Regional Analysis of Associations between Infant and Young Child Feeding Practices and Diarrhoea in Indian Children

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Method
2.1. Data Sources
2.2. Study Setting
2.3. Study Outcome
2.4. Exposure Factors
- EIBF or timely initiation of breastfeeding was defined as the proportion of children within 0–23 months of age who were breastfed within one hour of birth.
- ExcBF was defined as the proportion of infants 0–5 months of age who received breast milk as the only source of nourishment but allowed oral rehydration solution, drops or syrups of vitamins and medicines.
- Predominant breastfeeding (PBF) was defined as the proportion of infants 0–5 months of age who received breast milk as the main source of nourishment but allowed water, water-based drinks, fruit juice, oral rehydration solution, drops or syrups of vitamins and medicines.
- Bottle feeding (BotF) was defined as the proportion of children 0–23 months of age who were fed with a bottle during the previous day.
- Continued breastfeeding (BF) at 1 year was defined as the proportion of children 12–15 months of age who were fed breast milk.
- Continued BF at 2 years was defined as the proportion of children 20–23 months of age who were fed breast milk.
- Children ever breastfed was defined as the proportion of children born in the last 24 months who were ever breastfed.
- Introduction of solid, semi–solid or soft foods (ISSSF) was defined as the proportion of infants 6–8 months of age who received solid, semi–solid or soft foods.
2.5. Potential Confounding Factors
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Characteristics of the Study Population
3.2. Prevalence of Diarrhoea by IYCF Practices among Children Aged 0–23 Months in Regional India
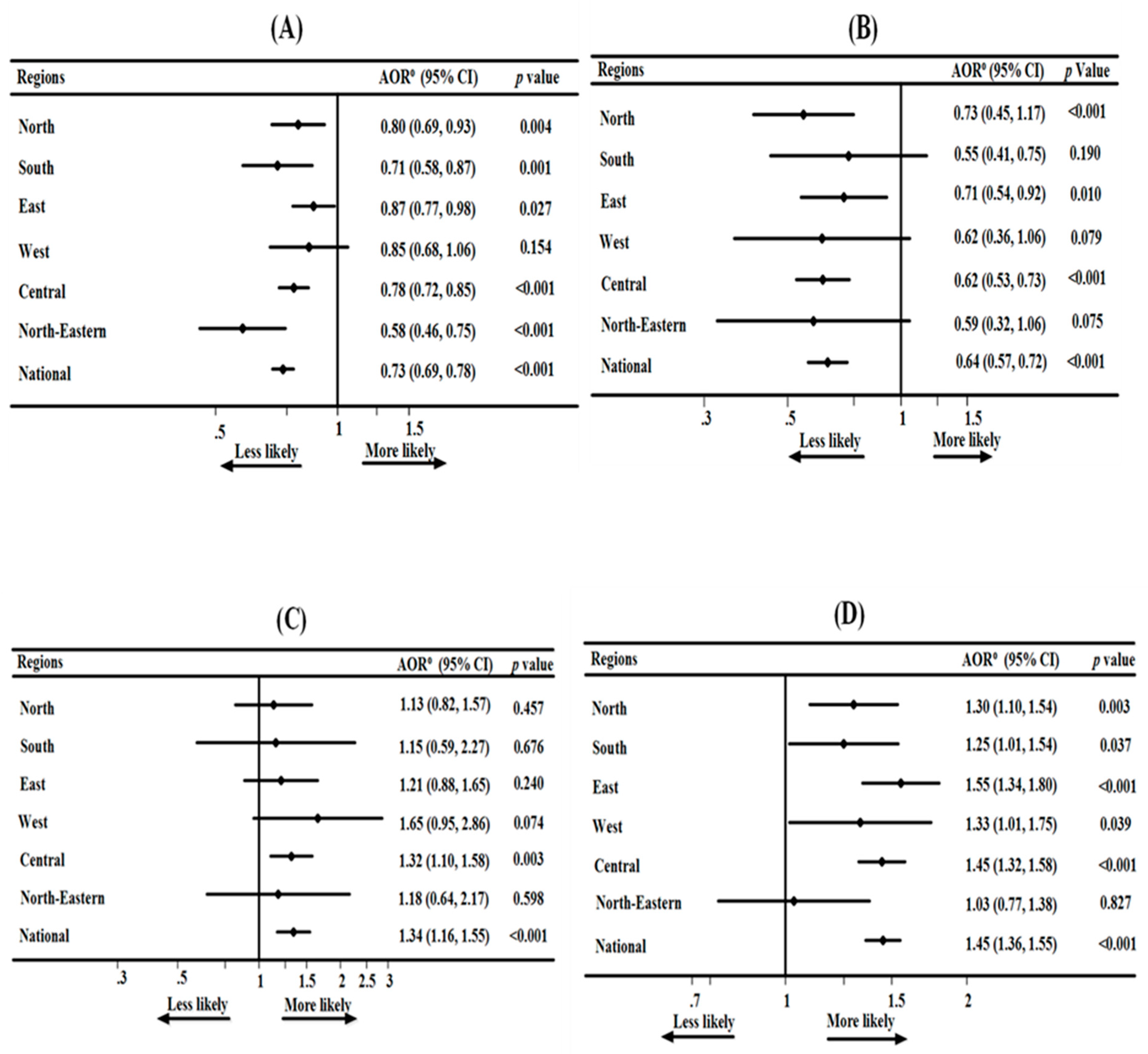
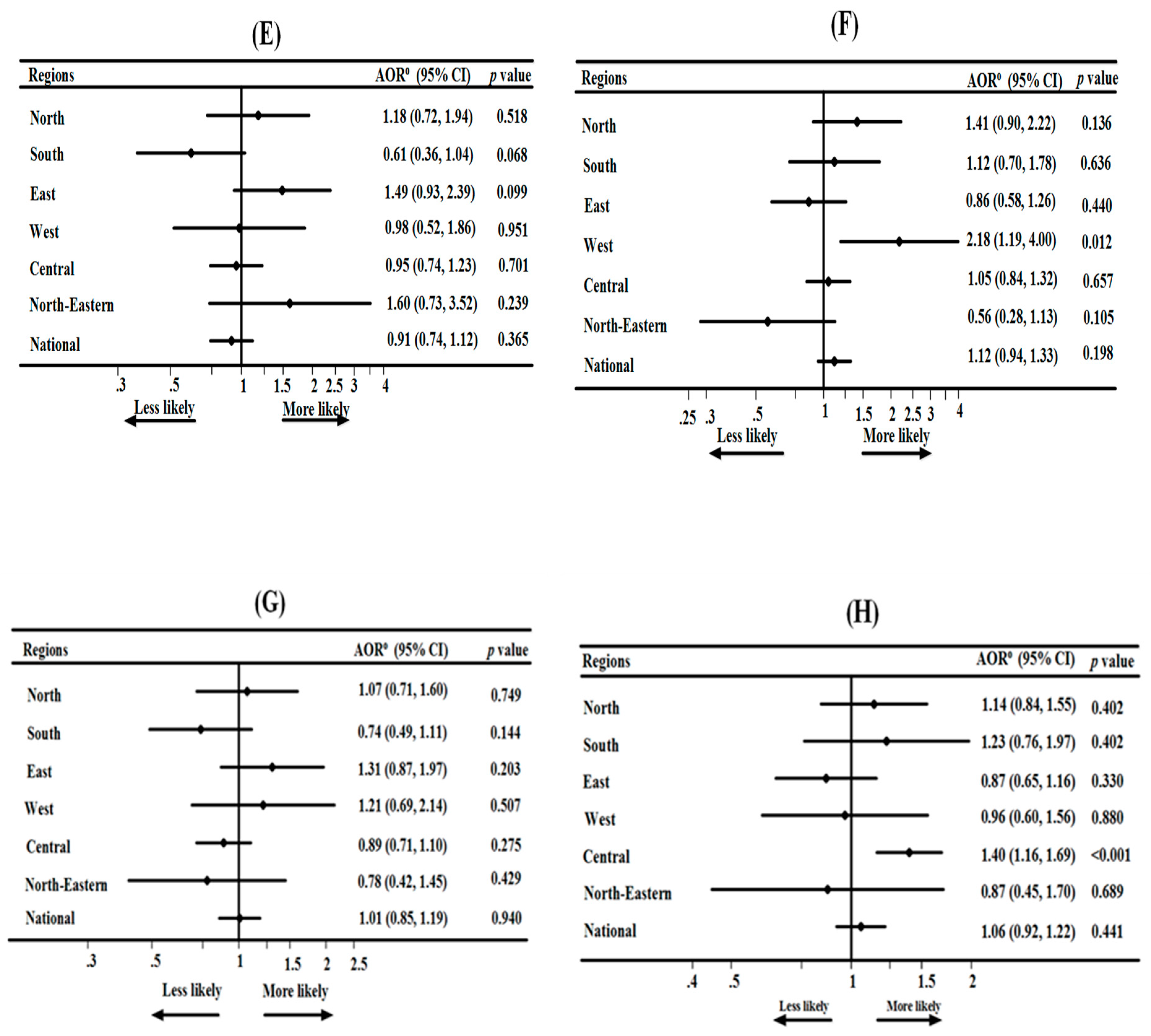
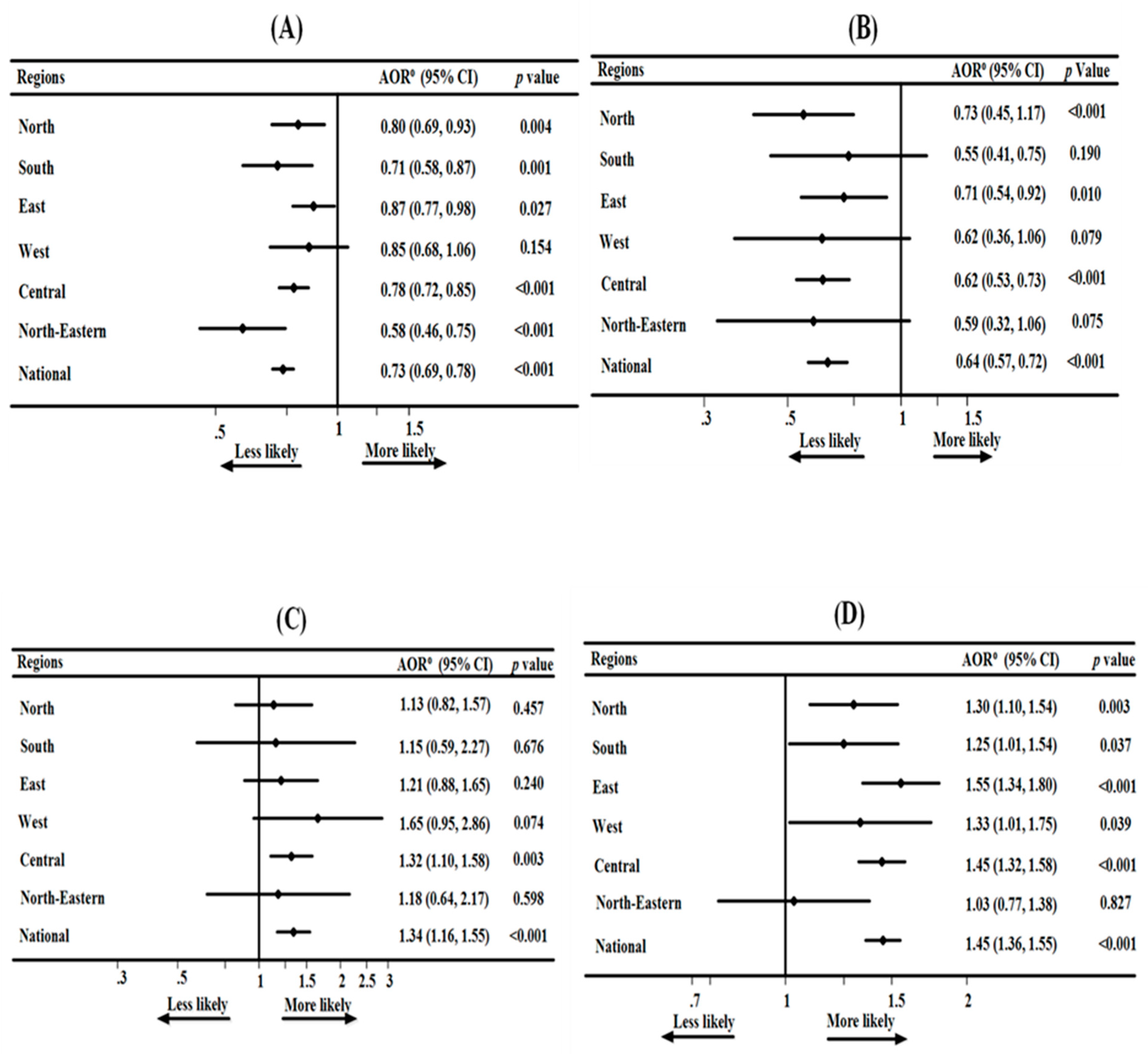
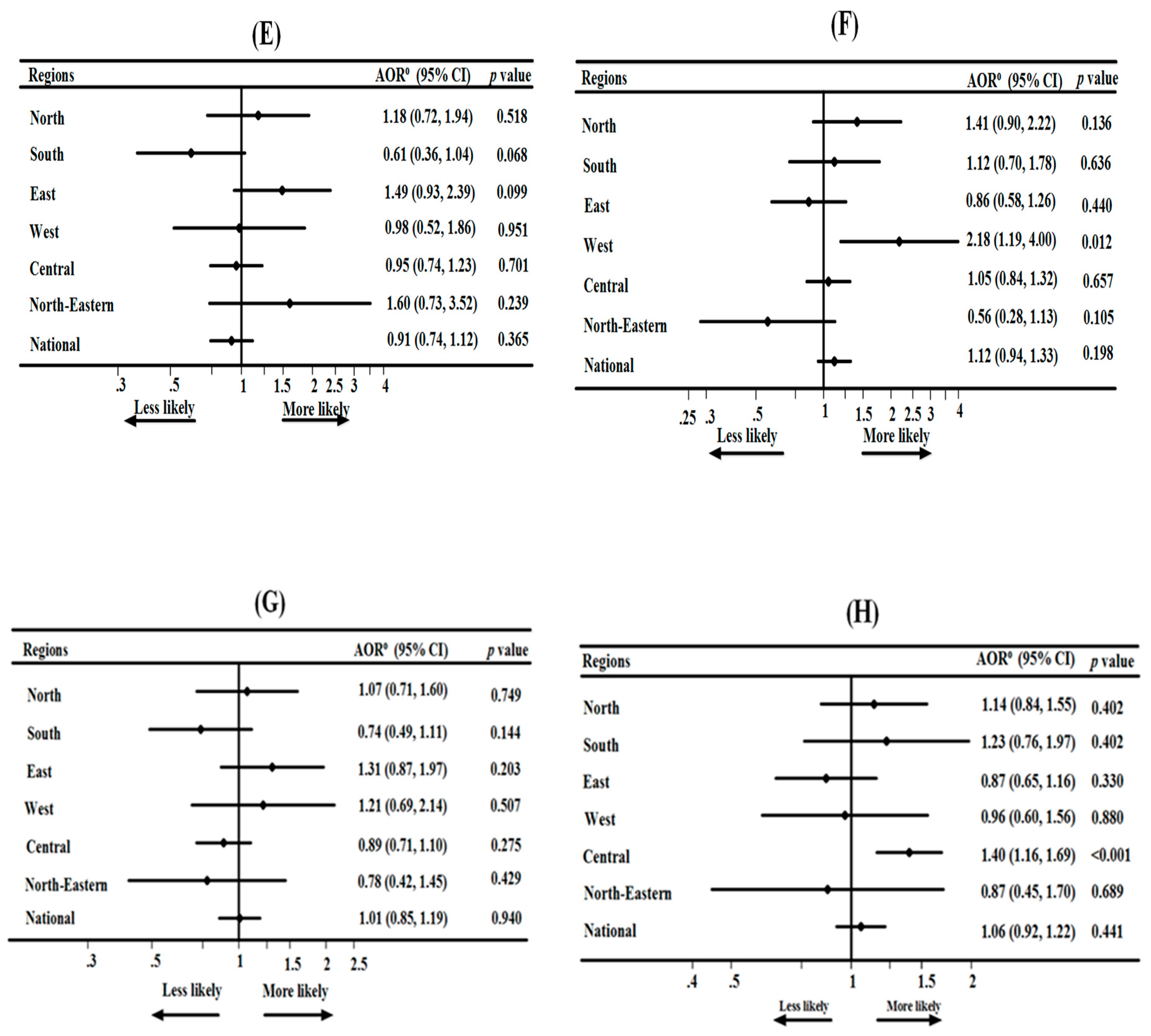
3.3. Association between IYCF Practices and Diarrhoea in Regional India
4. Discussion
Study Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
- Infant and Young Child Feeding (IYCF),
- Early initiation of breastfeeding (EIBF),
- Exclusive breastfeeding (ExcBF),
- Predominant breastfeeding (PBF),
- Bottle feeding (BotF),
- Continued breastfeeding (BF) at one year,
- Introduction of solid, semi-solid or soft foods (ISSSF),
- Low- and Middle-Income Countries (LMICs),
- Water, Sanitation and Hygiene (WASH) trials,
- National Family Health Survey (NFHS-4),
- Ministry of Health and Family Welfare (MoHFW),
- Inner-City Fund (ICF) International Inner-City Fund (ICF) International,
- Primary Sampling Units (PSUs),
- Census Enumeration Blocks (CEBs),
- World Health Organisation (WHO),
- Antenatal clinic (ANC),
- Generalized Linear Latent and Mixed Models (GLLAMM),
- Baby Friendly Hospital Initiative (BFHI),
- World Breastfeeding Trends Initiative (WBTi),
- Stop Diarrhoea Project (SDP).
References
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; The Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Alvis-Guzman, N. GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- Senanayake, P.; O’Connor, E.; Ogbo, F.A. National and rural-urban prevalence and determinants of early initiation of breastfeeding in India. BMC Public Health 2019, 19, 896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogbo, F.A.; Dhami, M.V.; Awosemo, A.O.; Olusanya, B.O.; Olusanya, J.; Osuagwu, U.L.; Agho, K.E. Regional prevalence and determinants of exclusive breastfeeding in India. Int. Breastfeed. J. 2019, 14, 20. [Google Scholar] [CrossRef]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Agho, K.E. Prevalence and factors associated with complementary feeding practices among children aged 6–23 months in India: A regional analysis. BMC Public Health 2019, 19, 1034. [Google Scholar] [CrossRef] [Green Version]
- Freeman, M.C.; Clasen, T. Assessing the impact of a school-based safe water intervention on household adoption of point-of-use water treatment practices in southern India. Am. J. Trop. Med. Hyg. 2011, 84, 370–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of India. National Health Mission 2016. Available online: http://vikaspedia.in/health/nrhm/national-health-mission (accessed on 11 March 2019).
- Government of India. Childhood Diarrhoea and its management 2019. Available online: http://vikaspedia.in/health/child-health/diarrhoea (accessed on 22 March 2019).
- Government of India. National Nutrition Strategy 2017: NITI Aayog. 2017. Available online: http://vikaspedia.in/health/nrhm/national-health-policies/national-nutrition-strategy-2017 (accessed on 12 April 2019).
- Stanly, A.; Sathiyasekaran, B.; Palani, G. A population based study of acute diarrhoea among children under 5 years in a rural community in South India. SRJM 2009, 1, 1–7. [Google Scholar]
- Ahmed, S.F.; Farheen, A.; Muzaffar, A.; Mattoo, G.M. Prevalence of Diarrhoeal Disease, its Seasonal and Age Variation in under- fives in Kashmir, India. Int. J. Health Sci. 2008, 2, 126–133. [Google Scholar]
- Avachat, S.S.; Phalke, V.D.; Phalke, D.B.; Aarif, S.M.M.; Kalakoti, P. A cross-sectional study of socio-demographic determinants of recurrent diarrhoea among children under five of rural area of Western Maharashtra, India. Australas. Med. J. 2011, 4, 72–75. [Google Scholar] [CrossRef]
- Kumar, S.; Vollmer, S. Does access to improved sanitation reduce childhood diarrhea in rural India? Health Econ. 2013, 22, 410–427. [Google Scholar] [CrossRef] [Green Version]
- Nandi, A.; Megiddo, I.; Ashok, A.; Verma, A.; Laxminarayan, R. Reduced burden of childhood diarrheal diseases through increased access to water and sanitation in India: A modeling analysis. Soc. Sci. Med. 2017, 180, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Million Death Study Collaborators. Causes of neonatal and child mortality in India: A nationally representative mortality survey. Lancet 2010, 376, 1853–1860. [Google Scholar] [CrossRef] [Green Version]
- Lakshminarayanan, S.; Jayalakshmy, R. Diarrheal diseases among children in India: Current scenario and future perspectives. J. Nat. Sci. Biol. Med. 2015, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, N.; Chakraborty, A.; Lahiri, A.; Biswas, K. Exclusive breast feeding reduces diarrhoeal episodes among children: Results from a cross-sectional study among the mothers of under-five children in Kolkata. Int. J. Community Med. Public Health 2019, 6, 733–737. [Google Scholar] [CrossRef] [Green Version]
- Panda, S.; Deb, A.K.; Chawla-Sarkar, M.; Ramamurthy, T.; Ganguly, S.; Pradhan, P.; Dhere, R. Factors associated with diarrhoea in young children and incidence of symptomatic rotavirus infection in rural West Bengal, India. Epidemiol. Infect. 2014, 142, 1848–1858. [Google Scholar] [CrossRef] [PubMed]
- Joseph, N.; Naik, V.A.; Mahantshetti, N.S.; Unnikrishnan, B.; Mallapur, M.; Kotian, S.M. Factors associated with morbidities among infants in three sub centre areas of belgaum district of South India: A longitudinal study. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2013, 38, 168. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, C.; Do, Y.K. Socio-economic disparities in health system responsiveness in India. Health Policy Plan 2012, 28, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neogi, D. Disparity in Socio-Economic Development and Its Implications on Communal Conflicts: A Study on India’s North-Eastern Region. Int. J. Humanit. Soc. Sci. 2010, 4, 1069–1076. [Google Scholar]
- Baru, R.; Acharya, A.; Acharya, S.; Kumar, A.S.; Nagaraj, K. Inequities in access to health services in India: Caste, class and region. Econ. Political Wkly. 2010, 45, 49–58. [Google Scholar]
- Jat, T.R.; Ng, N.; San Sebastian, M. Factors affecting the use of maternal health services in Madhya Pradesh state of India: A multilevel analysis. Int. J. Equity Health 2011, 10, 59. [Google Scholar] [CrossRef] [Green Version]
- International Institute for Population Sciences (IIPS); ICF. National Family Health Survey (NFHS-4)-National Report, Mumbai, India IIPS. 2017. Available online: http://rchiips.org/NFHS/NFHS-4Reports/India.pdf (accessed on 2 May 2019).
- Ghatowar, P.S. The North-Eastern Council (Amendment) Bill, 2013-A Bill further to amend the North-Eastern Council Act, 1971: Bill No. XVII of 2013. New Delhi, India, 2013. Available online: http://164.100.24.167/newcommittee/press_release/Bill/Committee%20on%20Home%20Affairs/Norheast-E.pdf (accessed on 10 May 2019).
- Government of India-Ministry of Home Affairs. Zonal Council Online: Government of India. 2018. Available online: https://mha.gov.in/zonal-council (accessed on 21 May 2019).
- Government of India, Ministry of Home Affairs. Maps of newly formed Union Territories of Jammu Kashmir and Ladakh, with the map of India; Government of India: Delhi, India, 2019. Available online: https://pib.gov.in/PressReleasePage.aspx?PRID=1590112 (accessed on 26 May 2019).
- Ogbo, F.A.; Agho, K.; Ogeleka, P.; Woolfenden, S.; Page, A.; Eastwood, J. Infant feeding practices and diarrhoea in sub-Saharan African countries with high diarrhoea mortality. PLoS ONE 2017, 12, e0171792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogbo, F.A.; Nguyen, H.; Naz, S.; Agho, K.E.; Page, A. The association between infant and young child feeding practices and diarrhoea in Tanzanian children. Trop. Med. Health 2018, 46, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ogbo, F.A.; Page, A.; Idoko, J.; Claudio, F.; Agho, K.E. Diarrhoea and suboptimal feeding practices in Nigeria: Evidence from the national household surveys. Paediatr. Perinat. Epidemiol. 2016, 30, 346–355. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices—Part 1—Definitions. 2008. Available online: http://apps.who.int/iris/bitstream/handle/10665/43895/9789241596664_eng.pdf?sequence=1&isAllowed=y (accessed on 2 June 2019).
- Biswas, A.; Mandal, A.K. A study on association between breastfeeding and its protective role against diarrhoea in under five children in a rural block of West Bengal, India. Int. J. Community Med. Public Health 2016, 3, 2499–2503. [Google Scholar] [CrossRef] [Green Version]
- Gabida, M. Effects of Mother-Based Promotion of Exclusive Breastfeeding on Duration and Severity of Diarrhoea and Pneumonia: A Cluster Randomized Controlled Trial; University of Zimbabwe: Midlands Province, Zimbabwe, 2013. [Google Scholar]
- Lamberti, L.M.; Walker, C.L.F.; Noiman, A.; Victora, C.; Black, R.E. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health 2011, 11, S15. [Google Scholar] [CrossRef] [Green Version]
- Mitra, K.; Nandi, C.; Banerjee, S. A Study on Infant and Young Child Feeding Practice among the Slum Dwellers of Barddhaman Municipal Area, West Bengal. IOSR J. Dent. Med. Sci. 2017, 16, 19–22. [Google Scholar] [CrossRef]
- Rana, B.M.; Chandwani, H.; Sonaliya, K.; Prajapati, A. A descriptive study to assess factors affecting core indicators of infant and young child feeding practices in urban area of Gujarat State, India. Int. J. Community Med. Public Health 2017, 3, 1101–1106. [Google Scholar] [CrossRef]
- Rao, S.; Swathi, P.; Unnikrishnan, B.; Hegde, A. Study of complementary feeding practices among mothers of children aged six months to two years-A study from coastal south India. Australas. Med J. 2011, 4, 252. [Google Scholar] [CrossRef]
- UNICEF; WHO. Progress on household drinking water, sanitation and hygiene 2000–2017; Special focus on inequalities; United Nations Children’s Fund (UNICEF) and World Health Organization: New York, NY, USA, 2019; Available online: https://www.who.int/water_sanitation_health/publications/jmp-report-2019/en/ (accessed on 11 January 2020).
- Dibley, M.J.; Titaley, C.R.; d’Este, C.; Agho, K. Iron and folic acid supplements in pregnancy improve child survival in Indonesia. Am. J. Clin. Nutr. 2012, 95, 220–230. [Google Scholar] [CrossRef]
- Verduci, E.; Banderali, G.; Barberi, S.; Radaelli, G.; Lops, A.; Betti, F.; Giovannini, M. Epigenetic effects of human breast milk. Nutrients 2014, 6, 1711–1724. [Google Scholar] [CrossRef]
- Meshram, I.I.; Laxmaiah, A.; Venkaiah, K.; Brahmam, G. Impact of feeding and breastfeeding practices on the nutritional status of infants in a district of Andhra Pradesh, India. Natl. Med. J. India 2012, 25, 201. [Google Scholar] [PubMed]
- Srivastava, N.M.; Awasthi, S. Breastfeeding practices for newborns among urban poor in Lucknow, northern India: A prospective follow-up study. Clin. Epidemiol. Glob. Health 2014, 2, 66–74. [Google Scholar] [CrossRef]
- Vijayalakshmi, S.; Patil, R.; Datta, S.; Narayan, K.; Stephen, F. Feeding Practices and Morbidity Pattern of Infants in a Rural Area of Puducherry-A Follow Up Study. J. Community Med. Health Educ. 2014, 4, 304. [Google Scholar] [CrossRef] [Green Version]
- Acharya, D.; Singh, J.K.; Adhikari, M.; Gautam, S.; Pandey, P.; Dayal, V. Association of water handling and child feeding practice with childhood diarrhoea in rural community of Southern Nepal. J. Infect. Public Health 2018, 11, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Arifeen, S.; Black, R.E.; Antelman, G.; Baqui, A.; Caulfield, L.; Becker, S. Exclusive breastfeeding reduces acute respiratory infection and diarrhea deaths among infants in Dhaka slums. Pediatrics 2001, 108, e67. [Google Scholar] [CrossRef] [Green Version]
- Mihrshahi, S.; Oddy, W.H.; Peat, J.K.; Kabir, I. Association between infant feeding patterns and diarrhoeal and respiratory illness: A cohort study in Chittagong, Bangladesh. Int. Breastfeed. J. 2008, 3, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dairo, M.D.; Ibrahim, T.F.; Salawu, A.T. Prevalence and determinants of diarrhoea among infants in selected primary health centres in Kaduna north local government area, Nigeria. Pan. Afr. Med. J. 2017, 28, 151. [Google Scholar] [CrossRef] [PubMed]
- Hajeebhoy, N.; Nguyen, P.H.; Mannava, P.; Nguyen, T.T.; Mai, L.T. Suboptimal breastfeeding practices are associated with infant illness in Vietnam. Int. Breastfeed. J. 2014, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Sahu, M. Exclusive breastfeeding-mothers absolute affection. Acta Sci. Med. Sci. 2018, 2, 1–2. [Google Scholar]
- WHO. International Code of Marketing of Breast-milk Substitutes; World Health Organization: Geneva, Switzerland, 1981; Available online: https://www.who.int/nutrition/publications/code_english.pdf (accessed on 11 August 2019).
- WHO; UNICEF. Baby-friendly Hospital Initiative: WHO, UNICEF. 1990. Available online: https://www.who.int/nutrition/bfhi/en/ (accessed on 22 August 2019).
- Access to Nutrition Index. Access to Nutrition Index, India, BMS report: BMS 2016. 2016. Available online: https://www.accesstonutrition.org/sites/in16.atnindex.org/files/resources/india_bms_chapter.pdf (accessed on 29 August 2019).
- WHO. Implementation Guidance: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services—the Revised Baby-Friendly Hospital Initiative; Contract: No.: CC BY-NC-SA 3.0 IGO; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Uthkarsh, P.S.; Krishnappa, L.; Singh, S.; Murthy, N.S.; Puttajois, S.S.; Pruthvish, S. Assessment of The Status of Baby Friendly Hospital Initiative in Two Selected Tertiary Level Hospitals in South India. J. Clin. Res. Gov. 2014, 3, 16–20. [Google Scholar]
- Swetha, R.; Ravikumar, J.; Nageswara Rao, R. Study of breastfeeding practices in coastal region of South India: A cross sectional study. Int. J. Contemp. Pediatr. 2014, 1, 74–78. [Google Scholar]
- Korade, R.S.; Dhande, L.A.; Bendhari, M.L.; Patel, A.B. Can Re-training in Baby Friendly Hospital Initiative (BFHI) Improve Breast Feeding Indicators? Indian J. Pediatr. 2016, 83, 475–476. [Google Scholar] [CrossRef] [PubMed]
- Breastfeeding Promotion Network of India (BPNI), International Baby Food Action Network (IBFAN) Asia. Arrested Development. All Is Not Well with Our Children’s Health—Assessment of India’s Policy and Programmes on Infant and Young Child Feeding; World Breastfeeding Trends Initiative (WBTi): Delhi, India, 2015; Available online: https://www.bpni.org/report/WBTi-India-Report-2015.pdf (accessed on 5 September 2019).
- Breastfeeding Promotion Network of India (BPNI), International Baby Food Action Network (IBFAN) Asia. Arrested Development: 5th Report of Assessment of India’s Policy and Programmes on Infant and Young Child Feeding; World Breastfeeding Trends Initiative (WBTi): Delhi, India, 2018; Available online: https://www.worldbreastfeedingtrends.org/uploads/country-data/country-report/WBTi-India-Report-2018.pdf (accessed on 6 September 2019).
- Bahl, R.; Frost, C.; Kirkwood, B.R.; Edmond, K.; Martines, J.; Bhandari, N.; Arthur, P. Infant feeding patterns and risks of death and hospitalization in the first half of infancy: Multicentre cohort study. Bull World Health Organ 2005, 83, 418–426. [Google Scholar] [PubMed]
- Victora, C.G.; Barros, F.C.; Horta, B.L.; Lima, R.C. Breastfeeding and school achievement in Brazilian adolescents. Acta Paediatr. 2005, 94, 1656–1660. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Horta, B.L.; De Mola, C.L.; Quevedo, L.; Pinheiro, R.T.; Gigante, D.P.; Barros, F.C. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: A prospective birth cohort study from Brazil. Lancet Glob. Health 2015, 3, e199–e205. [Google Scholar] [CrossRef] [Green Version]
- WHO. Infant and Young Child Feeding-Model Chapter for Textbooks for Medical Students and Allied Health Professionals; WHO: Geneva, Switzerland, 2009; Available online: https://www.who.int/nutrition/publications/infantfeeding/9789241597494.pdf (accessed on 2 October 2019).
- Government of India. Swachh Bharat Abhiyan. 2014. Available online: https://www.pmindia.gov.in/en/major_initiatives/swachh-bharat-abhiyan/ (accessed on 15 October 2019).
- Shamim, S.; Jamalvi, S.W.; Naz, F. Determinants of bottle use amongst economically disadvantaged mothers. J. Ayub Med. Coll. Abbottabad 2006, 18, 1–4. [Google Scholar]
- Hengstermann, S.; Mantaring, J.B.V.; Sobel, H.L.; Borja, V.E.; Basilio, J.; Iellamo, A.D.; Nyunt-U, S. Formula feeding is associated with increased hospital admissions due to infections among infants younger than 6 months in Manila, Philippines. J. Hum. Lact. 2010, 26, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Satija, M.; Sharma, S.; Chaudhary, A.; Kaushal, P.; Girdhar, S. Infant and young child feeding practices in a rural area of North India. Asian J. Med. Sci. 2015, 6, 60–65. [Google Scholar] [CrossRef] [Green Version]
- John, B.; Devgan, A.; Mitra, B. Prevalence of rotavirus infection in children below two years presenting with diarrhea. Med. J. Armed Forces India 2014, 70, 116–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenske, N.; Burns, J.; Hothorn, T.; Rehfuess, E.A. Understanding child stunting in India: A comprehensive analysis of socio-economic, nutritional and environmental determinants using additive quantile regression. PLoS ONE 2013, 8, e78692. [Google Scholar] [CrossRef]
- Sheth, M.; Dwivedi, R. Complementary foods associated diarrhea. Indian J. Pediatr. 2006, 73, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Ahmed, T.; Faruque, A.S.G.; Rahman, S.; Das, S.K.; Ahmed, D.; Cravioto, A. Microbiological quality of complementary foods and its association with diarrhoeal morbidity and nutritional status of Bangladeshi children. Eur. J. Clin. Nutr. 2012, 66, 1242–1246. [Google Scholar] [CrossRef] [PubMed]
- Kimanya, M.E.; De Meulenaer, B.; Roberfroid, D.; Lachat, C.; Kolsteren, P. Fumonisin exposure through maize in complementary foods is inversely associated with linear growth of infants in Tanzania. Mol. Nutr. Food Res. 2010, 54, 1659–1667. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.P.; Iannotti, L.; Dewey, K.G.; Michaelsen, K.F.; Onyango, A.W. Contextualising complementary feeding in a broader framework for stunting prevention. Matern. Child. Nutr. 2013, 9, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Kerr, R.B.; Dakishoni, L.; Shumba, L.; Msachi, R.; Chirwa, M. “We grandmothers know plenty”: Breastfeeding, complementary feeding and the multifaceted role of grandmothers in Malawi. Soc. Sci. Med. 2008, 66, 1095–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anigo, K.; Ameh, D.; Ibrahim, S.; Danbauchi, S. Nutrient composition of commonly used complementary foods in North Western Nigeria. Afr. J. Biotechnol. 2009, 8, 4211–4216. [Google Scholar]
- Gibson, R.; Ferguson, E.; Lehrfeld, J. Complementary foods for infant feeding in developing countries: Their nutrient adequacy and improvement. Eur. J. Clin. Nutr. 1998, 52, 764. [Google Scholar] [CrossRef] [Green Version]
- Save the Children India. Stop Diarrhoea Project Demonstrates 62% Reduction in Point Prevalence of Diarrhoea 2019. Available online: https://www.savethechildren.in/news/stop-diarrhoea-project-demonstrates-62-reduction (accessed on 11 November 2019).

{kind=link}
{kind=link}
| North | South | East | West | Central | North-East | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N a | Prevalence b (95% CI) | N | Prevalence (95% CI) | N | Prevalence (95% CI) | N | Prevalence (95% CI) | N | Prevalence (95% CI) | N | Prevalence (95% CI) | |
| Early initiation of breastfeeding | ||||||||||||
| No | 939 | 8.3 (7.7, 9.1) | 860 | 5.2 (4.6, 5.9) | 1770 | 7.5 (7.1, 8.1) | 749 | 6.5 (5.7, 7.4) | 3672 | 14.7 (14.2, 15.3) | 82 | 2.5 (2.1, 3.1) |
| Yes | 393 | 3.5 (3.1, 3.9) | 699 | 4.2 (3.7, 4.7) | 1163 | 4.9 (4.5, 5.4) | 797 | 6.9 (6.0, 8.0) | 1298 | 5.2 (4.9, 5.5) | 85 | 2.6 (2.3, 3.0) |
| Exclusive breastfeeding | ||||||||||||
| No | 169 | 6.1 (5.1, 7.3) | 114 | 3.1 (2.2, 4.2) | 260 | 5.0 (4.2, 5.9) | 126 | 4.9 (3.4, 6.9) | 638 | 10.3 (9.4, 11.1) | 13 | 1.7 (1.2, 2.3) |
| Yes | 132 | 4.8 (3.9, 5.8) | 120 | 3.2 (2.4, 4.4) | 241 | 4.6 (3.9, 5.4) | 118 | 4.6 (3.5, 6.0) | 412 | 6.6 (6.0, 7.4) | 13 | 1.6 (1.0, 2.4) |
| Predominant breastfeeding | ||||||||||||
| No | 226 | 8.2 (7.1, 9.5) | 198 | 5.4 (4.3, 6.8) | 404 | 7.7 (6.8, 8.8) | 178 | 6.9 (5.3, 8.8) | 742 | 11.9 (11.1, 12.9) | 22 | 2.7 (2.0, 3.7) |
| Yes | 75 | 2.7 (2.1, 3.5) | 36 | 0.9 (0.5, 1.6) | 98 | 1.8 (1.4, 2.4) | 67 | 2.6 (1.6, 4.1) | 309 | 5.0 (4.4, 5.6) | 4 | 0.5 (0.3, 0.8) |
| Bottle feeding | ||||||||||||
| No | 91 | 8.8 (8.2, 9.5) | 1133 | 6.8 (6.2, 7.2) | 2339 | 10.0 (9.4, 10.6) | 1260 | 10.9 (9.9, 12.0) | 3584 | 14.4 (13.9, 14.9) | 137 | 4.2 (3.7, 4.8) |
| Yes | 342 | 3.1 (2.6, 3.5) | 426 | 2.5 (2.2, 3.0) | 595 | 2.5 (2.2, 2.8) | 287 | 2.5 (1.9, 3.2) | 1385 | 5.6 (5.2, 5.9) | 29 | 0.9 (0.7, 1.1) |
| Continued breastfeeding at one year | ||||||||||||
| No | 35 | 1.8 (1.2, 2.8) | 80 | 2.7 (1.8, 5.3) | 43 | 1.1 (0.7, 1.5) | 47 | 2.3 (1.2, 4.4) | 121 | 3.0 (2.4, 3.6) | 2 | 0.3 (0.1, 0.5) |
| Yes | 212 | 11.1 (9.8, 12.9) | 195 | 6.7 (5.3, 8.4) | 526 | 12.8 (11.5, 14.3) | 258 | 13.0 (10.7, 15.7) | 733 | 18.0 (16.7, 19.3) | 32 | 5.2 (4.1, 6.7) |
| Continued breastfeeding at two years | ||||||||||||
| No | 38 | 2.3 (1.6, 3.3) | 106 | 4.0 (2.9, 5.3) | 72 | 1.9 (1.3, 2.6) | 38 | 2.1 (1.3, 3.4) | 159 | 4.5 (3.8, 5.2) | 7 | 1.3 (0.8, 3.0) |
| Yes | 127 | 7.8 (6.4, 9.4) | 151 | 5.8 (4.3, 7.4) | 349 | 9.2 (8.0, 10.6) | 144 | 7.9 (5.9, 10.4) | 471 | 13.2 (12.1, 14.5) | 21 | 4.1 (3.0, 5.5) |
| Children ever breastfed | ||||||||||||
| No | 36 | 0.3 (0.2, 0.4) | 76 | 0.5 (0.3, 0.7) | 58 | 0.2 (0.2, 0.4) | 31 | 0.3 (0.1, 0.4) | 125 | 0.5 (0.4, 0.6) | 9 | 0.3 (0.1, 0.6) |
| Yes | 1297 | 11.5 (10.8, 12.3) | 1483 | 9.0 (8.2, 9.8) | 2876 | 12.3 (11.7, 13.0) | 1516 | 13.2 (11.9, 14.5) | 4845 | 19.5 (18.9, 20.1) | 157 | 4.8 (4.3, 5.5) |
| Introduction of solid, semi-solid or soft foods | ||||||||||||
| No | 137 | 8.2 (6.9, 9.7) | 93 | 4.2 (3.1, 5.7) | 281 | 8.5 (7.2, 9.8) | 171 | 10.5 (8.1, 13.6) | 451 | 12.5 (11.3, 13.8) | 11 | 2.9 (1.9, 4.6) |
| Yes | 103 | 6.1 (5.1, 7.5) | 170 | 7.7 (5.5, 10.6) | 183 | 5.5 (4.5, 6.6) | 151 | 9.3 (6.6, 12.9) | 355 | 9.9 (8.8, 11.0) | 11 | 3.1 (2.0, 4.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhami, M.V.; Ogbo, F.A.; Diallo, T.M.O.; Agho, K.E.; on behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). Regional Analysis of Associations between Infant and Young Child Feeding Practices and Diarrhoea in Indian Children. Int. J. Environ. Res. Public Health 2020, 17, 4740. https://doi.org/10.3390/ijerph17134740
Dhami MV, Ogbo FA, Diallo TMO, Agho KE, on behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). Regional Analysis of Associations between Infant and Young Child Feeding Practices and Diarrhoea in Indian Children. International Journal of Environmental Research and Public Health. 2020; 17(13):4740. https://doi.org/10.3390/ijerph17134740
Chicago/Turabian StyleDhami, Mansi Vijaybhai, Felix Akpojene Ogbo, Thierno M.O. Diallo, Kingsley E. Agho, and on behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). 2020. "Regional Analysis of Associations between Infant and Young Child Feeding Practices and Diarrhoea in Indian Children" International Journal of Environmental Research and Public Health 17, no. 13: 4740. https://doi.org/10.3390/ijerph17134740
APA StyleDhami, M. V., Ogbo, F. A., Diallo, T. M. O., Agho, K. E., & on behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). (2020). Regional Analysis of Associations between Infant and Young Child Feeding Practices and Diarrhoea in Indian Children. International Journal of Environmental Research and Public Health, 17(13), 4740. https://doi.org/10.3390/ijerph17134740