Epidemiologic Characteristics of Domestic Patients with Hemorrhagic Fever with Renal Syndrome in Taiwan: A 19-Year Retrospective Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Policy
2.2. Definition of Confirmed Cases
2.3. Data Source
2.4. Data Analysis
3. Results
3.1. Study Population
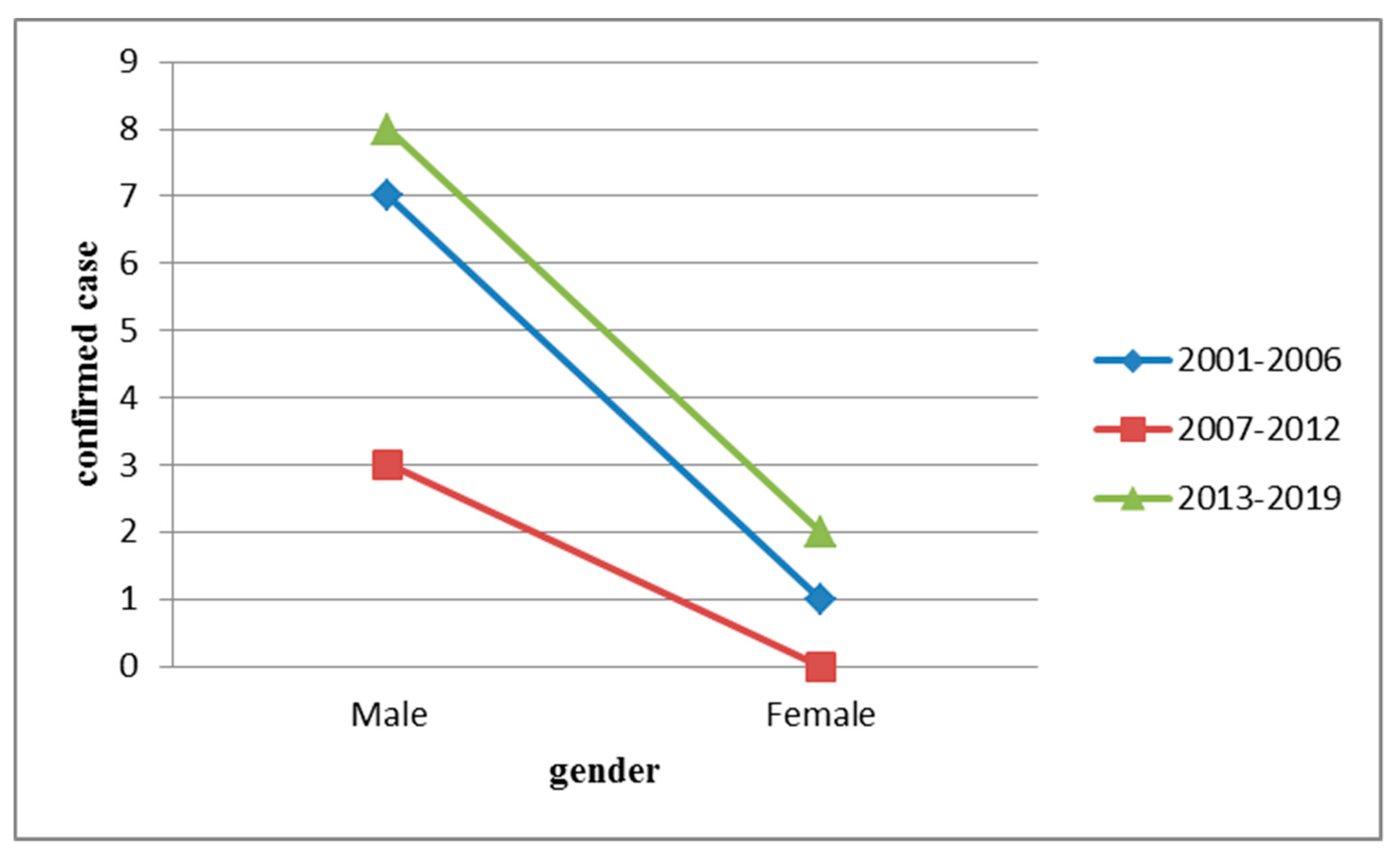
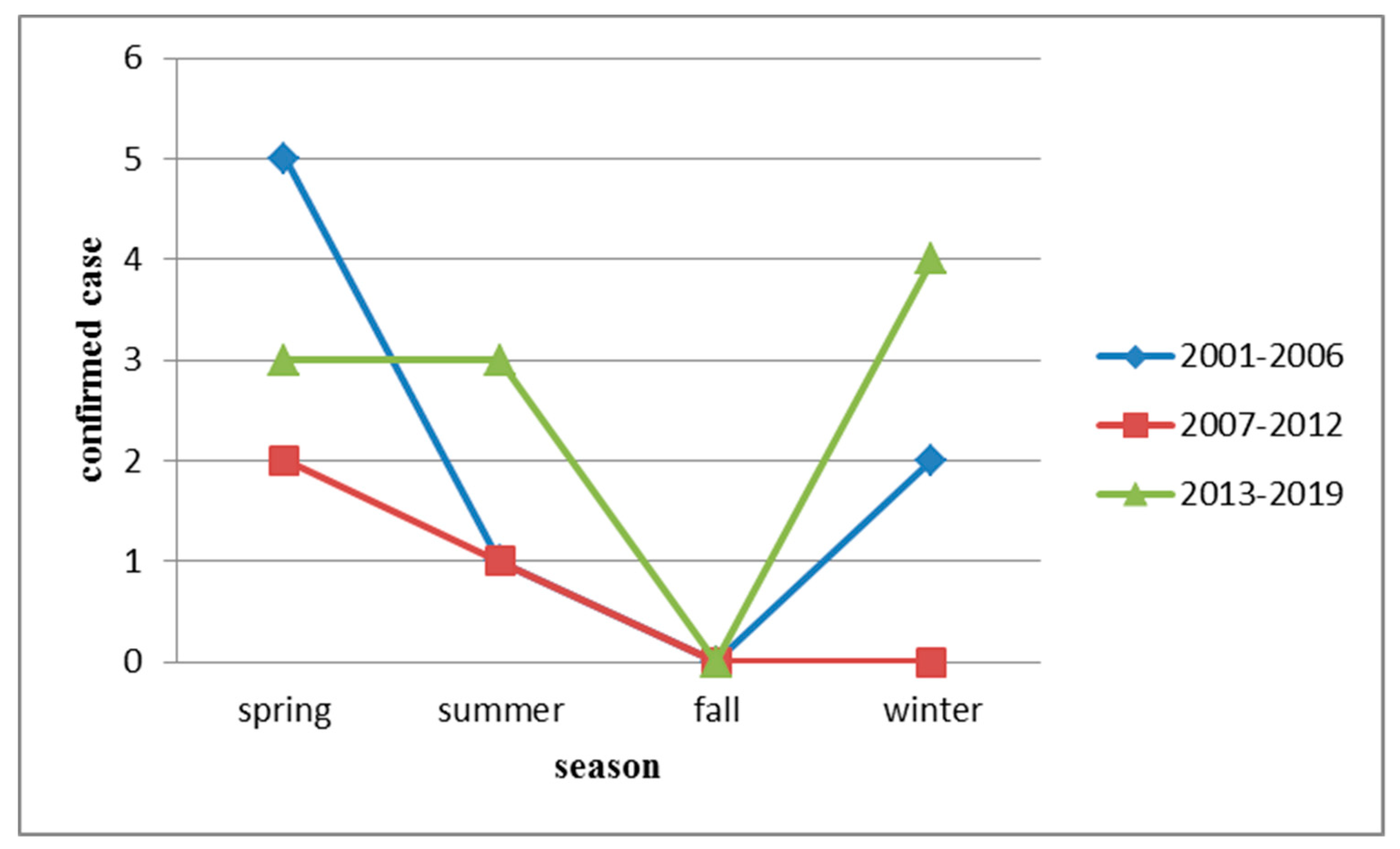
3.2. Epidemiological Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jiang, H.; Zheng, X.; Wang, L.; Du, H.; Wang, P.; Bai, X. Hantavirus infection: A global zoonotic challenge. Virol. Sin. 2017, 32, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Ling, J.; Verner-Carlsson, J.; Eriksson, P.; Plyusnina, A.; Löhmus, M.; Järhult, J.D.; van de Goot, F.; Plyusnin, A.; Lundkvist, Å.; Sironen, T. Genetic analyses of Seoul hantavirus genome recovered from rats (Rattus norvegicus) in the Netherlands unveils diverse routes of spread into Europe. J. Med. Virol. 2019, 91, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Chandy, S.; Mathai, D. Globally emerging hantaviruses: An overview. Indian J. Med. Microbiol. 2017, 35, 165. [Google Scholar] [PubMed]
- Jiang, H.; Du, H.; Wang, L.M.; Wang, P.Z.; Bai, X.F. Hemorrhagic fever with renal syndrome: Pathogenesis and clinical picture. Front. Cell. Infect. Microbiol. 2016, 6, 1. [Google Scholar] [CrossRef]
- Plyusnin, A.; Vaheri, A.; Lundkvist, Å. Saaremaa hantavirus should not be confused with its dangerous relative, Dobrava virus. J. Clin. Microbiol. 2006, 44, 1608–1611. [Google Scholar] [CrossRef]
- Avšič-Županc, T.; Saksida, A.; Korva, M. Hantavirus infections. Clin. Microbiol. Infect. 2013. [Google Scholar] [CrossRef]
- Li, Q.; Cai, Y.; Wei, Y.; Han, X.; Han, Z.; Zhang, Y.; Qi, S.; Xu, Y. Genovariation study of hantavirus in main endemic areas of hemorrhagic fever with renal syndrome in Hebei province, China. PLoS ONE 2016, 11, e0159731. [Google Scholar] [CrossRef]
- Clement, J.; Maes, P. Acute kidney injury and hantavirus disease. In Oxford Textbook of Clinical Nephrology, 4th ed.; Turner, N., Lameire, N., Eds.; Oxford University Press: Oxford, UK, 2015; pp. 2059–2066. ISBN 978-0-1995-9254-8. [Google Scholar]
- Cunze, S.; Kochmann, J.; Kuhn, T.; Frank, R.; Dörge, D.D.; Klimpel, S. Spatial and temporal patterns of human Puumala virus (PUUV) infections in Germany. PeerJ 2018, 6, e4255. [Google Scholar] [CrossRef]
- Bai, Y.; Xu, Z.; Lu, B.; Sun, Q.; Tang, W.; Liu, X.; Yang, W.; Xu, X.; Liu, Q. Effects of climate and rodent factors on hemorrhagic fever with renal syndrome in Chongqing, China, 1997–2008. PLoS ONE 2015, 10, e0133218. [Google Scholar] [CrossRef]
- Hansen, A.; Cameron, S.; Liu, Q.; Sun, Y.; Weinstein, P.; Williams, C.; Han, G.-S.; Bi, P. Transmission of haemorrhagic fever with renal syndrome in china and the role of climate factors: A review. Int. J. Infect. Dis. 2015, 33, 212–218. [Google Scholar] [CrossRef]
- Duggan, J.; Close, R.; McCann, L.; Wright, D.; Keys, M.; McCarthy, N.; Mannes, T.; Walsh, A.; Charlett, A.; Brooks, T. A seroprevalence study to determine the frequency of hantavirus infection in people exposed to wild and pet fancy rats in England. Epidemiol. Infect. 2017, 145, 2458–2465. [Google Scholar] [CrossRef] [PubMed]
- Çelebi, G.; Öztoprak, N.; Öktem, İ.M.A.; Heyman, P.; Lundkvist, Å.; Wahlström, M.; Köktürk, F.; Pişkin, N. Dynamics of Puumala hantavirus outbreak in Black Sea Region, Turkey. Zoonoses Public Health 2019, 66, 783–797. [Google Scholar] [CrossRef] [PubMed]
- Hemorrhagic Fever with Renal Syndrome. Taiwan: Taiwan Centers for Disease Control. Available online: https://nidss.cdc.gov.tw/en/SingleDisease.aspx?dc=1&dt=2&disease=0786 (accessed on 15 December 2019).
- McArthur, D.B. Emerging Infectious Diseases. Nurs. Clin. 2019, 54, 297–311. [Google Scholar] [CrossRef] [PubMed]
- Jánová, E. Emerging and threatening vector-borne zoonoses in the world and in Europe: A brief update. Pathog. Glob. Health 2019, 113, 49–57. [Google Scholar] [CrossRef]
- Maxwell, M.J.; Freire de Carvalho, M.H.; Hoet, A.E.; Vigilato, M.A.; Pompei, J.C.; Cosivi, O.; del Rio Vilas, V.J. Building the road to a regional zoonoses strategy: A survey of zoonoses programmes in the Americas. PLoS ONE 2017, 12, e0174175. [Google Scholar] [CrossRef]
- Forbes, K.M.; Sironen, T.; Plyusnin, A. Hantavirus maintenance and transmission in reservoir host populations. Curr. Opin. Virol. 2018, 28, 1–6. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Chang, S.-F.; Wang, H.-C.; Hsieh, J.-W.; Lin, M.-C.; Yang, S.-Y. Seroepidemiological Investigation on Hantavirus Prevalence in Rodent Population at International Ports in Taiwan, 2007–2009. Taiwan Epidemiol. Bull. 2012, 28, 148–159. [Google Scholar]
- Hsieh, T.; Wang, J.; Huang, T.; Chen, C. Epidemiological survey of rodent-vector hantavirus infection in Taiwan harbor. Taiwan Epidemiol. Bull. 2008, 24, 51–62. [Google Scholar]
- Investigation of Important Rodent Infectious Diseases in 5 Metropolitan Areas of Taiwan. Taiwan Centers for Disease Control: Taiwan. Available online: https://www.cdc.gov.tw/File/Get/sqrAKrJg_Uq8Ki5B0HtO3g?path=sgK4o5Wbr4mnIuhYzlQsPHSRg7Jqtd6di4k28DXeI6CmXLruu2XUWrlY6EUQgtvr&name=iHFdLwlAwg6YI2WsBXaEIlXqe28ecTJ7hHhZx5xXSy13wOfOmfBJ7nhJWxaZX7TaEme-3hA9_zcm6gEX45EBgsNILCO6FiML1GHf1FVT6UCdK4XUgy-WWSCJ_DqmK8s3vCN1j1l7MAVMRQs563heVdu44bVDoQJocKjd89cNNiNlE7yjsMeQB0hFUSWO5O4g (accessed on 10 July 2020).
- Clement, J.; Maes, P.; Muthusethupathi, M.; Nainan, G.; Van Ranst, M. First evidence of fatal hantavirus nephropathy in India, mimicking leptospirosis. Nephrol. Dial. Transplant. 2006, 21, 826–827. [Google Scholar] [CrossRef][Green Version]
- Lee, T.-Y.; Lin, H.-C.; Tuan, Y.-C.; Hung, M.-N.; You, C.-Y.; Liu, P.-L. Outbreak of Hemorrhagic Fever with Renal Syndrome, Kaohsiung, January–April 2016. Taiwan Epidemiol. Bull. 2016, 32, 438–442. [Google Scholar]
- Anti-Rodent “No Rat Infestation, No Rat Dwelling, and No Rat Feeding” Strategies. Taiwan Centers for Disease Control: Taiwan. Available online: https://www.cdc.gov.tw/Category/ListContent/RNewy5yBj4zj3XIEZep-Lg?uaid=63gxF46w5CHd3dVP5ch2SQ (accessed on 10 July 2020).
- Makary, P.; Kanerva, M.; Ollgren, J.; Virtanen, M.; Vapalahti, O.; Lyytikäinen, O. Disease burden of Puumala virus infections, 1995–2008. Epidemiol. Infect. 2010, 138, 1484–1492. [Google Scholar] [CrossRef]
- Clement, J.; LeDuc, J.W.; Lloyd, G.; Reynes, J.-M.; McElhinney, L.; Van Ranst, M.; Lee, H.-W. Wild rats, laboratory rats, pet rats: Global Seoul hantavirus disease revisited. Viruses 2019, 11, 652. [Google Scholar] [CrossRef] [PubMed]
- Kerins, J.; Koske, S.; Kazmierczak, J.; Austin, C.; Gowdy, K.; Dibernardo, A. Seoul Virus Working GroupCanadian Seoul Virus Investigation Group (Federal) Canadian Seoul Virus Investigation Group (Provincial) Contributors. Outbreak of Seoul virus among rats and rat owners-United States and Canada, 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Krautkrämer, E.; Grouls, S.; Urban, E.; Schnitzler, P.; Zeier, M. No gender-related differences in the severity of nephropathia epidemica, Germany. BMC Infect. Dis. 2013, 13, 457. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Marks, M.A.; Li, W.; Glass, G.E.; Fang, L.-Q.; Ma, J.-Q.; Cao, W.-C. Sex differences in the incidence and case fatality rates from hemorrhagic fever with renal syndrome in China, 2004–2008. Clin. Infect. Dis. 2011, 52, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Oscarsson, K.B.; Brorstad, A.; Baudin, M.; Lindberg, A.; Forssén, A.; Evander, M.; Eriksson, M.; Ahlm, C. Human Puumala hantavirus infection in northern Sweden; increased seroprevalence and association to risk and health factors. BMC Infect. Dis. 2016, 16, 566. [Google Scholar]
- Santos, I.O.; Figueiredo, G.G.D.; Figueiredo, L.T.M.; Azevedo, M.R.A.D.; Novo, N.F.; Vaz, C.A.C. Serologic survey of hantavirus in a rural population from the northern State of Mato Grosso, Brazil. Rev. Soc. Bras. Med. Trop. 2013, 46, 30–33. [Google Scholar] [CrossRef]
- Prist, P.R.; Uriarte, M.; Tambosi, L.R.; Prado, A.; Pardini, R.; Metzger, J.P. Landscape, environmental and social predictors of Hantavirus risk in São Paulo, Brazil. PLoS ONE 2016, 11, e0163459. [Google Scholar] [CrossRef]
- Huang, L.-Y.; Zhou, H.; Yin, W.-W.; Wang, Q.; Sun, H.; Ding, F.; Man, T.-F.; Li, Q.; Feng, Z.-J. The current epidemic situation and surveillance regarding hemorrhagic fever with renal syndrome in China, 2010. Zhonghua Liu Xing Bing Xue Za Zhi 2012, 33, 685–691. [Google Scholar]
- Nikolić, J.; Kuzman, I.; Markotić, A.; Đaković Rode, O.; Curić, I.; Bebek Ivanković, H.; Grgić, S. The occurrence of hemorrhagic fever with renal syndrome in southern parts of Bosnia and Herzegovina. Coll. Antropol. 2009, 33, 37–42. [Google Scholar]
- Donalisio, M.R.; Peterson, A.T. Environmental factors affecting transmission risk for hantaviruses in forested portions of southern Brazil. Acta Trop. 2011, 119, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Gherasim, A.; Hjertqvist, M.; Lundkvist, Å.; Kühlmann-Berenzon, S.; Carlson, J.V.; Stenmark, S.; Widerström, M.; Österlund, A.; Boman, H.; Ahlm, C. Risk factors and potential preventive measures for nephropatia epidemica in Sweden 2011–2012: A case–control study. Infect. Ecol. Epidemiol. 2015, 5, 27698. [Google Scholar] [CrossRef] [PubMed]
- Vapalahti, K.; Virtala, A.-M.; Vaheri, A.; Vapalahti, O. Case-control study on Puumala virus infection: Smoking is a risk factor. Epidemiol. Infect. 2010, 138, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, J.; Oliveira, R.C.D.; Coelho, T.A.; Martins, R.M.B.; Caetano, K.A.A.; Horta, M.A.P.; Levis, S.; Carneiro, M.A.D.S.; Teles, S.A.; Lemos, E.R.S.D. Rodent-borne viruses survey in rural settlers from Central Brazil. Mem. Inst. Oswaldo Cruz 2019, 114. [Google Scholar] [CrossRef] [PubMed]
- Clement, J.; Neild, G.; Hinrichsen, S.L.; Crescente, J.A.; Van Ranst, M. Urban leptospirosis versus urban hantavirus infection in Brazil. Lancet 1999, 354, 2003–2004. [Google Scholar] [CrossRef]
- Mailles, A.; Vaillant, V.; Haeghebaert, S.; Fradet, M.R.; Capek, I.; Zeller, H. Increase of Hantavirus infections in France, 2003. Med. Mal. Infect. 2005, 35, 68–72. [Google Scholar] [CrossRef]
- Gimaque, J.B.L.; Bastos, M.D.S.; Braga, W.S.M.; Oliveira, C.M.C.D.; Castilho, M.D.C.; Figueiredo, R.M.P.D.; Galusso, E.D.S.; Itapirema, E.F.; Figueiredo, L.T.M.D.; Mourão, M.P.G. Serological evidence of hantavirus infection in rural and urban regions in the state of Amazonas, Brazil. Mem. Inst. Oswaldo Cruz 2012, 107, 135–137. [Google Scholar] [CrossRef]
- Klotz, A.; Harouna, A.; Smith, A.F. Tuberculosis in quebec: A review of trends. J. Public Health Res. 2012, 1, 158–164. [Google Scholar] [CrossRef]
- Ryu, S.; Kim, B.I.; Lim, J.-S.; Tan, C.S.; Chun, B.C. One Health Perspectives on Emerging Public Health Threats. J. Prev. Med. Public Health 2017, 50, 411–414. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Years | Summary Cases (%) |
|---|---|
| 2001 | 2 (9.5) |
| 2002 | Not applicable |
| 2003 | Not applicable |
| 2004 | 3 (14.3) |
| 2005 | Not applicable |
| 2006 | 3 (14.3) |
| 2007 | Not applicable |
| 2008 | 1 (4.8) |
| 2009 | Not applicable |
| 2010 | 1 (4.8) |
| 2011 | Not applicable |
| 2012 | 1 (4.8) |
| 2013 | Not applicable |
| 2014 | 2 (9.5) |
| 2015 | 2 (9.5) |
| 2016 | 4 (19.0) |
| 2017 | Not applicable |
| 2018 | 1 (4.8) |
| 2019 | 1 (4.8) |
| Variables | HFRS Cases (n = 21) | p Value | |
|---|---|---|---|
| 2001–2010 | 2011–2019 | ||
| Gender | 1.000 | ||
| Male | 9 | 9 | |
| Female | 1 | 2 | |
| Age | |||
| <20 | 0 | 0 | Not applicable |
| 20–64 | 10 | 10 | 1.000 |
| >=65 | 0 | 1 | 1.000 |
| Season | |||
| Spring | 7 | 3 | 0.086 |
| Summer | 1 | 4 | 0.311 |
| Fall | 0 | 0 | Not applicable |
| Winter | 2 | 4 | 0.635 |
| Area | |||
| Northern | 5 | 5 | 1.000 |
| Central | 1 | 0 | 0.476 |
| Southern | 4 | 6 | 0.670 |
| Eastern | 0 | 0 | Not applicable |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, C.-J.; Li, C.-W.; Cheng, C.-A.; Wu, D.-C.; Wu, W.-C.; Lin, F.-H.; Chou, Y.-C.; Yu, C.-P. Epidemiologic Characteristics of Domestic Patients with Hemorrhagic Fever with Renal Syndrome in Taiwan: A 19-Year Retrospective Study. Int. J. Environ. Res. Public Health 2020, 17, 5291. https://doi.org/10.3390/ijerph17155291
Hsieh C-J, Li C-W, Cheng C-A, Wu D-C, Wu W-C, Lin F-H, Chou Y-C, Yu C-P. Epidemiologic Characteristics of Domestic Patients with Hemorrhagic Fever with Renal Syndrome in Taiwan: A 19-Year Retrospective Study. International Journal of Environmental Research and Public Health. 2020; 17(15):5291. https://doi.org/10.3390/ijerph17155291
Chicago/Turabian StyleHsieh, Chi-Jeng, Chuan-Wang Li, Chun-An Cheng, Ding-Chung Wu, Wen-Chih Wu, Fu-Huang Lin, Yu-Ching Chou, and Chia-Peng Yu. 2020. "Epidemiologic Characteristics of Domestic Patients with Hemorrhagic Fever with Renal Syndrome in Taiwan: A 19-Year Retrospective Study" International Journal of Environmental Research and Public Health 17, no. 15: 5291. https://doi.org/10.3390/ijerph17155291
APA StyleHsieh, C.-J., Li, C.-W., Cheng, C.-A., Wu, D.-C., Wu, W.-C., Lin, F.-H., Chou, Y.-C., & Yu, C.-P. (2020). Epidemiologic Characteristics of Domestic Patients with Hemorrhagic Fever with Renal Syndrome in Taiwan: A 19-Year Retrospective Study. International Journal of Environmental Research and Public Health, 17(15), 5291. https://doi.org/10.3390/ijerph17155291