Mobilizing for Community Benefits to Assess Health and Promote Environmental Justice near the Gordie Howe International Bridge

 ,
, 
Abstract
1. Introduction
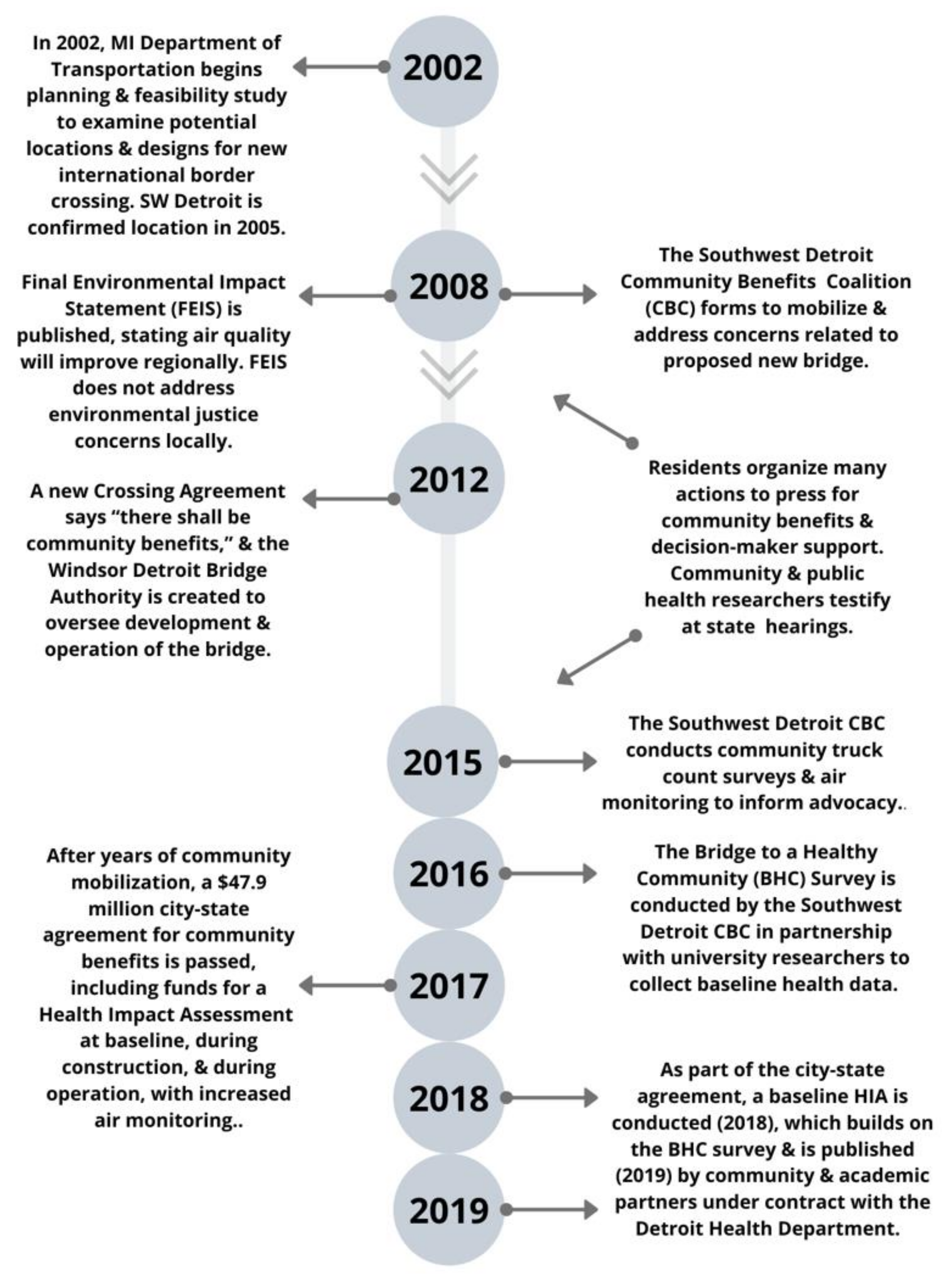
2. Background and Context
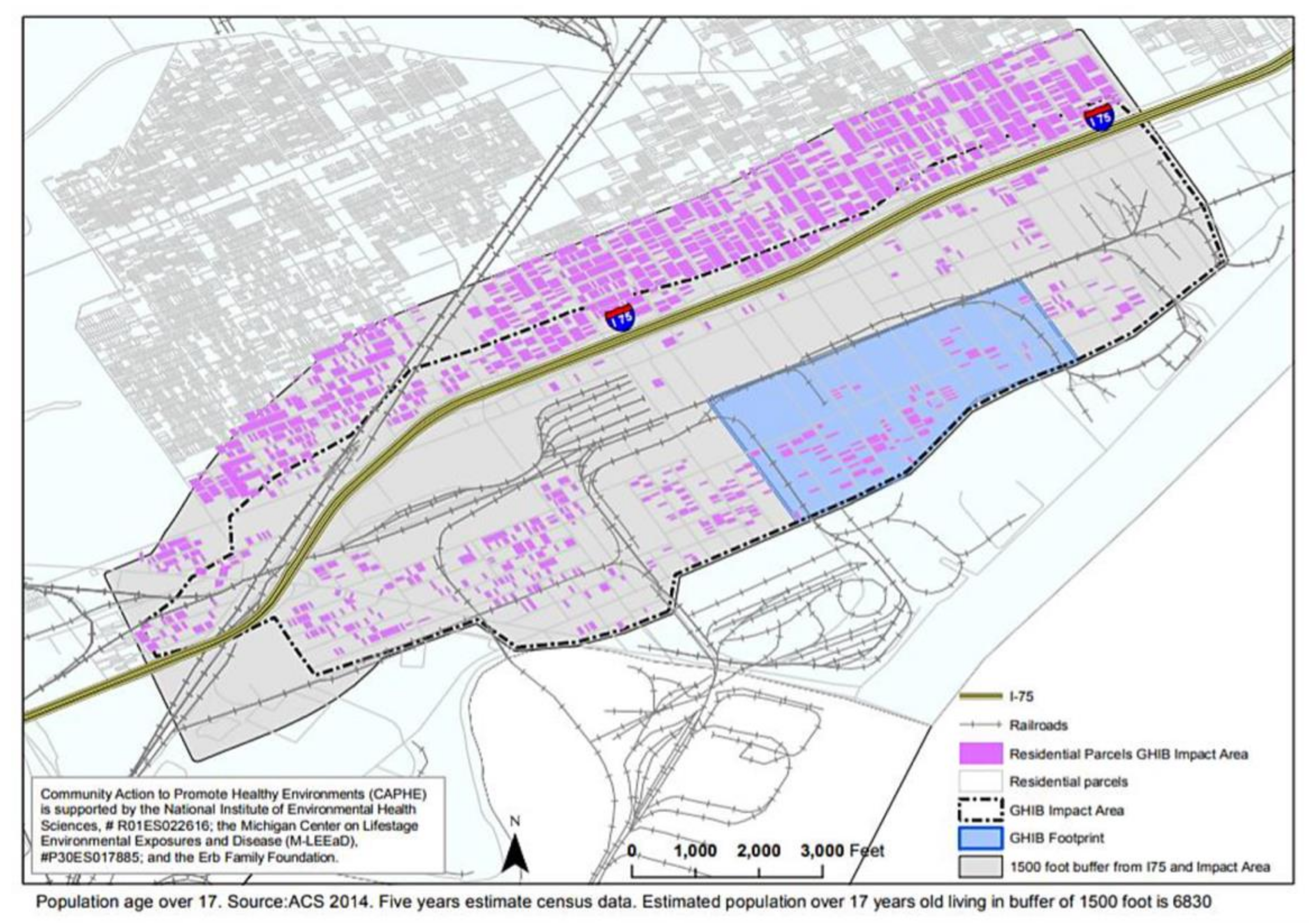
2.1. Cumulative Impacts for Delray and Surrounding Community
2.2. Health Impact Assessment to Inform Community Benefits
- Testifying at state hearings at multiple points in the bridge deliberations;
- Organizing a ‘Visit Before you Vote’ campaign, and a tour of the affected area for elected officials and bridge decision-makers to humanize land use decisions;
- Holding call-in days to mayors, city council, and the Governor’s office to inform specific decisions;
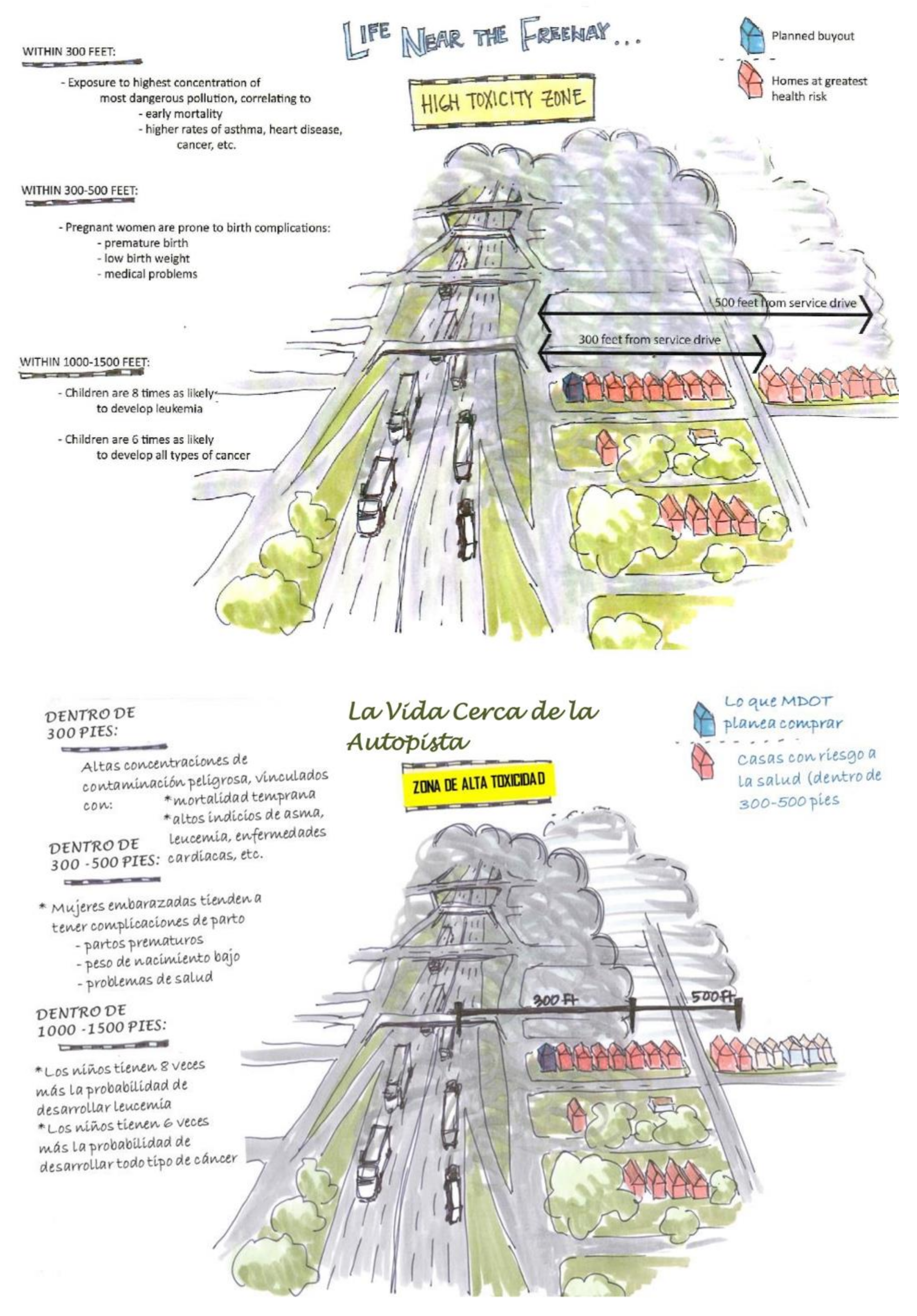
- Signing thousands of postcards and organizing petitions to advocate for community benefits (see Figure 3);
- Conducting community-led studies on truck traffic and routes, air quality, and health of residents to share with decision-makers;
- Door-knocking and holding countless CBC meetings to inform residents of data, pending decisions, and opportunities to engage.
3. Materials and Methods
3.1. Community-Led Data Collection
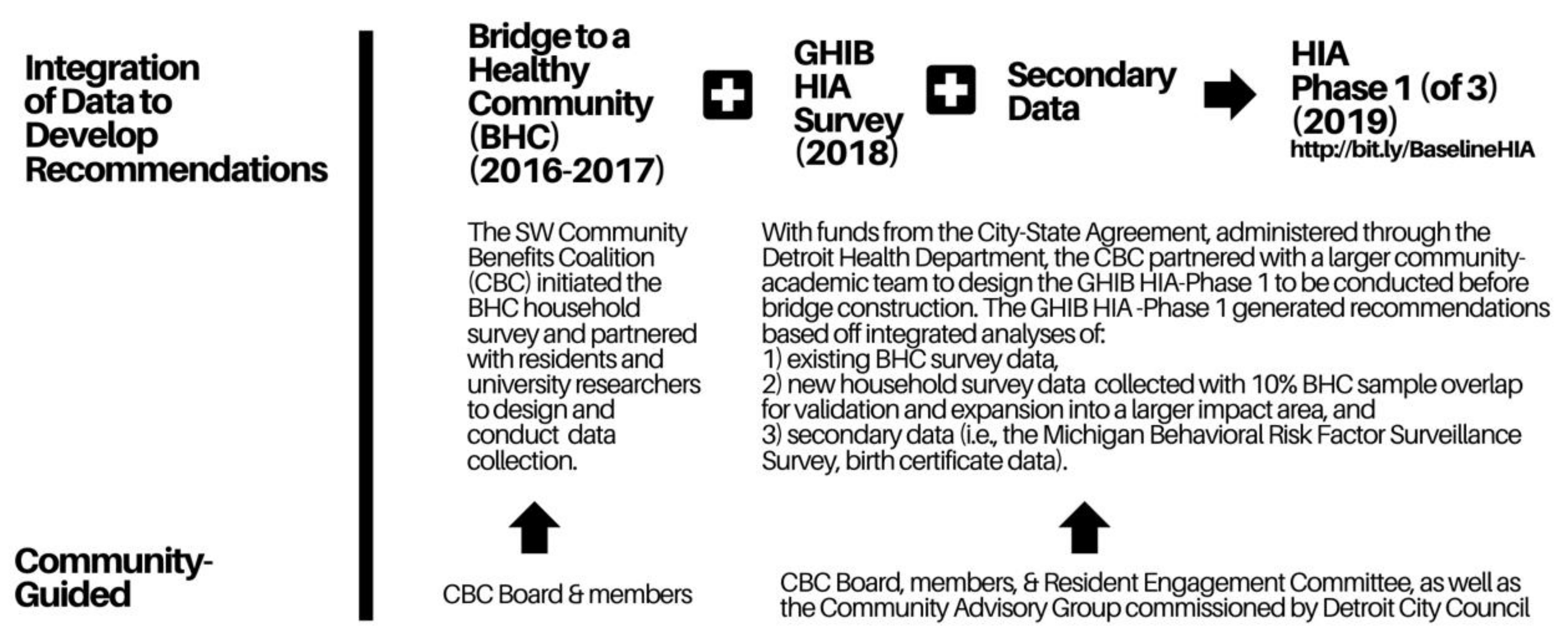
3.2. Designing a Community-Driven Health Impact Assessment
3.3. Data Analysis
4. Results
- (1)
- Reduce emissions of air pollutants or noise associated with the new GHIB;
- (2)
- Reduce the exposure of residents to air pollutants or noise emitted as a result of GHIB activity;
- (3)
- Reduce adverse health effects among residents whose health is impacted by air pollutants or noise in the GHIB area.
4.1. Demographic & Health Characteristics
4.2. Neighborhood Perceptions and Plans to Move
5. Discussion
- Expanding the optional home swap program to include all residents living within 500 feet of the new bridge;
- Expanding the number of homes eligible for windows and indoor air filters to reduce indoor air pollutants;
- Assuring that entrance and exit ramps and truck routes avoid residential neighborhoods;
- And increasing enforcement of existing idling policies and truck routes.
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bureau of Transportation Statistics. 2020. Available online: https://www.bts.gov/newsroom/january-2020-north-american-transborder-freight-numbers (accessed on 6 June 2020).
- Ontario Michigan Border Transportation Partnership Planning/Need and Feasibility Study. 2002. Available online: http://www.partnershipborderstudy.com/pdf/PNF%20Progress%20Report%201%20-%20March%2002.pdf (accessed on 6 June 2020).
- U.S. Department of Transportation & Michigan Department of Transportation. Final Environmental Impact Statement. 2008. Available online: http://www.partnershipborderstudy.com/reports_us.asp#feis (accessed on 6 June 2020).
- Lougheed, T. Arising from the Ashes? Environmental health in Detroit. Environ. Health Perspect. 2014, 122, A324–A331. [Google Scholar] [CrossRef] [PubMed]
- Martenies, S.E.; Milando, C.W.; Batterman, S.A. Air pollutant strategies to reduce adverse health impacts and health inequalities: A quantitative assessment for Detroit, Michigan. Air Qual. Atmos. Health 2018, 11, 409–422. [Google Scholar] [CrossRef] [PubMed]
- Snyder, R. New International Trade Crossing agreement to Bring Jobs, Economic Security, Easier Travel, 2012, June 15. [press release]. Available online: https://www.michigan.gov/formergovernors/0,4584,7-212-96477_90815_57657-280608--,00.html (accessed on 6 June 2020).
- Minnesota Health Impact Coalition. Minnesota HIA Action Guide; Minnesota Department of Health: St. Paul, MN, USA, 2016; Available online: https://www.health.state.mn.us/communities/environment/hia/docs/mnhiaguide.pdf. (accessed on 6 September 2020).
- Reyes, A.; Schulz, A.; Sampson, N.; Sagovac, S.; Rice, K.; Mentz, G.; DeMajo, R.; Vial, B.; Gamboa, C. Baseline Health Impact Assessment of the Gordie Howe Bridge Project; Detroit Health Department: Detroit, MI, USA, 2019; Available online: http://bit.ly/BaselineHIA (accessed on 6 September 2020).
- Great Lakes Water Authority/Detroit Water and Sewerage Department. Available online: https://www.michigan.gov/egle/0,9429,7-135-3313_71618_3682_3713-298007--,00.html (accessed on 6 September 2020).
- Chen, H.; Kwong, J.C.; Copes, R.; Tu, K.; Villeneuve, P.J.; Van Donkelaar, A.; Hystad, P.; Martin, R.V.; Murray, B.J.; Jessiman, B.; et al. Living near major roads and the incidence of dementia, Parkinson’s disease, and multiple sclerosis: A population-based cohort study. Lancet 2017, 389, 718–726. [Google Scholar] [CrossRef]
- Health Effects Institute. Traffic-Related Air Pollution: A Critical Review of the Literature on Emissions, Exposure, and Health Effects. 2010. Available online: https://www.healtheffects.org/publication/traffic-related-air-pollution-critical-reviewliterature-emissions-exposure-and-health (accessed on 6 September 2020).
- Urman, R.; Eckel, S.; Deng, H.; Berhane, K.; Avol, E.; Lurmann, F.; McConnell, R.; Gilliland, F. Risk effects of near-roadway pollutants and asthma status on bronchitic symptoms in children. Environ. Epidemiol. 2018, 2, e012. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, M.; Hricko, A.; Gottlieb, R.; DeLara, J. Global Trade Impacts: Addressing the Health, Social and Environmental Consequences of Moving International Freight through Our Communities. 2011. Available online: http://scholar.oxy.edu/uep_faculty/411. (accessed on 6 June 2020).
- Michigan Department of Environment, Great Lakes, and Energy. Attainment Status for the National Ambient Air Quality Standards. 2019. Available online: https://www.michigan.gov/documents/deq/deq-aqd-aqe-mi_attainment_status_map_407842_7.pdf (accessed on 6 June 2020).
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Clark, C.; Sbihi, H.; Tamburic, L.; Brauer, M.; Frank, L.D.; Davies, H.W. Association of long-term exposure to transportation noise and traffic-related air pollution with the incidence of diabetes: A prospective cohort study. Environ. Health Perspect. 2017, 125, 087025. [Google Scholar] [CrossRef]
- Hricko, A. Guest editorial: Ships, trucks, and trains: Effects of goods movement on environmental health. Environ. Health Perspect. 2006, 114, A204–A205. [Google Scholar] [CrossRef] [PubMed]
- Hricko, A. Global trade comes home: Community impacts of goods movement. Environ. Health Perspect. 2008, 116, A78–A81. [Google Scholar] [CrossRef]
- Schulz, A.J.; Mentz, G.B.; Sampson, N.; Ward, M.; Anderson, R.; De Majo, R.; Israel, B.A.; Lewis, T.; Wilkins, D. Race and the distribution of social and physical environmental risk: A case example from the Detroit Metropolitan Area. Du Bois Rev. 2016, 13, 285–304. [Google Scholar] [CrossRef]
- Kim, J.J. Ambient air pollution: Health hazards to children. Pediatrics 2004, 114, 1699–1707. [Google Scholar] [CrossRef]
- Medina-Ramón, M.; Schwartz, J. Who is more vulnerable to die from ozone air pollution? Epidemiology 2008, 19, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, L.; Zhou, J. Neighborhood air quality, respiratory health, and vulnerable populations in compact and sprawled regions. J. Am. Plan. Assoc. 2010, 76, 363–371. [Google Scholar] [CrossRef]
- Birley, M. The Health Impact Assessment of Development Projects; Her Majesty’s Stationery Office: London, UK, 1995. [Google Scholar]
- Kemm, J. Health Impact Assessment: Past Achievement, Current Understanding, and Future Progress; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Dannenberg, A.L.; Bhatia, R.; Cole, B.L.; Heaton, S.K.; Feldman, J.D.; Rutt, C.D. Use of health impact assessment in the US: 27 case studies, 1999–2007. Am. J. Prev. Med. 2008, 34, 241–256. [Google Scholar] [CrossRef]
- Phillips, R.; Wong, C. Handbook of Community Well-Being Research; Springer: New York, NY, USA, 2017. [Google Scholar]
- Solomon, G.; Morello-Frosch, R.; Zeise, L.; Faust, J.B. Cumulative environmental impacts: Science and policy to protect communities. Annu. Rev. Public Health 2016, 37, 83–96. [Google Scholar] [CrossRef] [PubMed]
- American Community Survey: 2012–2016. Data Survey at Block Group Level. Available online: https://www.census.gov/programs-surveys/acs (accessed on 6 June 2020).
- Fulllilove, M.T. Root shock: How Tearing up City Neighborhoods Hurts America and What We Can Do about It, 2nd ed.; New Village Press: New York, NY, USA, 2016. [Google Scholar]
- Trounstine, J. Segregation by Design: Local Politics and Inequality in American Cities; Cambridge University Press (CUP): Cambridge, UK, 2018. [Google Scholar]
- Sugrue, T.J. The Origins of the Urban Crisis: Race and Inequality in Postwar Detroit, 2nd ed.; Princeton University Press: Princeton, NJ, USA, 2014. [Google Scholar]
- Hricko, A.; Rowland, G.; Eckel, S.P.; Logan, A.; Taher, M.; Wilson, J. Global trade, local impacts: Lessons from California on health impacts and environmental justice concerns for residents living near freight rail yards. Int. J. Environ. Res. Public Health 2014, 11, 1914–1941. [Google Scholar] [CrossRef]
- Environmental Protection Agency. Reducing Air Emissions Associated with Goods Movement: Working Towards Environmental Justice. 2009. Available online: https://www.epa.gov/sites/production/files/2015-02/documents/2009-goods-movement.pdf (accessed on 6 June 2020).
- Lee, C. A game changer in the making? Lessons from states advancing environmental justice through mapping and cumulative impact strategies. Environ. Law Rep. 2020, 50, 10203. [Google Scholar]
- Ellickson, K.M.; Sevcik, S.M.; Burman, S.; Pak, S.; Kohlasch, F.; Pratt, G.C. Cumulative risk assessment and environmental equity in air permitting: Interpretation, methods, community participation and implementation of a unique statute. Int. J. Environ. Res. Public Health 2011, 8, 4140–4159. [Google Scholar] [CrossRef]
- Waheed, F.; Ferguson, G.M.; Ollson, C.A.; MacLellan, J.I.; McCallum, L.C.; Cole, D.C. Health impact assessment of transportation projects, plans and policies: A scoping review. Environ. Impact Assess. Rev. 2018, 71, 17–25. [Google Scholar] [CrossRef]
- Richter, L. Constructing insignificance: Critical race perspectives on institutional failure in environmental justice communities. Environ. Sociol. 2017, 4, 107–121. [Google Scholar] [CrossRef]
- Christakopoulou, S.; Dawson, J.; Gari, A. The community well-being questionnaire: Theoretical context and initial assessment of its reliability and validity. Soc. Indic. Res. 2001, 56, 319–349. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The Public Health System & the 10 Essential Public Health Services. Available online: https://www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html (accessed on 6 June 2020).
- American Public Health Association. Policy Statement: Addressing Environmental Justice to Achieve Health Equity. Available online: https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2020/01/14/addressing-environmental-justice-to-achieve-health-equity (accessed on 6 June 2020).
- Cromar, K.; Duncan, B.N.; Bartoňová, A.; Benedict, K.; Brauer, M.; Habre, R.; Hagler, G.S.W.; Haynes, J.A.; Khan, S.; Kilaru, V.; et al. Air pollution monitoring for health research and patient care. An official american thoracic society workshop report. Ann. Am. Thorac. Soc. 2019, 16, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Tishman Environment and Design Center. Local Policies for Environmental Justice: A National Scan; Natural Resources Defense Council: Boston, MA, USA, 2019; Available online: https://www.nrdc.org/sites/default/files/local-policies-environmental-justice-national-scan-tishman-201902.pdf (accessed on 6 June 2020).
- Environmental Justice and Cumulative Impact Ordinance 16-0803, Newark, NJ. 2016. Available online: https://newark.legistar.com/LegislationDetail.aspx?ID=2770971&GUID=D0C566D0-463A-482D-A4AC-78884351DA79&FullText=1 (accessed on 6 June 2020).
- City of Detroit. Community Benefits Ordinance, No. 35-16 Ordinance. 2016. Available online: https://detroitmi.gov/document/ordinance-no-35-16-community-benefits-ordinance (accessed on 6 June 2020).
- Sampson, N.R.; Schulz, A.J.; Parker, E.A.; Israel, B.A. Improving public participation to achieve environmental justice: Applying lessons from freight’s frontline communities. Environ. Justice 2014, 7, 45–54. [Google Scholar] [CrossRef]
- Woolcock, M. When do development projects enhance community well-being? Int. J. Community Well-Being 2019, 2, 81–89. [Google Scholar] [CrossRef]
- Iroz-Elardo, N. Health impact assessment as community participation. Community Dev. J. 2014, 50, 280–295. [Google Scholar] [CrossRef]
- Gilhuly, K.; Purciel, M.; Farhang, L.; Lucky, J.; Harris, E.C.; Heller, J.; Seto, E.Y.W. Using health impact assessment in community development to improve air quality and public health. Community Dev. 2011, 42, 193–207. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Critical issues in developing and following CBPR principles. In Community-Based Participatory Research for Health: From Process to Outcomes, 2nd ed.; Minkler, M., Wallerstein, N., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 47–66. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | Survey Respondents (2016, 2018) (n = 435) (A) | American Community Survey ≥ 18 Years Old (n = 11,320) * (B) | p-Value A vs. B | Survey Household Members (n = 1629) (C) | American Community Survey All Household Residents (n = 16,382) (D) | p-Value C vs. D | p-Value A vs. D | |
|---|---|---|---|---|---|---|---|---|
| Age (in years) | ≤4 | 0.4343 | 9.1 | 9.9 | 0.084 | |||
| 5–17 | 27.9 | 21 | ||||||
| 18–64 | 85.9 | 87.2 | 56 | 60.3 | ||||
| ≥65 | 14.1 | 12.8 | 7.1 | 8.8 | ||||
| Gender ** | Female | 68.1 | 50.5 | <0.001 | n.a. | 50.7 | ||
| Male | 32.0 | 49.5 | 49.3 | |||||
| Education | <High School Graduation | 48.7 | n.a. | n.a. | 46.2 | 0.464 | ||
| High School Graduation | 28.9 | 30.6 | ||||||
| >High School Graduation | 22.4 | 23.3 | ||||||
| Self-Reported Asthma or Allergies Affecting Breathing or Asthma | Age Group | GHIB Area | GHIB Area | |
|---|---|---|---|---|
| ≤500 Feet | >500 Feet | All | ||
| Asthma | <18 years * | 16.3 | 11.6 | 13.8 |
| Under 5 years | 9.8 | 4.6 | 7.4 | |
| 5–17 years | 19.0 | 13.4 | 15.9 | |
| 18–40 years | 9.1 | 6.6 | 7.7 | |
| 41–64 years | 14.4 | 13.6 | 13.9 | |
| ≥65 | 24.4 | 12.9 | 17.4 | |
| Allergies affecting breathing or asthma | <18 years ** | 28.7 | 20.4 | 24.3 |
| Under 5 years | 18.3 | 10.6 | 14.9 | |
| 5–17 years ** | 33.0 | 22.9 | 27.4 | |
| 18–40 years | 25.5 | 20.9 | 22.9 | |
| 41–64 years | 34.8 | 29.7 | 31.9 | |
| ≥65 | 42.2 | 32.9 | 36.5 | |
| Perceptions of Neighborhood | n * | % Agree or Strongly Agree Unweighted Weighted | |
|---|---|---|---|
| I think this neighborhood is a good place for me to live. | 431 | 70.3 | 70.5 |
| People in this neighborhood share the same values. | 417 | 69.5 | 69.8 |
| I feel at home in this neighborhood. | 431 | 85.2 | 85.6 |
| It is very important to me to live in this particular neighborhood. | 433 | 63.3 | 64.0 |
| I expect to live in this neighborhood for a long time. | 424 | 68.6 | 69.6 |
| People in this neighborhood generally know each other. | 429 | 81.1 | 81.9 |
| Plan to Move | % Living in Impact Area (n = 224) | % Living in Buffer Area (n = 211) | Statistical Test of Difference * |
|---|---|---|---|
| Within one year | 8.6 | 5.3 | 0.01 |
| Between 1–5 years | 17.7 | 10.4 | |
| More than 5 years | 5.9 | 4.7 | |
| Not planning to move | 57.8 | 73.6 |
| Neighborhood Concerns | Very Much a Concern (%) | Somewhat of a Concern (%) | Not a Concern at all (%) |
|---|---|---|---|
| Rats | 81.6 | 9.2 | 9.2 |
| Traffic congestion making it hard to get places | 76.1 | 8.8 | 15.9 |
| Clogged sewers or standing water in streets | 75.3 | 11.6 | 13.1 |
| Outdoor air quality, such as emissions from trucks industry, fumes or odors | 66.7 | 18.8 | 14.6 |
| Vibration from trucks or construction activity damaging property | 60.9 | 18.4 | 20.7 |
| Vacant houses | 60.4 | 16.2 | 23.3 |
| Road dust | 60.2 | 20.0 | 19.9 |
| Loss of property value | 56.7 | 21.3 | 22.0 |
| Crime | 55.0 | 23.9 | 21.1 |
| Truck traffic on residential streets affecting safety | 54.8 | 16.1 | 29.1 |
| Noise during sleeping hours | 47.1 | 20.3 | 32.6 |
| Indoor air quality, such as fumes and dust inside the house | 41.4 | 25.1 | 33.5 |
| Noise during the day | 40.9 | 29.8 | 29.3 |
| Many residents moving away | 23.8 | 35.6 | 40.6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampson, N.; Sagovac, S.; Schulz, A.; Fink, L.; Mentz, G.; Reyes, A.; Rice, K.; de Majo, R.; Gamboa, C.; Vial, B. Mobilizing for Community Benefits to Assess Health and Promote Environmental Justice near the Gordie Howe International Bridge. Int. J. Environ. Res. Public Health 2020, 17, 4680. https://doi.org/10.3390/ijerph17134680
Sampson N, Sagovac S, Schulz A, Fink L, Mentz G, Reyes A, Rice K, de Majo R, Gamboa C, Vial B. Mobilizing for Community Benefits to Assess Health and Promote Environmental Justice near the Gordie Howe International Bridge. International Journal of Environmental Research and Public Health. 2020; 17(13):4680. https://doi.org/10.3390/ijerph17134680
Chicago/Turabian StyleSampson, Natalie, Simone Sagovac, Amy Schulz, Lauren Fink, Graciela Mentz, Angela Reyes, Kristina Rice, Ricardo de Majo, Cindy Gamboa, and Bridget Vial. 2020. "Mobilizing for Community Benefits to Assess Health and Promote Environmental Justice near the Gordie Howe International Bridge" International Journal of Environmental Research and Public Health 17, no. 13: 4680. https://doi.org/10.3390/ijerph17134680
APA StyleSampson, N., Sagovac, S., Schulz, A., Fink, L., Mentz, G., Reyes, A., Rice, K., de Majo, R., Gamboa, C., & Vial, B. (2020). Mobilizing for Community Benefits to Assess Health and Promote Environmental Justice near the Gordie Howe International Bridge. International Journal of Environmental Research and Public Health, 17(13), 4680. https://doi.org/10.3390/ijerph17134680