A Review: The Prospect of Inhaled Insulin Therapy via Vibrating Mesh Technology to Treat Diabetes


{kind=link}
{kind=link}
Abstract
1. Aerosol Therapy
1.1. Aerosol Droplet Size
1.2. Aerosol Deposition Mechanisms
1.3. Anatomy of the Airways
2. Objectives
- To review the failures and shortcomings of current inhaled insulin therapy.
- To review the suitability of vibrating mesh nebulisers to administer inhaled insulin effectively.
- To define the aerosol flow rate and droplet size to treat type-II diabetes effectively using a vibrating mesh nebulisers.
3. Insulin Therapy
3.1. Inhaled Insulin: Devices Development
3.1.1. AERx iDMS
3.1.2. Exubera
3.1.3. AIR
3.1.4. Afrezza
3.2. Clinical Trials: Afrezza Inhalable Insulin
3.2.1. Hypoglycaemia
3.2.2. Weight Gain
3.2.3. Persistent Cough
3.2.4. Patient Satisfaction of Afrezza Inhalable Insulin
3.2.5. Insulin Administration and Dosing
4. Review of Inhaled Insulin Delivery Devices
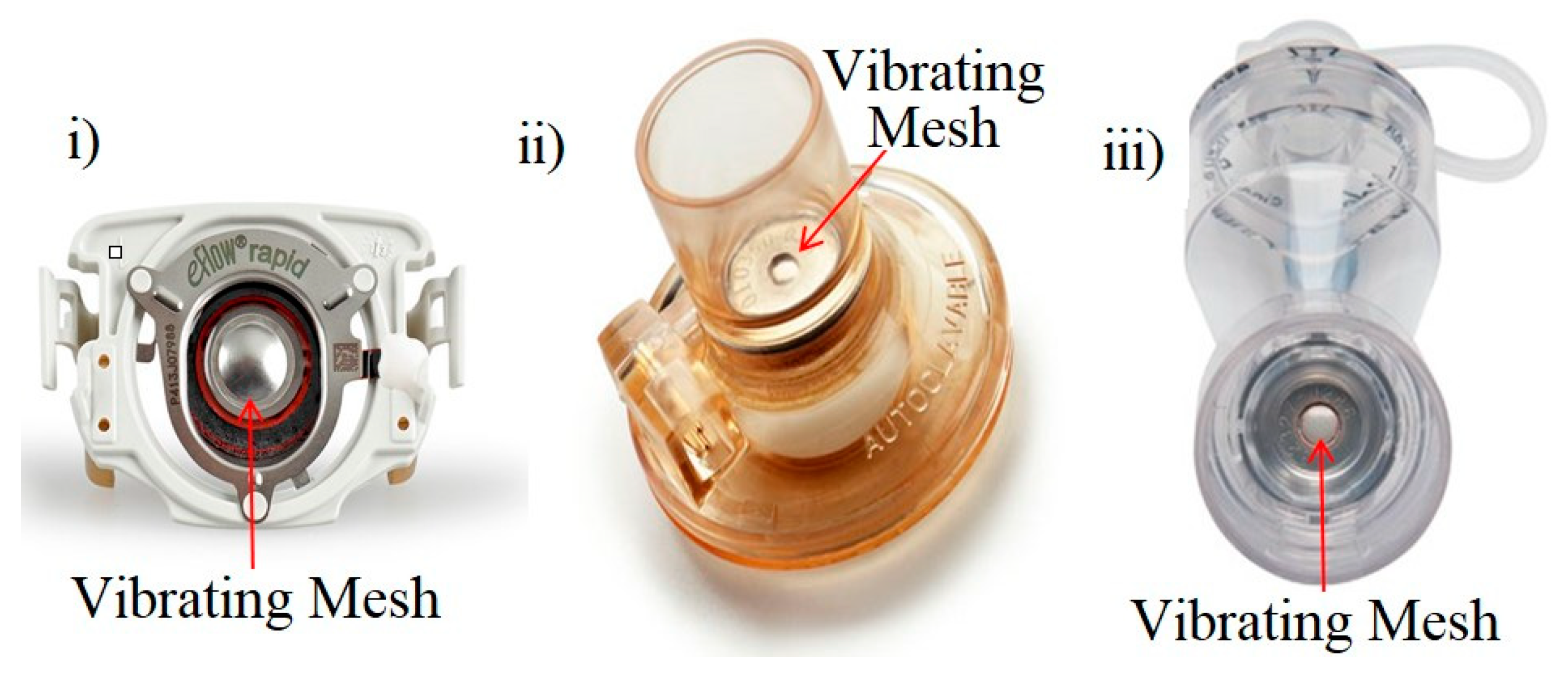
4.1. Vibrating Mesh Technology
4.1.1. Published Clinical Trials: VMN for Topical Applications
4.1.2. Published Clinical Trials: The Dance 501 VMN Inhaled Insulin
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| A1C | Average haemoglobin level over three months |
| CSII | Continuous subcutaneous insulin infusion |
| CMax | Maximal insulin concentration |
| DPI | Dry powder inhaler |
| EDIC | Epidemiology of diabetes interventions and complications |
| FDA | Food and Drug Administration |
| HbA1c | Average glycated haemoglobin level |
| ICU | Intensive care unit |
| iDMS | Insulin diabetes management system |
| IU | Insulin unit |
| pMDI | Pressurised metered dose inhalers |
| RD | Respirable dose |
| SMI | Soft mist inhaler |
| SVN | Small-volume inhaler |
| T1DM | Type-1 diabetes |
| T2DM | Type-1 diabetes |
| TI | Technosphere insulin |
| VMN | Vibrating mesh nebuliser |
References
- Sanders, M. An Historical Overview; Pulmonary Drug Delivery: New York, NY, USA, 2011; pp. 51–73. [Google Scholar]
- Merriam-Webster. 2018. Available online: Merriam-Webster.com (accessed on 30 July 2020).
- Finlay, W.H. The Mechanics of Inhaled Pharmaceutical Aerosols; Academic Press, University of Alberta: Edmonton, AB, Canada, 2019. [Google Scholar]
- Kendrick, A. Nebulisers: Back to the future. The buyers guide to respiratory care product. Transl. Respir. Med. 2001, 2, 28–34. [Google Scholar]
- Lewis, R.A.; Fleming, J. Fractional deposition from a jet nebulizer: How it differs from a metered-dose inhaler. Br. J. Diseases Chest 1985, 79, 361–367. [Google Scholar] [CrossRef]
- Xu, Z.; Hickey, A.J. The Physics of Aerosol Droplet and Particle Generation from Inhalers. In Controlled Pulmonary Drug Delivery; Springer: New York, NY, USA, 2011; pp. 75–100. [Google Scholar]
- Djupesland, P.G. Nasal drug delivery devices: Characteristics and performance from a clinical perspective—A review. Drug Deliv. Transl. Res. 2013, 3, 42–62. [Google Scholar] [CrossRef] [PubMed]
- Le Brun, P.; De Boer, A.H.; Frijlink, H.W.; Heijerman, H. A review of the technical aspects of drug nebulization. Pharm. World Sci. 2000, 22, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Hess, D. Nebulizers: Principles and performance. Respir Care 2000, 45, 609–622. [Google Scholar] [PubMed]
- Van Hoeve, W.; Gekle, S.; Snoeijer, J.H.; Versluis, M.; Brenner, M.P.; Lohse, D. Breakup of diminutive Rayleigh jets. Phys. Fluids 2010, 22, 1–17. [Google Scholar] [CrossRef]
- Eggers, J.; Villermaux, E. Physics of liquid jets. Rep. Prog. Phys. 2008, 71, 36601. Available online: http://stacks.iop.org/0034-4885/71/i=3/a=036601 (accessed on 30 July 2020). [CrossRef]
- O’Donnell, K.P.; Smyth, H.D. Macro- and Microstructure of the Airways for Drug Delivery; Springer: New York, NY, USA, 2011; pp. 1–19. [Google Scholar]
- White, D. The pathogenesis of obstructive sleep apnoea: Advances in the past 100 years. Am. J. Respir. Cell Mol. Biol. 2006, 34, 1–6. [Google Scholar] [CrossRef]
- Altiere, R.J. Physiology and pharmacology of the airways. Inf. Healthc. 2007, 24, 83–126. [Google Scholar]
- Shelly, M.P.; Lloyd, G.M.; Park, G.R. A review of the mechanisms and methods of humidification of inspired gases. Intensive Care Med. 1988, 14, 1–9. [Google Scholar] [CrossRef]
- Marfatia, S.; Donahoe, P.K.; Hendren, W.H. Effect of dry and humidified gases on the respiratory epithelium in rabbits. J. Paediatr. Surg. 1975, 10, 583. [Google Scholar] [CrossRef]
- Tamer, M.A.; Modell, J.H. Hyponatremia secondary to ultrasonic aerosol therapy in the new-born infant. J. Pediatr. 1970, 77, 93–99. [Google Scholar] [CrossRef]
- Patton, J. Mechanisms of macromolecule absorption by the lungs. Adv. Drug Deliv. Rev. 1996, 19, 3–36. [Google Scholar] [CrossRef]
- Patton, J.S. Inhaling medicines: Delivering drugs to the body through the lungs. Nat. Rev. 2007, 6, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Ireland. What is Diabetes; Diabetes Ireland: Dublin, Ireland, 2019; Available online: https://www.diabetes.ie/about-us/what-is-diabetes/ (accessed on 30 July 2020).
- Control, D. National Diabetes Fact Sheet: General Information and National Estimates on Diabetes in the United States, US Department of Health and Human Services; Centres for Disease Control and Prevention, CDC: Atlanta, GA, USA, 2014. [Google Scholar]
- Mastrandrea, L.D. Inhaled insulin: An overview of a novel route of insulin administration. Vasc. Health Risk Manag. 2010, 6, 47–58. [Google Scholar] [CrossRef]
- WebMD, Diabetes Overview; Diabetes Healthcare Center: USA, 2017; Volume 1, Available online: https://www.webmd.com/diabetes/guide/diabetes-general-overview-facts (accessed on 30 July 2020).
- Kalra, S. Oral insulin. Diabetol. Metab. Syndr. 2010, 6, 66. [Google Scholar] [CrossRef]
- Tesauro, M.; Leo, R.; Lauro, R.; Cardillo, C. Endothelial dysfunction and diabetes: Roles of hyperglycaemia, impaired insulin signalling and obesity. Cell Tissue Res 2009, 335, 165–189. [Google Scholar]
- Stamler, J.; Vaccaro, O.; Neaton, J.D.; Wentworth, D. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the multiple risk factor intervention trial. Diabetes Care 1993, 16, 434–444. [Google Scholar] [CrossRef]
- Andrzej, S.; Krolewski, E.J.K. Magnitude and determinants of coronary artery disease in juvenile-onset, insulin-dependent diabetes mellitus. Am. J. Cardiol. 1987, 59, 750–755. [Google Scholar]
- Laing, S.P.; Swerdlow, A.J. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetology 2003, 46, 760–765. [Google Scholar] [CrossRef]
- Diabetes Control and Complications Trial Research Group. Effect of intensive diabetes treatment on the development and progression of long-term complications in adolescents with insulin-dependent diabetes mellitus: Diabetes control and complications trial. J. Paediatr. 1994, 125, 177–188. Available online: http://www.sciencedirect.com/science/article/pii/S0022347694701903 (accessed on 30 July 2020). [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type-II Diabetes. The Lancet 1998, 352, 837–853. [Google Scholar]
- Zambanini, A.; Newson, R.B.; Maisey, M.; Feher, M.D. Injection related anxiety in insulin-treated diabetes. Diabetes Res. Clin. Pract. 1999, 46, 239–246. [Google Scholar] [CrossRef]
- Logtenberg, S.J.; Kleefstra, N.H.S. Improved glycaemic control with intraperitoneal versus subcutaneous insulin in type-I diabetes: A randomized controlled trial. Diabetes Care 2009, 32, 1372–1377. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.; Bliss, M. The Discovery of Insulin. Am. Hist. Rev. 1983, 88, 964. Available online: https://books.google.ie/books?id=ii0pAQAAIAAJ (accessed on 30 July 2020). [CrossRef]
- Patton, J.S.; Bukar, J.G.; Eldon, M.A.; Patton, J.S. Clinical pharmacokinetics and pharmacodynamics of inhaled insulin. Clin. Pharmacokinet. 2004, 43, 781–801. [Google Scholar] [CrossRef]
- Brunner, G.A.; Balent, B. Dose-response relation of liquid aerosol inhaled insulin in type I diabetic patients. Diabetology 2001, 44, 305–308. [Google Scholar] [CrossRef][Green Version]
- Rave, K.; Heise, T. Coverage of postprandial blood glucose excursions with inhaled Technosphere insulin in comparison to subcutaneously injected regular human insulin in subjects with type-II diabetes. Diabetes Care 2007, 30, 2307–2308. Available online: http://care.diabetesjournals.org/content/30/9/2307 (accessed on 30 July 2020). [CrossRef]
- Food and Drug Administration. FDA Approves First-Ever Inhaled Insulin Combination Product for the Treatment of Diabetes; Food and Drug Administration, FDA: Silver Spring, MD, USA, 2006; Volume 1, pp. 1–10. Available online: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucm108585.htm (accessed on 30 July 2020).
- Rosenstock, J.; Bergenstal, R. Efficacy and safety of Technosphere inhaled insulin compared with Technosphere powder placebo in insulin-naive type-II diabetes suboptimal controlled with oral agents. Diabetes Care 2008, 31, 2177–2182. Available online: http://care.diabetesjournals.org/content/31/11/2177 (accessed on 30 July 2020). [CrossRef]
- NLM Clinical Trial Evaluating the Efficacy and Safety of Technosphere Inhalation Insulin (TI) Inhalation Powder Using the Gen2 Inhaler; NLM: National Library of Medicine: Bethesda, MD, USA, 2015. Available online: https://www.clinicaltrials.gov/ct2/show/NCT01196104 (accessed on 30 July 2020).
- Harsh, Q. What is the difference between inhaled insulin and syringe one and do they act differently on a diabetic patient? Pharm. Ther. 2017, 1, 1–12. Available online: www.quora.com/Whats-the-difference-between-inhaled-insulin-and-syringe-one-and-do-they-act-differently-on-a-diabetic-patient (accessed on 30 July 2020).
- Food and Drug Administration. FDA Approves Afrezza to Treat Diabetes; Food and Drug Administration: Silver Spring, MD, USA, 2014; Volume 1, pp. 1–12. Available online: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm403122.htm (accessed on 30 July 2020).
- Steiner, S.; Pfützner, A. Technosphere/insulin—Proof of concept study with a new insulin formulation for pulmonary delivery. Exp. Clin. Endocrinol. Diabetes 2002, 110, 17–21. [Google Scholar] [CrossRef]
- Rosenstock, J.; Lorber, D.L. Prandial inhaled insulin plus basal insulin glargine versus twice-daily bias part insulin for type-II diabetes: A multicentre randomised trial. Lancet 2010, 375, 2244–2253. [Google Scholar] [CrossRef]
- Raskin, P.; Heller, S. Pulmonary function over two years in diabetic patients treated with prandial inhaled Technosphere insulin or usual antidiabetic treatment: A randomized trial. Diabetes Obes. Metab. 2012, 14, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, J.P.; Amin, N. Insulin lung deposition and clearance following Technosphere insulin inhalation powder administration. Pharm. Res. 2011, 28, 2157–2164. [Google Scholar] [CrossRef] [PubMed]
- Rave, K.; Heise, T. Inhaled Technosphere insulin in comparison to subcutaneous regular human insulin: Time action profile and variability in subjects with type-II diabetes. J. Diabetes Sci. Technol. 2008, 2, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Pfützner, A.; Forst, T. Pulmonary insulin delivery by means of the Technosphere drug carrier mechanism. Expert Opin. Drug Deliv. 2005, 2, 1097–1106. [Google Scholar] [CrossRef]
- Brain, J.; Finch, G.L. Trough insulin levels in bronchoalveolar lavage following inhalation of human insulin (Exubera) in patients with diabetes mellitus. Am. Thorac. Soc. Annu. Meet. 2008, 1, 16–21. [Google Scholar]
- Turner, R. Glycaemic control with diet, sulfonylurea, metformin, or insulin in patients with type-II diabetes mellitus: Progressive requirement for multiple therapies (UKPDS 49). JAMA 1999, 281, 2005–2012. [Google Scholar] [CrossRef]
- Control, T.D.; Group, C.T.R. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar]
- NLM. Efficacy and Safety of Inhaled Insulin in Type-I Diabetes; NLM: National Library of Medicine: Bethesda, MD, USA, 2015. Available online: https://clinicaltrials.gov/ct2/show/study/NCT00308308 (accessed on 30 July 2020).
- Tack, C.J.; Christov, V. Randomized forced titration to different doses of Technosphere insulin demonstrates reduction in postprandial glucose excursions and haemoglobin a1c in patients with type-II diabetes. J. Diabetes Sci. Technol. 2008, 2, 47–57. [Google Scholar] [CrossRef]
- NLM. Healthy Normal Volunteers Looking at Exposure and Effects of Multiple Doses of Technosphere Insulin (TI) Using the Gen2c Inhale; NLM: National Library of Medicine: Bethesda, MD, USA, 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT01490762 (accessed on 30 July 2020).
- FDA Afrezza. Food and Drug Administration (FDA) Approved Product Information; National Library of Medicine: Bethesda, MD, USA, 2014. Available online: www.dailymed.nlm.nih.gov (accessed on 30 July 2020).
- NLM. A phase 3, Multicentre, Open-Label, Randomized, Forced-Titration Clinical Trial Evaluating the Efficacy and Safety of Technosphere Insulin Inhalation Powder in Combination with a Basal Insulin Versus Insulin as Part in Combination with a Basal Insulin in Subjects with Type-I Diabetes Mellitus over a 24-Week Treatment Period; NLM: National Library of Medicine: Bethesda, MD, USA, 2014. Available online: https://clinicaltrials.gov/ct2/show/NCT01445951 (accessed on 30 July 2020).
- NLM. Efficacy and Safety of Prandial Inhalation of Technosphere/Insulin in Combination with Metformin or Technosphere Insulin Alone versus Two Oral Anti-Diabetic Agents in Subjects with Type-II Diabetes; NLM: National Library of Medicine: Bethesda, MD, USA, 2015. [Google Scholar]
- Pittas, A.G. Efficacy, safety, and patient acceptability of Technosphere inhaled insulin for people with diabetes: A systematic review and meta-analysis. Diabetes Endocrinol. 2015, 3, 886–894. [Google Scholar] [CrossRef]
- NLM. An Open-Label, Multi-Center, International, Three-Year, Safety and Tolerability Follow on Trial; NLM: National Library of Medicine: Bethesda, MD, USA, 2015. [Google Scholar]
- Barnett, A.H.; Dreyer, A. An open, randomized, parallel-group study to compare the efficacy and safety profile of inhaled human insulin (Exubera) with metformin as adjunctive therapy in patients with type-II diabetes poorly controlled on a sulfonylurea. Diabetes Care 2006, 29, 1282–1287. Available online: http://care.diabetesjournals.org/content/29/6/1282 (accessed on 30 July 2020). [CrossRef] [PubMed]
- Rosenstock, J.; Zinman, B.; Murphy, L.J. Inhaled insulin improves glycaemic control when substituted for or added to oral combination therapy in type-II diabetes: A randomized, controlled trial. Ann. Intern. Med. 2005, 143, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.R.; Cheng, S.L. Inhaled insulin provides improved glycaemic control in patients with type-II diabetes mellitus inadequately controlled with oral agents: A randomized controlled trial. Arch. Intern. Med. 2003, 163, 2277–2282. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Freemantle, N.; Blonde, N. Availability of inhaled insulin promotes greater perceived acceptance of insulin therapy in patients with type-II diabetes. Diabetes Care 2005, 28, 427–428. Available online: http://care.diabetesjournals.org/content/28/2/427 (accessed on 30 July 2020). [CrossRef][Green Version]
- Peyrot, M.; Rubin, R.R. Effect of Technosphere inhaled insulin on quality of life and treatment satisfaction. Diabetes Technol. Ther. 2010, 12, 49–55. [Google Scholar] [CrossRef]
- Peyrot, M.; Rubin, R.R. Patient-reported outcomes in adults with type-II diabetes using mealtime inhaled Technosphere insulin and basal insulin versus premixed insulin. Diabetes Technol. Ther. 2011, 13, 1201–1206. [Google Scholar] [CrossRef]
- Martin, A.R.; Finlay, W.H. Nebulizers for drug delivery to the lungs. Expert Op. Drug Deliv. 2015, 889–900. [Google Scholar] [CrossRef]
- Aerogen. Aerogen Pro; Aerogen: Galway, Ireland, 2015; Available online: www.omniagmd.com/product/aerogen-pro (accessed on 30 July 2020).
- Dubus, J.C.; Vecellio, L.; De Monte, M.; Fink, J.B. Aerosol Depos. Neonatal Vent. Pediatric Res. 2005, 25, 10. [Google Scholar]
- PARI. eFlow Rapid Aerosol Head; PARI: Starnberg, Germany, 2015; Available online: www.pari.com/uk-en/products/spare-parts/eflow-rapid-aerosol-head-1/ (accessed on 30 July 2020).
- Newman, S.P.; Weisz, A.W. Improvement of drug delivery with a breath-actuated pressurised aerosol for patients with poor inhaler technique. Thorax 1991, 46, 712–716. [Google Scholar] [CrossRef]
- Ari, A. Jet, ultrasonic, and mesh nebulizers: An evaluation of nebulizers for better clinical outcome. Eurasian J. Pulmonol. 2014, 16, 1–7. [Google Scholar] [CrossRef]
- Ari, A.; Fink, J.B. Factors affecting bronchodilator delivery in mechanically ventilated adult. Nurs. Crit. Care 2010, 15, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Berlinski, A. Nebulized albuterol delivery in a model of spontaneously breathing children with tracheostom. Respir Care 2013, 58, 2076–2086. [Google Scholar] [CrossRef] [PubMed]
- Holmes-Truscott, E.; Skinner, T. Negative appraisals of insulin therapy are common among adults with type-II diabetes using insulin: Results from diabetes miles—Australia cross-sectional surve. Diabet. Med. 2015, 32, 1297–1303. [Google Scholar] [CrossRef]
- Fink, J.B.; Molloy, L. Good Things in Small Packages: An Innovative Delivery Approach for Inhaled Insuli. Pharm. Res. 2017, 34, 2568–2578. [Google Scholar] [CrossRef] [PubMed]
- McGill, J.B.; Ahn, D. Making Insulin Accessible: Does Inhaled Insulin Fill an Unmet Need? Adv. Ther. 2016, 33, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Gowtham, T.; Rafi Khan, P. Facts on inhaled insulin. J. Appl. Pharm. Sci. 2011, 12, 18–23. [Google Scholar]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunningham, S.M.; Tanner, D.A. A Review: The Prospect of Inhaled Insulin Therapy via Vibrating Mesh Technology to Treat Diabetes. Int. J. Environ. Res. Public Health 2020, 17, 5795. https://doi.org/10.3390/ijerph17165795
Cunningham SM, Tanner DA. A Review: The Prospect of Inhaled Insulin Therapy via Vibrating Mesh Technology to Treat Diabetes. International Journal of Environmental Research and Public Health. 2020; 17(16):5795. https://doi.org/10.3390/ijerph17165795
Chicago/Turabian StyleCunningham, Seán M., and David A. Tanner. 2020. "A Review: The Prospect of Inhaled Insulin Therapy via Vibrating Mesh Technology to Treat Diabetes" International Journal of Environmental Research and Public Health 17, no. 16: 5795. https://doi.org/10.3390/ijerph17165795
APA StyleCunningham, S. M., & Tanner, D. A. (2020). A Review: The Prospect of Inhaled Insulin Therapy via Vibrating Mesh Technology to Treat Diabetes. International Journal of Environmental Research and Public Health, 17(16), 5795. https://doi.org/10.3390/ijerph17165795