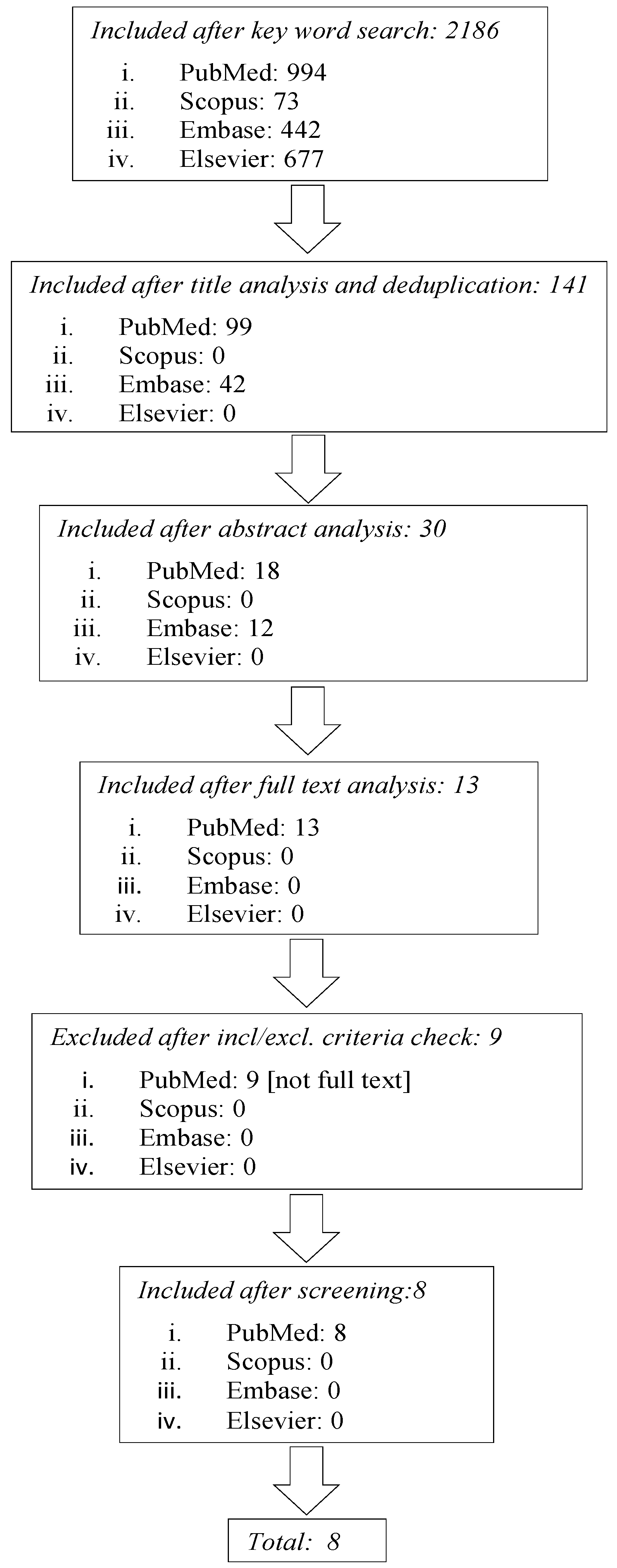
2.1. Literature Search and Study Selection
2.2. Selection Strategy
- Studies conducted on adult aged ≥65 years.
- Studies devoted to use technological systems for health coaching, in multiple or sole interventions, without any restriction in terms of technological applications.
- Randomized controlled trials, with control group which received usual care or different intervention.
- Before-after comparison of a single group.
- Conference proceedings.
- Studies for which the full text was not found.
- Studies written in languages other than English.
- Technical papers.
- Qualitative studies.
- Review articles.
2.3. Data Collection
3. Results
3.1. Study Quality Evaluation
3.2. General Characteristics of the Study Population
3.3. Descriptive Analysis and Outcome Measures
3.4. Intervention Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Palmer, K.; Marengoni, A.; Forjaz, M.J.; Jureviciene, E.; Laatikainen, T.; Mammarella, F.; Muth, C.; Navickas, R.; Prados-Torres, A.; Rijken, M.; et al. Joint Action on Chronic Diseases and Promoting Healthy Ageing Across the Life Cycle (JA-CHRODIS). Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy 2018, 122, 4–11. [Google Scholar] [PubMed]
- Farmer, C.; Fenu, E.; O’Flynn, N.; Guthrie, B. Clinical assessment and management of multimorbidity: summary of NICE guidance. BMJ 2016, 354, i4843. [Google Scholar] [CrossRef] [PubMed]
- Lattanzio, F.; Abbatecola, A.M.; Bevilacqua, R.; Chiatti, C.; Corsonello, A.; Rossi, L.; Bustacchini, S.; Bernabei, R. Advanced technology care innovation for older people in Italy: Necessity and opportunity to promote health and wellbeing. JAMDA 2014, 15, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://abcproject.eu/img/ABC%20Final.pdf (accessed on 1 July 2020).
- Mitzner, T.L.; McBride, S.E.; Barg-Warlow, L.; Rogers, W.A. Self-management of wellness and illness in an aging popoulation. Hum. Factor Ergon. Man 2013, 3, 277–333. [Google Scholar] [CrossRef]
- Costa, E.; Giardini, A.; Savin, M.; Menditto, E.; Lehane, E.; Laosa, O.; Pecorelli, S.; Monaco, A.; Marengoni, A. Interventional tools to improve medication adherence: Review of literature. Patient Prefer. Adher. 2015, 9, 1303–1314. [Google Scholar] [CrossRef]
- MacLeod, S.; Musich, S.; Hawkins, K.; Alsgaard, K.; Wicker, E.R. The impact of resilience among older adults. Geriatr. Nurs. 2016, 37, 266–272. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Kulzer, B.; Hermanns, N.; Gorges, D.; Schwarz, P.; Haak, T. Prevention of Diabetes Self-Management Program (PREDIAS): Effects on Weight, Metabolic Risk Factors, and Behavioral Outcomes. Diabetes Care 2009, 32, 1143–1146. [Google Scholar] [CrossRef][Green Version]
- Portz, J.D. A review of web-based chronic disease self-management for older adults. Gerontechnology 2017, 16, 12–20. [Google Scholar] [CrossRef]
- Cesari, M.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Cooper, C.; Martin, F.C.; Reginster, J.Y.; Vellas, B.; Beard, J.R. Evidence for the Domains Supporting the Construct of IC. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1653–1660. [Google Scholar] [CrossRef]
- Marengoni, A.; Vetrano, D.L.; Onder, G. Target Population for Clinical Trials on Multimorbidity: Is DiseaseCount Enough? JAMDA 2019, 20, 113–114. [Google Scholar] [CrossRef]
- Smith, D.C.; Lanesskog, D.; Cleeland, L.; Motl, R.; Weikert, M.; Dlugonski, D. Motivational Interviewing May Improve Exercise Experience for People with Multiple Sclerosis: A Small Randomized Trial. Health Soc. Work 2012, 37, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Droppa, M.; Lee, H. Motivational interviewing: a journey to improve health. Nursing 2014, 44, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Maissi, E.; Ridge, K.; Treasure, J.; Chalder, T.; Roche, S.; Barlett, J.; Schmidt, U.; Thomas, S.; Ismail, K. Nurse-led psychological interventions to improve diabetes control: assessing competencies. Patient Educ. Couns. 2011, 84, e37–e43. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.D.; Ivezaj, V. A systematic review of motivational interviewing for weight loss among adults in primary care. Obes. Rev. 2015, 16, 304–318. [Google Scholar] [CrossRef]
- Rehman, H.; Karpman, C.; Vickers Douglas, K.; Benzo, R.P. Effect of a Motivational Interviewing-Based Health Coaching on Quality of Life in Subjects with COPD. Respir. Care 2017, 62, 1043–1048. [Google Scholar] [CrossRef]
- Bombardier, C.H.; Cunniffe, M.; Wadhwani, R.; Gibbons, L.E.; Blake, K.D.; Kraft, G.H. The efficacy of telephone counseling for health promotion in people with multiple sclerosis: A randomized controlled trial. Arch. Phys. Med. Rehab. 2008, 89, 1849–1856. [Google Scholar] [CrossRef]
- Chen, S.M.; Creedy, D.; Lin, H.S.; Wollin, J. Effects of motivational interviewing intervention on self-management, psychological and glycemic outcomes in type 2 diabetes: A randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 637–644. [Google Scholar] [CrossRef]
- Shingleton, R.M.; Palfai, T.P. Technology-Delivered Adaptations of Motivational Interviewing for Health-Related Behaviors: A Systematic Review of the Current Research. Patient Educ. Couns. 2016, 99, 17–35. [Google Scholar] [CrossRef]
- Bickmore, T.W.; Silliman, R.A.; Nelson, K.; Cheng, D.M.; Winter, M.; Henault, L.; Paasche-Orlow, M.K. A randomized controlled trial of an automated exercise coach for older adults. J. Am. Geriatr. Soc. 2013, 61, 1676–1683. [Google Scholar] [CrossRef]
- McDonald, D.D.; Walsh, S.; Vergara, C.; Gifford, T.; Weiner, D.K. The effect of a Spanish virtual pain coach for older adults: A pilot study. Pain. Med. 2012, 13, 1397–1406. [Google Scholar] [CrossRef]
- Tabak, M.; Brusse-Keizer, M.; van der Valk, P.; Hermens, H.; Vollenbroek-Hutten, M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: A pilot randomized controlled trial. Int. J. Chron. Obstruct. Pulm. Dis. 2014, 9, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, C.S.; Houston, T.K.; Richman, J.S.; Sobko, H.J.; Berner, E.S.; Taylor, B.B.; Salanitro, A.H.; Locher, J.L. The E-Coach technology-assisted care transition system: a pragmatic randomized trial. Transl. Behav. Med. 2016, 6, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.D.; Anam, R.; Karanam, C.; Downey, P.; Ruiz, J.G. An overactive bladder online self-management program with embedded avatars: a randomized controlled trial of efficacy. Urology 2015, 85, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, E.; Garrett, J.; Jepsen, N.; Li Ogilvie, V.; Ahn, H.S.; Robinson, H.; Peri, K.; Kerse, N.; Rouse, P.; Pillai, A.; et al. Using Robots at Home to Support Patients With Chronic Obstructive Pulmonary Disease: Pilot Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e45. [Google Scholar] [CrossRef] [PubMed]
- Broekhuizen, K.; de Gelder, J.; Wijsman, C.A.; Wijsman, L.W.; Westendorp, R.G.; Verhagen, E.; Slagboom, P.E.; de Craen, A.J.; van Mechelen, W.; van Heemst, D.; et al. An Internet-Based Physical Activity Intervention to Improve Quality of Life of Inactive Older Adults: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e74. [Google Scholar] [CrossRef] [PubMed]
- Tabak, M.; Vollenbroek-Hutten, M.M.; van der Valk, P.D.; van der Palen, J.; Hermens, H.J. A telerehabilitation intervention for patients with Chronic Obstructive Pulmonary Disease: A randomized controlled pilot trial. Clin. Rehabil. 2014, 8, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Lukaschek, K.; Mergenthal, K.; Heider, D.; Hanke, A.; Munski, K.; Moschner, A.; Emig, M.; van den Akker, M.; Zapf, A.; Wegscheider, K.; et al. eHealth-supported case management for patients with panic disorder or depression in primary care: Study protocol for a cRCT (PREMA). Trials 2019, 20, 662. [Google Scholar] [CrossRef]
- Kwan, B.; Frankish, J.; Rootman, I. The Development and Validation of Measures of “Health Literacy” in Different Populations; University of British Columbia Institute of Health Promotion Research & University of Victoria Centre for Community Health Promotion Research: Vancouver, BC, Canada, 2006. [Google Scholar]
- Bickmore, T.W.; Pfeifer, L.M.; Byron, D.; Forsythe, S.; Henault, L.E.; Jack, B.W.; Silliman, R.; Paasche-Orlow, M.K. Usability of conversational agents by patients with inadequate health literacy: Evidence from two clinical trials. J. Health Commun. 2010, 15 (Suppl. 2), 197–210. [Google Scholar] [CrossRef]
- El Kamali, M.; Angelini, L.; Caon, M.; Carrino, F.; Röcke, C.; Guye, S.; Rizzo, G.; Mastropirtro, A.; Sykora, M.; Kniestedt, I. Virtual Coaches for Older Adults’ Wellbeing: A Systematic Review. IEEE Access 2020, 8, 101884–101902. [Google Scholar] [CrossRef]
- Bickmore, T.; Cassell, J. Relational Agents: A Model and Implementation of Building User Trust. In Proceedings of the ACM CHI 2001 Conference Proceedings, Seattle, DC, USA, 31 March–5 April 2001; pp. 369–403. [Google Scholar]
- Gaudiello, I.; Zibetti, E.; Lefort, S.; Chetouani, M.; Ivaldi, S. Trust as Indicator of Robot Functional and Social Acceptance. An Experimental Study on User Conformation to Icub Answers. Comput. Human Behav. 2016, 61, 633–655. [Google Scholar] [CrossRef]
- Barrett, D.H.; Haruna, A. Artificial intelligence and machine learning for targeted energy storage solutions. Curr. Opin. Electrochem. 2020, 21, 160–166. [Google Scholar] [CrossRef]
- Dankwa-Mullan, I.; Rivo, M.; Sepulveda, M.; Park, Y.; Snowdon, J.; Rhee, K. Transforming Diabetes Care Through Artificial Intelligence: The Future Is Here. Popul. Health Manag. 2019, 22, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, R.; Felici, E.; Marcellini, F.; Glende, S.; Klemcke, S.; Conrad, I.; Esposito, R.; Cavallo, F.; Dario, P. Robot-Era project: Preliminary results on the system usability. Part of the Lecture Notes in Computer Science book series (LNCS, Volume 9188). In Proceedings of the International Conference of Design, User Experience, and Usability (DUXU), Los Angeles, CA, USA, 2–7 August 2015; pp. 553–561. [Google Scholar]
- Cavallo, F.; Esposito, R.; Limosani, R.; Manzi, A.; Bevilacqua, R.; Felici, E.; Di Nuovo, A.; Cangelosi, A.; Lattanzio, F.; Dario, P.M. Robotic Services Acceptance in Smart Environments with Older Adults: User Satisfaction and Acceptability Study. J. Med. Internet Res. 2018, 20, e264. [Google Scholar] [CrossRef] [PubMed]
- Casaccia, S.; Bevilacqua, R.; Scalise, L.; Revel, G.M.; Astell, A.J.; Spinsante, S.; Rossi, L. Assistive sensor-based technology driven self-management for building resilience among people with early stage cognitive impairment. In Proceedings of the 2019 IEEE International Symposium on Measurements & Networking (M&N), Catania, Italy, 8–10 July 2019; pp. 1–5. [Google Scholar]
- Arnesano, M.; Casaccia, S.; di Perna, C.; Passerini, G.; Principi, P.; Revel, G.M.; Ulpiani, G. Citizen-Oriented Technologies in the Cities of Tomorrow. In The First Outstanding 50 Years of “Università Politecnica delle Marche”; Springer: Cham, Switzerland, 2019; pp. 143–160. [Google Scholar]
- Fiorini, L.; Esposito, R.; Bonaccorsi, M.; Petrazzuolo, C.; Saponara, F.; Giannantonio, R.; De Petris, G.; Dario, P.; Cavallo, F. Enabling personalised medical support for chronic disease management through a hybrid robot-cloud approach. Auton. Robots 2017, 41, 1263–1276. [Google Scholar] [CrossRef]
- Casaccia, S.; Revel, G.M.; Scalise, L.; Bevilacqua, R.; Rossi, L.; Paauwe, R.A.; Karkowsky, I.; Ercoli, I.; Artur Serrano, J.; Suijkerbuijk, S.; et al. Social Robot and Sensor Network in Support of Activity of Daily Living for People with Dementia. In Dementia Lab 2019. Making Design Work: Engaging with Dementia in Context; Springer: Cham, Switzerland, 2019. [Google Scholar]


{kind=link}
| PEDro | Bickmore et al., 2013 [21] | Mc Donald et al., 2012 [22] | Tabak et al., 2014 [23] | Ritchie et al., 2012 [24] | Andrade et al., 2014 [25] | Broadbent et al., 2018 [26] | Broekhuizen et al., 2016 [27] | Tabak et al., 2013 [28] |
|---|---|---|---|---|---|---|---|---|
| Eligibility | Y | Y | Y | Y | Y | Y | Y | Y |
| Randomized Allocation | Y | Y | Y | Y | Y | Y | Y | Y |
| Concealed Allocation | Y | N | Y | Y | Y | Y | Y | Y |
| Baseline Comparability | Y | N | N | N | N | N | N | N |
| Blinded Subject | N | N | N | N | N | N | N | N |
| Blinded Therapists | N | N | N | N | N | N | N | N |
| Blinded Raters | Y | N | N | N | Y | N | N | N |
| Key Outcomes | Y | Y | Y | Y | Y | Y | Y | Y |
| Intention to Treat | N | N | N | N | N | N | N | N |
| Comparison between Groups | Y | Y | Y | Y | Y | Y | Y | Y |
| Precision and Variability | Y | Y | Y | Y | Y | Y | Y | Y |
| 7/11 | 5/11 | 6/11 | 6/11 | 7/11 | 6/11 | 6/11 | 6/11 |
| Population | Intervention | Outcomes and Measurements | Results | |
|---|---|---|---|---|
| Bickmore et al., 2013 [21] | EG = 132 cases (age 71.7 ± 5.6 years) CG = 131 controls (age 70.8 ± 5.2 years) | EG was provided with touch screens tablet to use for 2 months connected with pedometers, that communicate through an animated virtual coach to discuss walking and setting goals. | Primary outcome: Average daily steps for 30 days before the 12-month interview Secondary outcome: Average daily steps for 30 days before the 2-month interview Outcomes were stratified according to health literacy level. | Primary outcome: p = 0.09 p = 0.02 (with adequate health literacy) Secondary outcome: p = 0.01 p = 0.03 (with adequate health literacy) |
| Mc Donald et al., 2012 [22] | EG = 8 cases with osteoarthritis pain (age 69.9 ± 7.4 years) CG = 10 controls with osteoarthritis pain (age 66.7 ± 4.3) | All participants viewed the pain communication videotape. EG practiced talking about osteoarthritis pain with the virtual pain coach | Primary outcomes: Pain intensity Pain interference with activities Depressive symptoms At baseline and 1 month later, between and within groups | Primary outcomes: p = 0.72 (between groups) p = 0.017 (within EG in depressive symptoms) |
| Tabak et al., 2014 [23] | EG = 12 cases with COPD (age 64.1 ± 9.0 years) CG = 12 controls with COPD (age 62.8 ± 7.4 years) | 4 modules: 1. Activity coach for ambulant activity monitoring and real-time coaching of daily activity behavior; 2. Web-based exercise program for home exercising; 3. Self-management of COPD exacerbations; 4. Teleconsultation. | Primary outcomes: Client Satisfaction Questionnaire 8 | Primary outcomes: Satisfaction with received care was 26.4 for the telehealth group and 30.4 (1.5) for the usual-care group after 1 month. After 3 months, this was 26.3 for the telehealth group and 29.9 for the usual-care group. |
| Ritchie et al., 2012 [24] | EG = 233 cases with CHF/COPD (age 63.0 ± 12.1 years) CG = 245 controls with CHF/COPD (age 63.8 ± 12.8 years) | E-Coach: intervention with condition-specific customization and in-hospital and post-discharge support by a CTN, interactive voice response post-discharge calls, and CTN follow-up versus usual post-discharge care. | Primary outcome: 30-days rehospitalization Secondary outcomes: Rehospitalization/death Community tenure | Primary outcome HR (95%CI): CHF: 1.14 (0.67 1.96) COPD: 0.56 (0.23 1.38) Secondary outcome: Rehospitalization/death: HR (95%CI) CHF: 1.03 (0.6 −1.8) COPD: 0.44 (0.2 −1.2) Community tenure: Beta(95%CI) CHF: −0.11 (−1.0 −0.9) COPD: 1.12 (1.11 −2.12) |
| Andrade et al., 2014 [25] | EG = 22 cases with OAB (age 62.41 ± 7.25 years) CG = 19 controls with OAB (age 60.68 ± 5.30 years) | EG: self-management program with a generic avatar coach with a self-avatar peer mentor. CG: identical online program with voice only. | Primary outcome: Quality of life (HRQoL) Secondary outcomes: Perception of bladder condition (PPBC) OAB symptoms Self-efficacy | Primary outcome: HRQoL p = 0.02 Secondary outcomes: PPBC p = 0.63 OAB symptoms p = 0.75 Self-efficacy p = 0.99 |
| Broadbent et al., 2018 [26] | EG = 30 cases with COPD (age 69.10 ± 9.85) CG = 30 controls with COPD (age 70.57 ± 10.34) | EG received a robot at home for 4 months in addition to usual care. CG received standard care alone. | Primary outcome: Number of days of hospitalization. Secondary outcome: Medication adherence Frequency of rehabilitation exercise Quality of life using CCQ | Primary outcome: p = 0.9 Secondary outcomes: Medication adherence: p = 0.04 Frequency of rehabilitation exercise: p = 0.001 CCQ: p = 0.35 |
| Broekhuizen et al., 2016 [27] | EG = 119 cases (age 64.7 ± 3.0) CG = 116 controls (age 64.9 ± 2.8) | EG used internet program with monitoring and feedback by accelerometry and feedback by digital coaching (messages, e-mail). CG received no intervention. | Primary outcomes: Quality of life (RAND-36) Physical activity between and within groups | Primary outcomes: Between groups RAND-36: p = 0.03 Physical activity: p = 0.01 Primary outcomes: Within EG RAND-36: p = 0.009 Physical activity: p = 0.004 |
| Tabak et al., 2013 [28] | EG = 14 cases (age 65.2 ± 9.0) CG = 11 controls (age 67.9 ± 5.7) | EG: activity coach for ambulant activity registration and real-time feedback for 4 weeks. CG: usual care | Primary outcomes: Activity level (step/day) Health status (CCQ) between and within groups | Primary outcomes: Between groups Activity level: p = 0.48 CCQ: p = 0.1 Primary outcomes: Within EG Activity level: p = 0.38 CCQ: p = 0.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bevilacqua, R.; Casaccia, S.; Cortellessa, G.; Astell, A.; Lattanzio, F.; Corsonello, A.; D’Ascoli, P.; Paolini, S.; Di Rosa, M.; Rossi, L.; et al. Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population. Int. J. Environ. Res. Public Health 2020, 17, 5930. https://doi.org/10.3390/ijerph17165930
Bevilacqua R, Casaccia S, Cortellessa G, Astell A, Lattanzio F, Corsonello A, D’Ascoli P, Paolini S, Di Rosa M, Rossi L, et al. Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population. International Journal of Environmental Research and Public Health. 2020; 17(16):5930. https://doi.org/10.3390/ijerph17165930
Chicago/Turabian StyleBevilacqua, Roberta, Sara Casaccia, Gabriella Cortellessa, Arlene Astell, Fabrizia Lattanzio, Andrea Corsonello, Paola D’Ascoli, Susy Paolini, Mirko Di Rosa, Lorena Rossi, and et al. 2020. "Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population" International Journal of Environmental Research and Public Health 17, no. 16: 5930. https://doi.org/10.3390/ijerph17165930
APA StyleBevilacqua, R., Casaccia, S., Cortellessa, G., Astell, A., Lattanzio, F., Corsonello, A., D’Ascoli, P., Paolini, S., Di Rosa, M., Rossi, L., & Maranesi, E. (2020). Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population. International Journal of Environmental Research and Public Health, 17(16), 5930. https://doi.org/10.3390/ijerph17165930