Development of a Personalized m/eHealth Algorithm for the Resumption of Activities of Daily Life Including Work and Sport after Total and Unicompartmental Knee Arthroplasty: A Multidisciplinary Delphi Study


 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
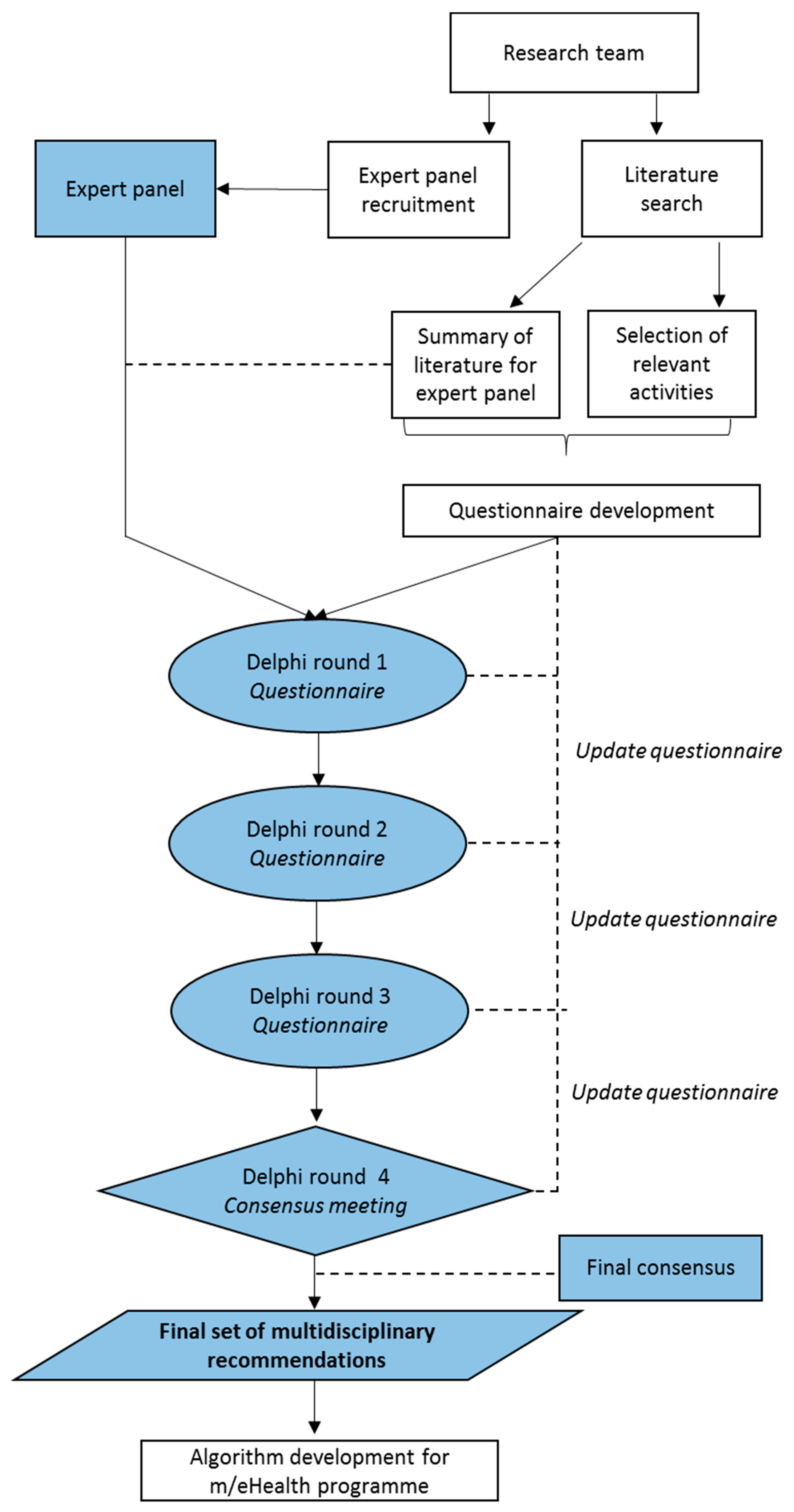
2.1. Study Design
2.2. Recruitment of Expert Panel
2.3. Review of Existing Recovery Recommendations after UKA and TKA
2.4. Selection of Relevant Activities and Development of Delphi Questionnaire
2.5. Delphi Protocol
3. Results
3.1. Relevant Activities
3.2. Consensus
3.3. Recovery Recommendations
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Algorithm Development for Future Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Item | Number of Gradations | Round 1 (%) | Round 2 (%) | Round 3 (%) | Round 4 (%) |
|---|---|---|---|---|---|
| Prolonged sitting | 3 | 62 | 82 | 96 | 100 |
| Prolonged standing | 3 | 68 | 92 | 100 | - |
| Walking on even ground with crutches without crutches | 4 | 69 62 | 96 88 | 100 93 * | - 100 |
| Walking on uneven ground | 4 | 88 | 97 | 89 * | 100 |
| Walking stairs with crutches without crutches | 4 | 49 60 | 70 82 | 92 * 88 * | 100 100 |
| Taking a shower | 2 | 84 | 97 | - | - |
| Taking a bath | 2 | 86 | 99 | - | - |
| Bending | 4 | 64 | 90 | 100 * | - |
| Pushing or pulling | 3 | 66 | 89 | 99 * | - |
| Lifting or carrying | 3 | 70 | 94 | 100 * | - |
| Reaching | 3 | 71 | 94 | 98 | - |
| Driving a car | 2 | 87 | 98 | 98 | - |
| Getting on/off a bike | 4 | 61 | 88 | 99 * | - |
| Riding a bicycle outside | 4 | 68 | 93 | 96 * | 100 |
| Gardening | 3 | 75 | 98 | 100 * | - |
| Household chores | 3 | 76 | 94 | 100 | - |
| Sexual intercourse | 2 | 84 | 99 | - | - |
| Crouching | 4 | 63 | 87 | 100 * | - |
| Kneeling | 4 | 63 | 79 | 92 * | 100 |
| Climbing and/or clambering | 4 | 64 | 85 | 95 | 100 |
| Jogging | 4 | 74 | 89 | 91 * | 100 |
| Sports | 4 | 71 | 95 | 93 * | 100 |
| Using public transportation | 2 | 93 | 99 | 100 | - |
| Working 4 h per day | 4 | 70 | 93 | 97 * | 100 |
| Working 8 h per day | 4 | 70 | 93 | 94 * | 100 |
References
- Volksgezondheid en Zorg. Artrose. 2016. Available online: https://www.volksgezondheidenzorg.info/onderwerp/artrose (accessed on 20 March 2020).
- Nivel Zorgregistraties Eerste Lijn. 2016. Available online: https://www.nivel.nl/sites/default/files/bestanden/Rapport_Reumatische_aandoeningen_nederland.pdf? (accessed on 20 March 2020).
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef]
- Wells, V.M.; Hearn, T.C.; McCaul, K.A.; Anderton, S.M.; Wigg, A.E.; Graves, S.E. Changing incidence of primary total hip arthroplasty and total knee arthroplasty for primary osteoarthritis. J. Arthroplast. 2002, 17, 267–273. [Google Scholar] [CrossRef]
- Heidari, B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Casp. J. Intern. Med. 2011, 2, 205–212. [Google Scholar]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Carr, A.J.; Robertsson, O.; Graves, S.; Price, A.J.; Arden, N.K.; Judge, A.; Beard, D.J. Knee replacement. Lancet 2012, 379, 1331–1340. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone. Joint. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Ackerman, I.N.; Bohensky, M.A.; Zomer, E.; Tacey, M.; Gorelik, A.; Brand, C.A.; de Steiger, R. The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskelet Disord. 2019, 20, 90. [Google Scholar] [CrossRef] [PubMed]
- Otten, R.; van Roermund, P.M.; Picavet, H.S. Trends in the number of knee and hip arthroplasties: Considerably more knee and hip prostheses due to osteoarthritis in 2030. Ned. Tijdschr. Geneeskd. 2010, 154, A1534. [Google Scholar] [PubMed]
- Witjes, S.; van Geenen, R.C.; Koenraadt, K.L.; van der Hart, C.P.; Blankevoort, L.; Kerkhoffs, G.M.; Kuijer, P.P. Expectations of younger patients concerning activities after knee arthroplasty: Are we asking the right questions? Qual. Life. Res. 2017, 26, 403–417. [Google Scholar] [CrossRef]
- Price, A.J.; Alvand, A.; Troelsen, A.; Katz, J.N.; Hooper, G.; Gray, A.; Carr, A.; Beard, D. Knee replacement. Lancet 2018, 392, 1672–1682. [Google Scholar] [CrossRef]
- Mahdi, A.; Svantesson, M.; Wretenberg, P.; Halleberg-Nyman, M. Patients’ experiences of discontentment one year after total knee arthroplasty- a qualitative study. BMC. Musculoskelet. Disord. 2020, 21, 29. [Google Scholar] [CrossRef]
- Nouri, F.; Coole, C.; Baker, P.; Drummond, A. Return to work advice after total hip and knee replacement. Occup. Med. 2020, 70, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef]
- Noble, P.C.; Conditt, M.A.; Cook, K.F.; Mathis, K.B. The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty. Clin. Orthop. Relat. Res. 2006, 452, 35–43. [Google Scholar] [CrossRef]
- Totale Knieprothese. 2014. Available online: https://richtlijnendatabase.nl/richtlijn/totale_knieprothese/totale_knieprothese_-_korte_beschrijving.html (accessed on 20 March 2020).
- Coenen, P.; Hulsegge, G.; Daams, J.G.; van Geenen, R.C.; Kerkhoffs, G.M.; van Tulder, M.W.; Huirne, J.A.; Anema, J.R.; Kuijer, P.P. Integrated care programmes for sport and work participation, performance of physical activities and quality of life among orthopaedic surgery patients: A systematic review with meta-analysis. BMJ Open Sport Exerc. Med. 2020, 6, e000664. [Google Scholar] [CrossRef]
- van der Meij, E.; Anema, J.R.; Leclercq, W.K.G.; Bongers, M.Y.; Consten, E.C.J.; Schraffordt Koops, S.E.; van de Ven, P.M.; Terwee, C.B.; van Dongen, J.M.; Schaafsma, F.G.; et al. Personalised perioperative care by e-health after intermediate-grade abdominal surgery: A multicentre, single-blind, randomised, placebo-controlled trial. Lancet 2018, 392, 51–59. [Google Scholar] [CrossRef]
- Pronk, Y.; Peters, M.; Sheombar, A.; Brinkman, J.M. Effectiveness of a mobile ehealth app in guiding patients in pain control and opiate use after total knee replacement: Randomized controlled trial. JMIR Mhealth Uhealth 2020, 8, e16415. [Google Scholar] [CrossRef]
- Timmers, T.; Janssen, L.; van der Weegen, W.; Das, D.; Marijnissen, W.J.; Hannink, G.; van der Zwaard, B.C.; Plat, A.; Thomassen, B.; Swen, J.W.; et al. The effect of an app for day-to-day postoperative care education on patients with total knee replacement: Randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e15323. [Google Scholar] [CrossRef]
- Bouwsma, E.V.A.; Bosmans, J.E.; van Dongen, J.M.; Brolmann, H.A.M.; Anema, J.R.; Huirne, J.A.F. Cost-effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: Economic evaluation alongside a stepped-wedge cluster-randomised trial. BMJ Open 2018, 8, e017782. [Google Scholar] [PubMed]
- Bouwsma, E.V.A.; Huirne, J.A.F.; van de Ven, P.M.; Vonk Noordegraaf, A.; Schaafsma, F.G.; Schraffordt Koops, S.E.; van Kesteren, P.J.M.; Brolmann, H.A.M.; Anema, J.R. Effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: Cluster controlled trial with randomised stepped-wedge implementation. BMJ Open 2018, 8, e017781. [Google Scholar]
- Jones, J.; Hunter, D. Consensus methods for medical and health services research. BMJ 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Huirne, J.A.; Brolmann, H.A.; van Mechelen, W.; Anema, J.R. Multidisciplinary convalescence recommendations after gynaecological surgery: A modified Delphi method among experts. BJOG 2011, 118, 1557–1567. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, D.C.; van der Meij, E.; Bouwsma, E.V.; Vonk Noordegraaf, A.; van den Heuvel, B.; Meijerink, W.J.; van Baal, W.M.; Huirne, J.A.; Anema, J.R. A modified Delphi method toward multidisciplinary consensus on functional convalescence recommendations after abdominal surgery. Surg. Endosc. 2016, 30, 5583–5595. [Google Scholar] [CrossRef] [PubMed]
- Lisv/UWV. Functional Ability List. In ClaimBeoordelings-en ZorgingsSysteem (CBBS); UWV: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Patient-Reported Outcomes Measurement Information System. 2020. Available online: www.healthmeasures.net (accessed on 24 April 2020).
- Kievit, A.J.; Kuijer, P.P.; Kievit, R.A.; Sierevelt, I.N.; Blankevoort, L.; Frings-Dresen, M.H. A reliable, valid and responsive questionnaire to score the impact of knee complaints on work following total knee arthroplasty: The WORQ. J. Arthroplasty. 2014, 26, 1169–1175.e2. [Google Scholar] [CrossRef]
- Kievit, A.J.; Kuijer, P.; de Haan, L.J.; Koenraadt, K.L.M.; Kerkhoffs, G.; Schafroth, M.U.; van Geenen, R.C.I. Patients return to work sooner after unicompartmental knee arthroplasty than after total knee arthroplasty. Knee. Surg. Sports. Traumatol. Arthrosc. 2019. [Google Scholar] [CrossRef]
- Straat, C.; Kuijer, P.P.; Coenen, P.; Hulsegge, G.; Anema, J.R. Uiteenlopende Adviezen Voor Terugkeer Naar Werk en Dagelijkse Activiteiten na een Knie-Vervanging in Nederlandse Ziekenhuizen, Bedrijfsgeneeskundige Dagen, Arnhem. The Netherlands, 24-05-2019; 24. Available online: https://nvab-online.nl/sites/default/files/bg-dagen/Book%20of%20Abstracts%202019%20def.pdf (accessed on 24 April 2020).
- Witjes, S.; Gouttebarge, V.; Kuijer, P.P.; van Geenen, R.C.; Poolman, R.W.; Kerkhoffs, G.M. Return to sports and physical activity after total and unicondylar knee arthroplasty: A systematic review and meta-analysis. Sports. Med. 2016, 46, 269–292. [Google Scholar] [CrossRef]
- Vogel, L.A.; Carotenuto, G.; Basti, J.J.; Levine, W.N. Physical activity after total joint arthroplasty. Sports Health 2011, 3, 441–450. [Google Scholar] [CrossRef]
- Peter, W.F.; Nelissen, R.G.; Vlieland, T.P. Guideline recommendations for post-acute postoperative physiotherapy in total hip and knee arthroplasty: Are they used in daily clinical practice? Musculoskelet. Care 2014, 12, 125–131. [Google Scholar] [CrossRef]
- Kuster, M.S. Exercise recommendations after total joint replacement: A review of the current literature and proposal of scientifically based guidelines. Sports Med. 2002, 32, 433–445. [Google Scholar] [CrossRef]
- Vonk Noordegraaf, A.; Anema, J.R.; van Mechelen, W.; van Baal, W.M.; van Kesteren, P.J.M.; Brölmann, H.A.; Huirne, J.A. A personalised eHealth programme reduces the duration until return to work after gynaecological surgery: Results of a multicentre randomised trial. Int. J. Obstet. Gynaecol. 2014, 121, 1127–1135. [Google Scholar] [CrossRef]
- Tolk, J.J.; Waarsing, J.E.H.; Janssen, R.P.A.; van Steenbergen, L.N.; Bierma-Zeinstra, S.M.A.; Reijman, M. Development of preoperative prediction models for pain and functional outcome after total knee arthroplasty using the dutch arthroplasty register data. J. Arthroplast. 2020, 35, 690–698.e2. [Google Scholar] [CrossRef]
- Westby, M.D.; Brittain, A.; Backman, C.L. Expert consensus on best practices for post-acute rehabilitation after total hip and knee arthroplasty: A Canada and United States Delphi study. Arthritis Care Res. 2014, 66, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Plenge, U.; Nortje, M.B.; Marais, L.C.; Jordaan, J.D.; Parker, R.; van der Westhuizen, N.; van der Merwe, J.F.; Marais, J.; September, W.V.; Davies, G.L.; et al. Optimising perioperative care for hip and knee arthroplasty in South Africa: A Delphi consensus study. BMC Musculoskelet Disord. 2018, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Westby, M.D.; Marshall, D.A.; Jones, C.A. Development of quality indicators for hip and knee arthroplasty rehabilitation. Osteoarthr. Cartil. 2018, 26, 370–382. [Google Scholar] [CrossRef] [PubMed]
- Bouwsma, E.V.A.; Anema, J.R.; Vonk Noordegraaf, A.; de Vet, H.C.W.; Huirne, J.A.F. Using patient data to optimize an expert-based guideline on convalescence recommendations after gynecological surgery: A prospective cohort study. BMC Surg. 2017, 17, 129. [Google Scholar] [CrossRef]
- Bardgett, M.; Lally, J.; Malviya, A.; Kleim, B.; Deehan, D. Patient-reported factors influencing return to work after joint replacement. Occup. Med. 2016, 66, 215–221. [Google Scholar] [CrossRef]
- Henderson, M.; Glozier, N.; Holland Elliott, K. Long term sickness absence. BMJ 2005, 330, 802–803. [Google Scholar] [CrossRef]



| 1 day | 2 days | 3 days | 4 days | 5 days | 6 days | 1 wk | 2 wks | 3 wks | 4 wks | 5 wks | 6 wks | 7 wks | 8 wks | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UKA (F) | ||||||||||||||
| UKA (A) | ||||||||||||||
| UKA (S) | ||||||||||||||
| TKA (F) | ||||||||||||||
| TKA (A) | ||||||||||||||
| TKA (S) | ||||||||||||||
| Ability score 0: Normal, can walk at least 2 h without walking aids 1: Slightly limited, can walk 1 h (maximum) without walking aids 2: Limited, can walk in and around the house without walking aids 3: Very limited, cannot walk without walking aids | ||||||||||||||
| 1–3 wks | 4 wks | 5 wks | 6 wks | 7 wks | 8 wks | 9 wks | 10 wks | 11 wks | 12 wks | 14 wks | 16 wks | 20 wks | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UKA (F) | |||||||||||||||
| UKA (A) | Not allowed | ||||||||||||||
| UKA (S) | 2–3 km | ||||||||||||||
| TKA (F) | 3–10 km | ||||||||||||||
| TKA (A) | 30–40 km (N) | ||||||||||||||
| TKA (S) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Straat, A.C.; Coenen, P.; Smit, D.J.M.; Hulsegge, G.; Bouwsma, E.V.A.; Huirne, J.A.F.; van Geenen, R.C.; Janssen, R.P.A.; Boymans, T.A.E.J.; Kerkhoffs, G.M.M.J.; et al. Development of a Personalized m/eHealth Algorithm for the Resumption of Activities of Daily Life Including Work and Sport after Total and Unicompartmental Knee Arthroplasty: A Multidisciplinary Delphi Study. Int. J. Environ. Res. Public Health 2020, 17, 4952. https://doi.org/10.3390/ijerph17144952
Straat AC, Coenen P, Smit DJM, Hulsegge G, Bouwsma EVA, Huirne JAF, van Geenen RC, Janssen RPA, Boymans TAEJ, Kerkhoffs GMMJ, et al. Development of a Personalized m/eHealth Algorithm for the Resumption of Activities of Daily Life Including Work and Sport after Total and Unicompartmental Knee Arthroplasty: A Multidisciplinary Delphi Study. International Journal of Environmental Research and Public Health. 2020; 17(14):4952. https://doi.org/10.3390/ijerph17144952
Chicago/Turabian StyleStraat, A. Carlien, Pieter Coenen, Denise J. M. Smit, Gerben Hulsegge, Esther V. A. Bouwsma, Judith A. F. Huirne, Rutger C. van Geenen, Rob P. A. Janssen, Tim A. E. J. Boymans, Gino M. M. J. Kerkhoffs, and et al. 2020. "Development of a Personalized m/eHealth Algorithm for the Resumption of Activities of Daily Life Including Work and Sport after Total and Unicompartmental Knee Arthroplasty: A Multidisciplinary Delphi Study" International Journal of Environmental Research and Public Health 17, no. 14: 4952. https://doi.org/10.3390/ijerph17144952
APA StyleStraat, A. C., Coenen, P., Smit, D. J. M., Hulsegge, G., Bouwsma, E. V. A., Huirne, J. A. F., van Geenen, R. C., Janssen, R. P. A., Boymans, T. A. E. J., Kerkhoffs, G. M. M. J., Anema, J. R., & Kuijer, P. P. F. M. (2020). Development of a Personalized m/eHealth Algorithm for the Resumption of Activities of Daily Life Including Work and Sport after Total and Unicompartmental Knee Arthroplasty: A Multidisciplinary Delphi Study. International Journal of Environmental Research and Public Health, 17(14), 4952. https://doi.org/10.3390/ijerph17144952