Navigating Life with HIV as an Older Adult in South African Communities: A Phenomenological Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Considerations
3. Findings
3.1. Participant Context
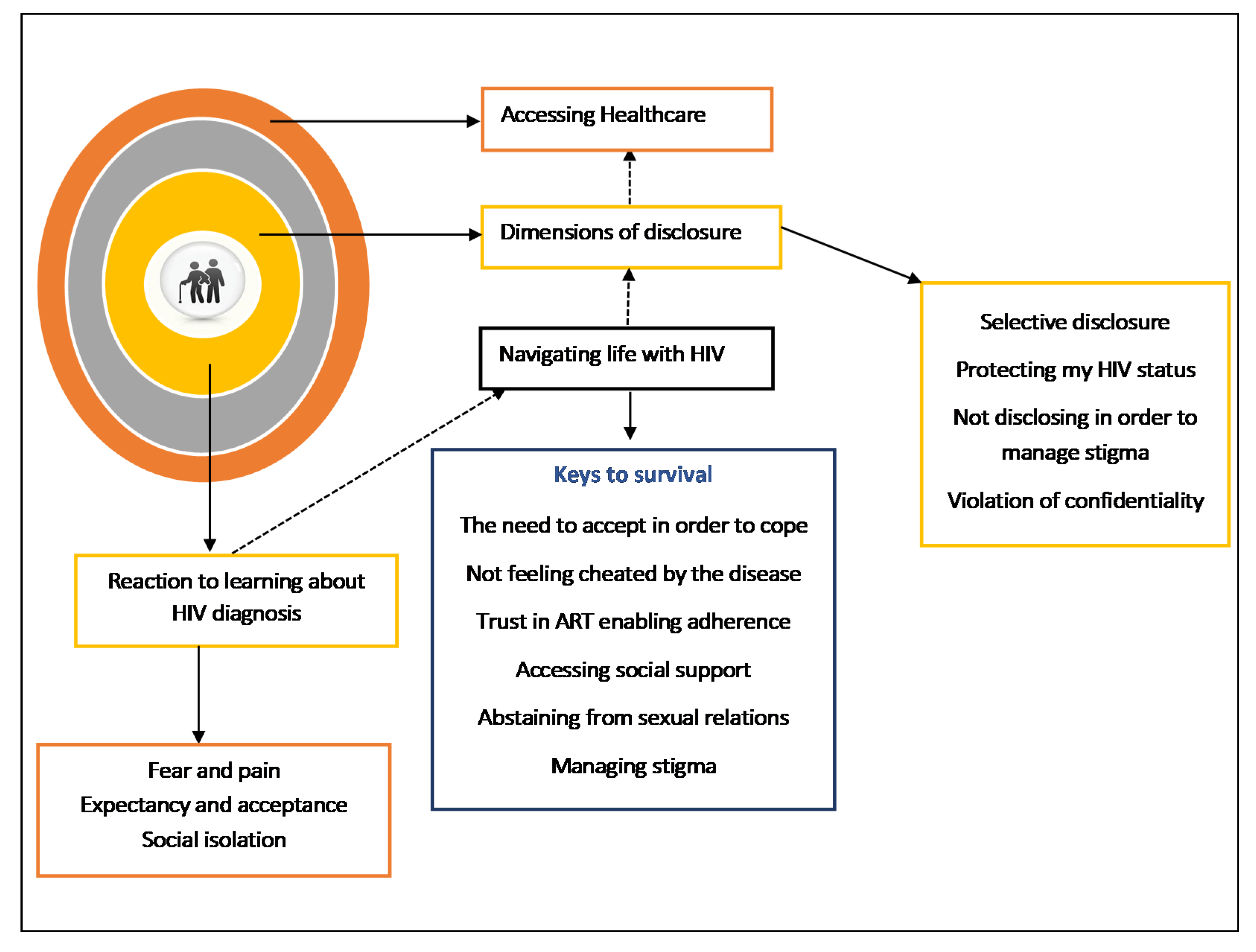
3.2. Emergent Themes
3.2.1. Reaction to Learning about the HIV Diagnosis
Fear and Pain
I felt scared because it was something that I was not ready for… Yho…. (quietness). I just told myself that from now on I would have to start taking treatment so at first; I didn’t accept the news very well because it came as a shock to me but as time goes I then accepted.(Johanna, a 58-year-old female)
Yho (sigh). I felt hurt and I wondered because my husband died and it’s now about 15 years since he passed on. They did not tell me what killed him, I thoughts that it’s just an illness. There is nothing I could do…, I told myself that I am not the only one and I will take care of myself.(Nancy a 55-year-old female)
Expectancy and Acceptance
As long as I know that my wife has been positive for long, and the time she was positive I never had that thing that I must go (leave her) because she is positive. I told myself that I accompanied her to test and she started medication. I was supporting her and when it appeared to me that I am positive, I did not have a problem.
Social Isolation
Ahh, no on my side they gossip and I don’t care about people. I don’t go visiting in people’s homes. I sit alone in my house.(Shiela a 63-year-old female)
Yho... why do I need to stress myself by going around visiting friends and neighbors because you know the people in the township talk too much so I stay home with my family.(Martha, a 53-year-old female)
3.2.2. Navigating Life with HIV
Keys to Survival
You know I just asked myself how come …, what happened to me to have HIV but still I didn’t find an answer to that question so I just told myself I had to accept there is no other way you know.(Olga, a 52-year-old female)
I have accepted and it [HIV] has become my friend and it’s just a virus. I don’t think it’s going to kill me. I will die when I want to die and provided that God has taken out my card, HIV is my brother.(Malifu, a 59-year-old female)
Living with HIV as an elderly person, it is a bit difficult. You know you feel like you are being looked down upon. And that if I am coming to collect medication (ARV’s) at my age, people take it that I am sleeping around. And when you think that you are taking care of yourself, you have one partner, it’s difficult to understand. And you just accept because there is nothing else you can do, but when you ask yourself that because I once tested and I was negative now why am I positive, how did this happen? That really bothered me. I asked myself these questions and could not get the answer as to how this happened.(Nora a 64-year-old woman)
As I have explained, I have accepted my life. I don’t perceives myself…, meaning me being HIV-positive, I don’t take it as being a problem. If I can take care of myself I will be OK just like the person who is negative.(Marriam, a 65-year-old female who has been HIV-positive for one year)
As I said before that I have accepted. Now I’m used to the idea of going to the clinic to get my treatment, and it is something that people are used to by now. It’s like a person who is diabetic.(Johanna, a 58-year-old female)
They [the nurses] said I should not worry. There was no pill back then, and it [HIV] was killing people. But, now it’s better because I can live in my age and not show any signs that I am sick. The pill is treating me well. And even when you tell someone that you are on the pill they won’t believe. I don’t give myself stress that I am sick, I accept everything that happens in my life.(Sheila, a 63-year-old female)
They [the nurses] said if you drink this medication as prescribed, you will live a long life. So from that day I told myself that since I want to live and I don’t want this illness to bring me down, I will surrender myself to the treatment and take it at the time they say I should.(Nora a 64-year-old woman)
Accessing Social Support
She [the sister] never reacted funny. She was actually the one encouraging me, even though she did not understand how did this happen because she knows what kind of a person I am. But she supported me. She was the one who brought me with her car, supporting me, when I came here for the first time, as I was sick at that time.(Nora, a 64-year-old woman)
They [the family] give me courage and always ask me if I have taken my medication yet. Like today when I came to the clinic, I live with my mother, so she asked when am I going to the clinic.(Samuel, a 59-year-old male)
The nurses give me courage that if I can continue taking my pills and not engage in unsafe sex and use protection so that I should not infect others.(Enos, a 59-year-old male)
Abstaining from Sexual Relations
When I was fist told that I am positive, I told myself this thing called a man I don’t want to see it in my life and will not find myself sleeping with one until today.(Nancy a 55-year-old female)
My husband and I have not had sex all together up to now from the time I started treatment (started ARV;’s a year ago) until now.(Marriam a 65-year-old female)
I just dealt with it-even sex. I don’t do sex anymore and is not because I don’t crave it. I do! Especially after I took my medication I crave for sex.(Samuel, a 59-year-old male, HIV-positive for six months)
Managing Stigma
When I came to test for the first time I didn’t care who was watching me and saying “What is that old lady doing here?” I came in to test …, I didn’t care about what people would say. Many of us [older people who collect ART] know each other. Even when I collect my pills, I don’t care who says what. I take them and leave.(Flora, a 60-year-old female)
People do gossip about me, more so the time when I was sick. Skinny, they were saying. Look at her she will die She has AIDS. But I didn’t care I took it as though I was injured, but they saw me as being sick when I walked in the streets because I was very skinny, and they would just talk bad about me.(Margret, a 54-year-old female, HIV-positive for one year)
3.2.3. Dimensions of Disclosure
Selective Disclosure
For me the person I told was my partner, and before I told him it was difficult for me at first, but because I live with him and he married me and he is my partner he was the first person I told. I told him that I am positive, but he accepted and he supports me.(Nora, a 64-year-old female)
It was not difficult; it was easy. As I mentioned that in my family there is already someone who is HIV positive. I didn’t hide my status from them, and they just accepted me.(Olga, a 52-year-old female)
Protecting One’s HIV Status
Not that I hide them [the medication], but I put them where I know they cannot reach.
I hide them [the medication] from the children, but I do not forget to take them. They don’t make me sick; nothing at all. Even when I go to places, my daughter will say Mama, are you leaving? You didn’t forget …, and she will call me to the corner and whisper to me “your pills”.
Not Disclosing to Manage Stigma
According to me I would not disclose to other people because when you have this illness they exclude you and ignore you, so it’s better to keep quiet.(Norman, a 55-year-old male)
I told my daughter about the HIV and we are OK, but I have not told the boys, because you know these boys get drunk, and soon he will be swearing at you on the streets.(Maria, a 57-year-old female)
Violation of Confidentiality
I disclosed to my neighbor, and when we fought, my neighbor told my husband that I was HIV-positive. But my husband did not confront me and asked me why did I not tell him that I was positive.(Marriam, a 65-year-old female who has been LHIV for one year)
I told my sister who is a nurse that I am positive. She was like, No problem, my sister. Just take your medication and you will be ok. But when I went to visit my mother, she asked me why didn’t I tell her that I was sick, which means that my sister told my mother. Since then I have not told anyone.(Joyce, a 53-year-old female who has been LHIV for a year)
3.2.4. Accessing Health Care
You can sit here [in the clinic] the whole day while they say they are looking for your file and end up not finding it. They then send you back home on foot because you do not have money for a taxi. When you come back the following day, they still cannot find your file. And you travel by foot and you find you don’t have money for food and you go back hungry.(Sheila, a 63-year-old female who has been HIV-positive for eight months)
It’s a burden. Even now I am just thinking if only they could give me medication for the next three months so I can rest a bit. It’s a long distance to come here. You wake up very early.(Nancy, a 55-year-old female)
Sometimes you come to the clinic and they don’t have needles…. They then tell you to come the following day, and when you get to the clinic there are still no needles. It can take a whole week and there still will be no needles. Then it becomes a problem at your work and people say this person is always at the clinic.(Sam, a 63-year-old male who has been HIV-positive for three years)
They treat us well… I am satisfied and I think if I was sitting at home, the information that they have here [in the clinic] I would not get from anyone.(Marriam, a 65-year-old female)
I meet other older people who come to collect their pills. We don’t have any problems. We end up having conversations here in the queue.(Gugu, a 60-year-old female)
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ellman, T.M.; Sexton, M.E.; Warshafsky, D.; Sobieszczyk, M.E.; Morrison, E.A. A forgotten population: Older adults with newly diagnosed HIV. Aids Patient Care STDs 2014, 28, 530–536. [Google Scholar] [CrossRef]
- Hontelez, J.A.; de Vlas, S.J.; Baltussen, R.; Newell, M.-L.; Bakker, R.; Tanser, F.; Lurie, M.; Bärnighausen, T. The impact of antiretroviral treatment on the age composition of the HIV epidemic in Sub-Saharan Africa. Aids 2012, 26, 19–30. [Google Scholar] [CrossRef]
- Autenrieth, C.S.; Beck, E.J.; Stelzle, D.; Mallouris, C.; Mahy, M.; Ghys, P. Global and regional trends of people living with HIV aged 50 and over: Estimates and projections for 2000–2020. PLoS ONE 2018, 13, e0207005. [Google Scholar] [CrossRef]
- Emlet, C.A. A comparison of HIV stigma and disclosure patterns between older and younger adults living with HIV/AIDS. Aids Patient Care STDs 2006, 20, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Siegel, K.; Schrimshaw, E.W.; Brown-Bradley, C.J.; Lekas, H.-M. Sources of emotional distress associated with diarrhea among late middle-age and older HIV-infected adults. J. Pain Symptom Manag. 2010, 40, 353–369. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E.; Woodley, R.A. Strengths and distress in adults who are aging with HIV: A pilot study. Psychol. Rep. 2005, 96, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Emlet, C.A.; Tozay, S.; Raveis, V.H. I’m not going to die from the AIDS”: Resilience in aging with HIV disease. Gerontology 2011, 51, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Goodkin, K.; Heckman, T.; Siegel, K.; Linsk, N.; Khamis, I.; Lee, D.; Lecusay, R.; Poindexter, C.C.; Mason, S.J.; Suarez, P. Putting a face on HIV infection/AIDS in older adults: A psychosocial context. J. Acquir. Immune Defic. Syndr. 2003, 33, S171–S184. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, T. HIV/AIDS and the older adult: An exploratory study of the age-related differences in access to medical and social services. J. Appl. Gerontol. 2005, 24, 35–54. [Google Scholar] [CrossRef]
- Schatz, E.; Seeley, J.; Negin, J.; Weiss, H.A.; Tumwekwase, G.; Kabunga, E.; Nalubega, P.; Mugisha, J. For us here, we remind ourselves: Strategies and barriers to ART access and adherence among older Ugandans. BMC Public Health 2019, 19, 131. [Google Scholar] [CrossRef]
- Foster, P.P.; Gaskins, S.W. Older African Americans’ management of HIV/AIDS stigma. Aids Care 2009, 21, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Audet, C.M.; McGowan, C.C.; Wallston, K.A.; Kipp, A.M. Relationship between HIV stigma and self-isolation among people living with HIV in Tennessee. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Lemin, A.S.; Rahman, M.M.; Pangarah, C.A. Factors affecting intention to disclose HIV status among adult population in Sarawak, Malaysia. J. Environ. Public Health 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Negin, J.; Gregson, S.; Eaton, J.W.; Schur, N.; Takaruza, A.; Mason, P.; Nyamukapa, C. Rising levels of HIV infection in older adults in Eastern Zimbabwe. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Lekalakala-Mokgele, E. Exploring gender perceptions of risk of HIV infection and related behaviour among elderly men and women of Ga-Rankuwa, Gauteng Province, South Africa. Sahara J. Soc. Asp. HIV/Aids 2016, 13, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Statistical Release. Mid-Year Population Estimates; Stats SA: Pretoria, South Africa, 2019; Volume P0302. Available online: www.statssa.gov.za (accessed on 4 April 2020).
- Dowling, M.; Cooney, A. Research approaches related to phenomenology: Negotiating a complex landscape. Nurse Res. 2012, 20, 21–27. [Google Scholar] [CrossRef]
- Giorgi, A. The theory, practice, and evaluation of the phenomenological method as a qualitative research procedure. J. Phenomenol. Psychol. 1997, 28, 235–260. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 4th ed.; Sage Publications: Los Angeles, CA, USA; London, UK; New Delhi, India; Washington, DC, USA; Melbourne, Australia, 2017. [Google Scholar]
- Patton, M.Q. Enhancing the quality and credibility of qualitative analysis. Health Serv. Res. 1999, 34, 1189. [Google Scholar]
- Patton, M.Q. Integrating theory and practice. In Qualitative Research & Evaluation Methods, 4th ed.; Sage Publications: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Converse, M. Philosophy of phenomenology: How understanding aids research. Nurse Res. 2012, 20, 28–32. [Google Scholar] [CrossRef]
- Bevan, M.T. A method of phenomenological interviewing. Qual. Health Res. 2014, 24, 136–144. [Google Scholar] [CrossRef]
- Sundler, A.J.; Lindberg, E.; Nilsson, C.; Palmér, L. Qualitative thematic analysis based on descriptive phenomenology. Nurs. Open 2019, 6, 733–739. [Google Scholar] [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo (Version 12). 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 16 June 2020).
- Guba, E.G. Criteria for assessing the trustworthiness of naturalistic inquiries. ECTJ 1981, 29, 75. [Google Scholar]
- Gearing, R.E. Bracketing in research: A typology. Qual. Health Res. 2004, 14, 1429–1452. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Shinebourne, P. Interpretative phenomenological analysis. In The SAGE Handbook of Qualitative Research in Psychology; American Psychological Association: Washington, DC, USA, 2012; Volume 2. [Google Scholar]
- Tavoschi, L.; Dias, J.G.; Pharris, A.; Schmid, D.; Sasse, A.; Van Beckhoven, D.; Varleva, T.; Blazic, T.N.; Hadjihannas, L.; Koliou, M. New HIV diagnoses among adults aged 50 years or older in 31 European Countries, 2004–15: An analysis of surveillance data. Lancet HIV 2017, 4, e514–e521. [Google Scholar] [CrossRef]
- Harris, T.G.; Rabkin, M.; El-Sadr, W.M. Achieving the fourth 90: Healthy aging for people living with HIV. Aids 2018, 32, 1563. [Google Scholar] [CrossRef]
- Grodensky, C.A.; Golin, C.E.; Jones, C.; Mamo, M.; Dennis, A.C.; Abernethy, M.G.; Patterson, K.B. I should know better: The roles of relationships, spirituality, disclosure, stigma, and shame for older women living with HIV seeking support in the South. J. Assoc. Nurses Aids Care 2015, 26, 12–23. [Google Scholar] [CrossRef]
- Kuteesa, M.O.; Wright, S.; Seeley, J.; Mugisha, J.; Kinyanda, E.; Kakembo, F.; Mwesigwa, R.; Scholten, F. Experiences of HIV-related stigma among HIV-positive older persons in Uganda—A mixed methods analysis. Sahara-J.: J. Soc. Asp. HIV/Aids 2014, 11, 126–137. [Google Scholar] [CrossRef]
- Yoo-Jeong, M.; Hepburn, K.; Holstad, M.; Haardörfer, R.; Waldrop-Valverde, D. Correlates of loneliness in older persons living with HIV. Aids Care 2019, 32, 1–8. [Google Scholar] [CrossRef]
- Emlet, C.A.; Brennan, D.J.; Brennenstuhl, S.; Rueda, S.; Hart, T.A.; Rourke, S.B. The impact of HIV-related stigma on older and younger adults living with HIV disease: Does age matter? Aids Care 2015, 27, 520–528. [Google Scholar] [CrossRef]
- Cook, C.L.; Canidate, S.; Ennis, N.; Cook, R.L. Types and delivery of emotional support to promote linkage and engagement in HIV care. Patient Prefer. Adherence 2018, 12, 45. [Google Scholar] [CrossRef]
- Vervoort, S.C.; Grypdonck, M.H.; De Grauwe, A.; Hoepelman, A.I.; Borleffs, J.C. Adherence to HAART: Processes explaining adherence behavior in acceptors and non-acceptors. Aids Care 2009, 21, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Skinner, E.A.; Edge, K.; Altman, J.; Sherwood, H. Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychol. Bull. 2003, 129, 216. [Google Scholar] [CrossRef] [PubMed]
- Quinn, K.; Sanders, C.; Petroll, A.E. HIV is not going to kill me, old age is!: The intersection of aging and HIV for older HIV-infected adults in rural communities. Aids Educ. Prev. 2017, 29, 62–76. [Google Scholar] [CrossRef] [PubMed]
- Emlet, C.A. Truth and consequences: A qualitative exploration of HIV disclosure in older adults. Aids Care 2008, 20, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Quinn, K.G.; Murphy, M.K.; Nigogosyan, Z.; Petroll, A.E. Stigma, isolation and depression among older adults living with HIV in rural areas. Ageing Soc. 2020, 20, 1352–1370. [Google Scholar] [CrossRef]
- Emlet, C.A.; Harris, L.; Furlotte, C.; Brennan, D.J.; Pierpaoli, C.M. I’m happy in my life now, I’m a positive person: Approaches to successful ageing in older adults living with HIV in Ontario, Canada. Ageing Soc. 2017, 37, 2128–2151. [Google Scholar] [CrossRef]
- Frisoli, A. The South African Elderly: Neglect, Social Contribution and the HIV/AIDS Epidemic. Ph.D. Thesis, City University of New York, New York, NY, USA, 2016. [Google Scholar]
- Hosegood, V.; Timaeus, I.M. HIV/AIDS and older people in South Africa. In Aging in Sub-Saharan Africa: Recommendations for Furthering Research; National Academies Press: Washington, DC, USA, 2006; p. 250. [Google Scholar]


{kind=link}
| Variables | Categories | Frequency | Percentage |
|---|---|---|---|
| Gender | Male | 5 | 25.0 |
| Female | 15 | 75.0 | |
| Age group | 50–55 | 3 | 15.0 |
| 56–60 | 8 | 40.0 | |
| Above 60 | 9 | 45.0 | |
| Marital status | Single | 3 | 15.0 |
| Married | 11 | 55.0 | |
| Widowed | 6 | 30.0 | |
| Educational attainment | No formal schooling | 3 | 15.0 |
| Primary education | 4 | 20.0 | |
| Secondary education and above | 13 | 55.0 | |
| Employment | Employed | 6 | 30.0 |
| Unemployed | 14 | 70.0 | |
| Duration on ART | Less than 2 years | 9 | 45.0 |
| 3–5 years | 11 | 55.0 | |
| Other chronic conditions | Yes | 12 | 60.0 |
| No | 8 | 40.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hlongwane, N.; Madiba, S. Navigating Life with HIV as an Older Adult in South African Communities: A Phenomenological Study. Int. J. Environ. Res. Public Health 2020, 17, 5797. https://doi.org/10.3390/ijerph17165797
Hlongwane N, Madiba S. Navigating Life with HIV as an Older Adult in South African Communities: A Phenomenological Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5797. https://doi.org/10.3390/ijerph17165797
Chicago/Turabian StyleHlongwane, Naomi, and Sphiwe Madiba. 2020. "Navigating Life with HIV as an Older Adult in South African Communities: A Phenomenological Study" International Journal of Environmental Research and Public Health 17, no. 16: 5797. https://doi.org/10.3390/ijerph17165797
APA StyleHlongwane, N., & Madiba, S. (2020). Navigating Life with HIV as an Older Adult in South African Communities: A Phenomenological Study. International Journal of Environmental Research and Public Health, 17(16), 5797. https://doi.org/10.3390/ijerph17165797