A Pilot Study of Musculoskeletal Abnormalities in Patients in Recovery from a Unilateral Rupture-Repaired Achilles Tendon


 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Recruitment
2.2. Achilles Tendon Length Measurement
2.3. Experimental Protocol and Procedure Maryland
2.4. Musculoskeletal Modeling
2.5. Model Validation and Sensitivity
2.6. Data and Statistical Analysis
3. Results
3.1. Achilles Tendon Length
3.2. Joint Kinematics
3.3. Joint Moments
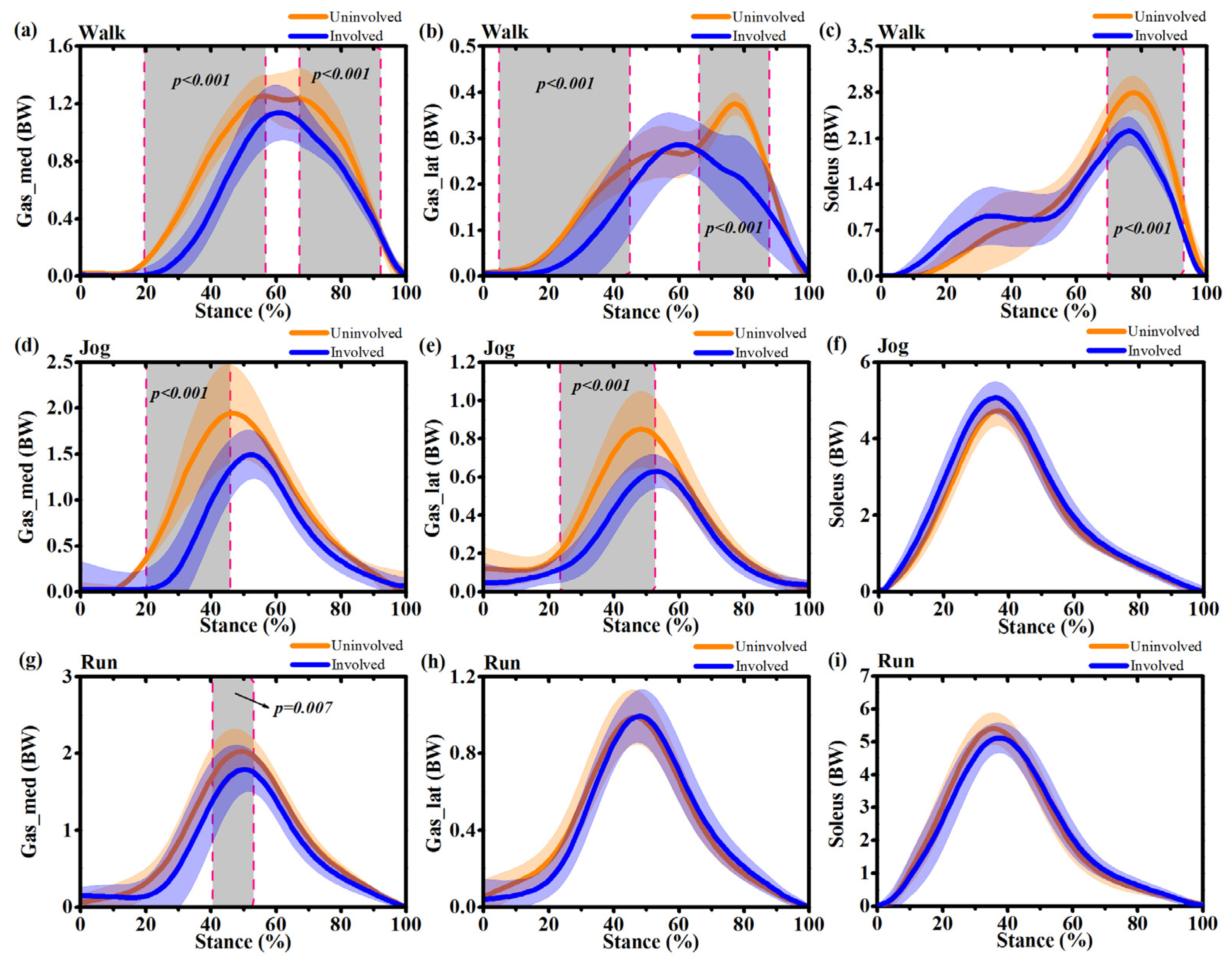
3.4. Muscle Forces
3.5. Joint Reaction Forces
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lantto, I.; Heikkinen, J.; Flinkkilä, T.; Ohtonen, P.; Leppilahti, J. Epidemiology of Achilles tendon ruptures: Increasing incidence over a 33-year period. Scand. J. Med. Sci. Sport 2015, 25, e133–e138. [Google Scholar] [CrossRef] [PubMed]
- Ganestam, A.; Kallemose, T.; Troelsen, A.; Barfod, K.W. Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3730–3737. [Google Scholar] [CrossRef] [PubMed]
- Mullaney, M.J.; McHugh, M.P.; Tyler, T.F.; Nicholas, S.J.; Lee, S.J. Weakness in end-range plantar flexion after achilles tendon repair. Am. J. Sports Med. 2006, 34, 1120–1125. [Google Scholar] [CrossRef] [PubMed]
- Barfod, K.W.; Bencke, J.; Lauridsen, H.B.; Dippmann, C.; Ebskov, L.; Troelsen, A. Nonoperative, dynamic treatment of acute achilles tendon rupture: Influence of early weightbearing on biomechanical properties of the plantar flexor muscle-tendon complex-a blinded, randomized, controlled trial. J. Foot Ankle Surg. 2015, 54, 220–226. [Google Scholar] [CrossRef]
- Heikkinen, J.; Lantto, I.; Flinkkila, T.; Ohtonen, P.; Niinimaki, J.; Siira, P.; Laine, V.; Leppilahti, J. Soleus Atrophy is Common after the Nonsurgical Treatment of Acute Achilles Tendon Ruptures: A Randomized Clinical Trial Comparing Surgical and Nonsurgical Functional Treatments. Am. J. Sports Med. 2017, 45, 1395–1404. [Google Scholar] [CrossRef]
- Heikkinen, J.; Lantto, I.; Piilonen, J.; Flinkkilä, T.; Ohtonen, P.; Siira, P.; Laine, V.; Niinimäki, J.; Pajala, A.; Leppilahti, J. Tendon Length, Calf Muscle Atrophy, and Strength Deficit After Acute Achilles Tendon Rupture. J. Bone Jt. Surg. 2017, 99, 1509–1515. [Google Scholar] [CrossRef]
- Rosso, C.; Buckland, D.M.; Polzer, C.; Sadoghi, P.; Schuh, R.; Weisskopf, L.; Vavken, P.; Valderrabano, V. Long-term biomechanical outcomes after Achilles tendon ruptures. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 890–898. [Google Scholar] [CrossRef]
- Suydam, S.M.; Buchanan, T.S.; Manal, K.; Silbernagel, K.G. Compensatory muscle activation caused by tendon lengthening post-Achilles tendon rupture. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 868–874. [Google Scholar] [CrossRef]
- Olsson, N.; Nilsson-Helander, K.; Karlsson, J.; Eriksson, B.I.; Thomée, R.; Faxén, E.; Silbernagel, K.G. Major functional deficits persist 2 years after acute Achilles tendon rupture. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1385–1393. [Google Scholar] [CrossRef]
- Jandacka, D.; Zahradnik, D.; Foldyna, K.; Hamill, J. Running biomechanics in a long-term monitored recreational athlete with a history of achilles tendon rupture. BMJ Case Rep. 2013. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.L.; Logan, K.; Heylings, D.; Donell, S.T.; Tucker, K. The effect of Achilles tendon lengthening on ankle dorsiflexion: A cadaver study. Foot Ankle Int. 2006, 27, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Goren, D.; Ayalon, M.; Nyska, M. Isokinetic strength and endurance after percutaneous and open surgical repair of achilles tendon ruptures. Foot Ankle Int. 2005, 26, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Almonroeder, T.; Willson, J.D.; Kernozek, T.W. The effect of foot strike pattern on achilles tendon load during running. Ann. Biomed. Eng. 2013, 41, 1758–1766. [Google Scholar] [CrossRef] [PubMed]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef]
- Seth, A.; Hicks, J.L.; Uchida, T.K.; Habib, A.; Dembia, C.L.; Dunne, J.J.; Ong, C.F.; DeMers, M.S.; Rajagopal, A.; Millard, M.; et al. OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS Comput. Biol. 2018, 14, e1006223. [Google Scholar] [CrossRef]
- Smale, K.B.; Conconi, M.; Sancisi, N.; Krogsgaard, M.; Alkjaer, T.; Parenti-Castelli, V.; Benoit, D.L. Effect of implementing magnetic resonance imaging for patient-specific OpenSim models on lower-body kinematics and knee ligament lengths. J. Biomech. 2019, 83, 9–15. [Google Scholar] [CrossRef]
- Harris, M.D.; MacWilliams, B.A.; Bo Foreman, K.; Peters, C.L.; Weiss, J.A.; Anderson, A.E. Higher medially-directed joint reaction forces are a characteristic of dysplastic hips: A comparative study using subject-specific musculoskeletal models. J. Biomech. 2017, 54, 80–87. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Board, W.J.; Browning, R.C. Pediatric obesity and walking duration increase medial tibiofemoral compartment contact forces. J. Orthop. Res. 2016, 34, 97–105. [Google Scholar] [CrossRef]
- Modenese, L.; Montefiori, E.; Wang, A.; Wesarg, S.; Viceconti, M.; Mazzà, C. Investigation of the dependence of joint contact forces on musculotendon parameters using a codified workflow for image-based modelling. J. Biomech. 2018, 73, 108–118. [Google Scholar] [CrossRef]
- Sun, D.; Fekete, G.; Mei, Q.; Gu, Y. Gait Abnormality and Asymmetry Analysis After 18–24 Months Surgical Repair of Unilateral Achilles Tendon Rupture. J. Med. Imaging Heal. Inform. 2019, 9, 552–560. [Google Scholar] [CrossRef]
- Nilsson-Helander, K.; Thomeé, R.; Grävare-Silbernagel, K.; Thomeé, P.; Faxén, E.; Eriksson, B.I.; Karlsson, J. The Achilles tendon Total Rupture Score (ATRS): Development and validation. Am. J. Sports Med. 2007, 35, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Strickland, J.W. Flexor Tendon Injuries: II. Operative Technique. J. Am. Acad. Orthop. Surg. 1995, 3, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Kunimasa, Y.; Sano, K.; Oda, T.; Nicol, C.; Komi, P.V.; Locatelli, E.; Ito, A.; Ishikawa, M. Specific muscle-tendon architecture in elite Kenyan distance runners. Scand. J. Med. Sci. Sport. 2014, 24, e269–e274. [Google Scholar] [CrossRef]
- Barfod, K.W.; Riecke, A.F.; Boesen, A.; Hansen, P.; Maier, J.F.; Døssing, S.; Troelsen, A. Validation of a novel ultrasound measurement of achilles tendon length. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3398–3406. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Gu, Y.; Xiang, L.; Baker, J.S.; Fernandez, J. Foot Pronation Contributes to Altered Lower Extremity Loading After Long Distance Running. Front. Physiol. 2019, 10, 573. [Google Scholar] [CrossRef] [PubMed]
- Moissenet, F.; Bélaise, C.; Piche, E.; Michaud, B.; Begon, M. An Optimization Method Tracking EMG, Ground Reactions Forces, and Marker Trajectories for Musculo-Tendon Forces Estimation in Equinus Gait. Front. Neurorobot. 2019, 13, 48. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Browning, R.C. Compressive and shear hip joint contact forces are affected by pediatric obesity during walking. J. Biomech. 2016. [Google Scholar] [CrossRef]
- Lerner, Z.F.; DeMers, M.S.; Delp, S.L.; Browning, R.C. How tibiofemoral alignment and contact locations affect predictions of medial and lateral tibiofemoral contact forces. J. Biomech. 2015. [Google Scholar] [CrossRef]
- Steele, K.M.; DeMers, M.S.; Schwartz, M.H.; Delp, S.L. Compressive tibiofemoral force during crouch gait. Gait Posture 2012, 35, 556–560. [Google Scholar] [CrossRef]
- Fukuchi, R.K.; Fukuchi, C.A.; Duarte, M. A public dataset of running biomechanics and the effects of running speed on lower extremity kinematics and kinetics. PeerJ 2017, 5, e3298. [Google Scholar] [CrossRef]
- Hebenstreit, F.; Leibold, A.; Krinner, S.; Welsch, G.; Lochmann, M.; Eskofier, B.M. Effect of walking speed on gait sub phase durations. Hum. Mov. Sci. 2015. [Google Scholar] [CrossRef] [PubMed]
- Lohman, E.B.; Balan Sackiriyas, K.S.; Swen, R.W. A comparison of the spatiotemporal parameters, kinematics, and biomechanics between shod, unshod, and minimally supported running as compared to walking. Phys. Ther. Sport 2011, 12, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Pataky, T.C.; Robinson, M.A.; Vanrenterghem, J. Vector field statistical analysis of kinematic and force trajectories. J. Biomech. 2013. [Google Scholar] [CrossRef]
- Agres, A.N.; Duda, G.N.; Gehlen, T.J.; Arampatzis, A.; Taylor, W.R.; Manegold, S. Increased unilateral tendon stiffness and its effect on gait 2–6 years after Achilles tendon rupture. Scand. J. Med. Sci. Sport. 2015. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Sun, D.; Fekete, G. Ba Duan Jin Preliminary Analysis of the Second Type of Plantar Pressure. Physical Activity and Health. 2018, 2, 1–7. [Google Scholar] [CrossRef]
- Don, R.; Ranavolo, A.; Cacchio, A.; Serrao, M.; Costabile, F.; Iachelli, M.; Camerota, F.; Frascarelli, M.; Santilli, V. Relationship between recovery of calf-muscle biomechanical properties and gait pattern following surgery for achilles tendon rupture. Clin. Biomech. 2007, 22, 211–220. [Google Scholar] [CrossRef]
- Speedtsberg, M.B.; Kastoft, R.; Barfod, K.W.; Penny, J.; Bencke, J. Gait Function and Postural Control 4.5 Years After Nonoperative Dynamic Treatment of Acute Achilles Tendon Ruptures. Orthop. J. Sport. Med. 2019. [Google Scholar] [CrossRef]
- Rosso, C.; Vavken, P.; Polzer, C.; Buckland, D.M.; Studler, U.; Weisskopf, L.; Lottenbach, M.; Müller, A.M.; Valderrabano, V. Long-term outcomes of muscle volume and Achilles tendon length after Achilles tendon ruptures. Knee Surger. Sport. Traumatol. Arthrosc. 2013. [Google Scholar] [CrossRef]
- Willy, R.W.; Brorsson, A.; Powell, H.C.; Willson, J.D.; Tranberg, R.; Grävare Silbernagel, K. Elevated Knee Joint Kinetics and Reduced Ankle Kinetics Are Present during Jogging and Hopping after Achilles Tendon Ruptures. Am. J. Sports Med. 2017. [Google Scholar] [CrossRef]
- Nilsson-Helander, K.; Grävare Silbernagel, K.; Thomeé, R.; Faxén, E.; Olsson, N.; Eriksson, B.I.; Karlsson, J. Acute achilles tendon rupture: A randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am. J. Sports Med. 2010. [Google Scholar] [CrossRef]
- Chan, A.P.H.; Chan, Y.Y.; Fong, D.T.P.; Wong, P.Y.K.; Lam, H.Y.; Lo, C.K.; Yung, P.S.H.; Fung, K.Y.; Chan, K.M. Clinical and biomechanical outcome of minimal invasive and open repair of the Achilles tendon. Sport. Med. Arthrosc. Rehabil. Ther. Technol. 2011. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Ugbolue, U.C. Is There a Relationship Between Strike Pattern and Injury During Running: A Review. Physical Activity and Health. 2019, 3, 127–134. [Google Scholar] [CrossRef]
- Jandacka, D.; Plesek, J.; Skypala, J.; Uchytil, J.; Silvernail, J.F.; Hamill, J. Knee Joint Kinematics and Kinetics During Walking and Running After Surgical Achilles Tendon Repair. Orthop. J. Sport. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Grävare Silbernagel, K.; Willy, R.; Davis, I. Preinjury and Postinjury Running Analysis Along with Measurements of Strength and Tendon Length in a Patient With a Surgically Repaired Achilles Tendon Rupture. J. Orthop. Sports Phys. Ther. 2012, 42, 521–529. [Google Scholar] [CrossRef]
- Cooper, A.; Alghamdi, G.A.; Alghamdi, M.A.; Altowaijri, A.; Richardson, S. The Relationship of Lower Limb Muscle Strength and Knee Joint Hyperextension during the Stance Phase of Gait in Hemiparetic Stroke Patients. Physiother. Res. Int. 2012. [Google Scholar] [CrossRef]
- Peng, W.C.; Chao, Y.H.; Fu, A.S.N.; Fong, S.S.M.; Rolf, C.; Chiang, H.; Chen, S.; Wang, H.K. Muscular Morphomechanical Characteristics After an Achilles Repair. Foot Ankle Int. 2019. [Google Scholar] [CrossRef]
- Farrokhi, S.; Keyak, J.H.; Powers, C.M. Individuals with patellofemoral pain exhibit greater patellofemoral joint stress: A finite element analysis study. Osteoarthr. Cartil. 2011. [Google Scholar] [CrossRef]
- Draper, C.E.; Fredericson, M.; Gold, G.E.; Besier, T.F.; Delp, S.L.; Beaupre, G.S.; Quon, A. Patients with patellofemoral pain exhibit elevated bone metabolic activity at the patellofemoral joint. J. Orthop. Res. 2012. [Google Scholar] [CrossRef]
- Bennett, J.E.; Reinking, M.F.; Pluemer, B.; Pentel, A.; Seaton, M.; Killian, C. Factors contributing to the development of medial tibial stress syndrome in high school runners. J. Orthop. Sports Phys. Ther. 2001. [Google Scholar] [CrossRef]
- Baxter, J.R.; Hullfish, T.J.; Chao, W. Functional deficits may be explained by plantarflexor remodeling following Achilles tendon rupture repair: Preliminary findings. J. Biomech. 2018. [Google Scholar] [CrossRef]
- Powell, H.C.; Silbernagel, K.G.; Brorsson, A.; Tranberg, R.; Willy, R.W. Individuals post achilles tendon rupture exhibit asymmetrical knee and ankle kinetics and loading rates during a drop countermovement jump. J. Orthop. Sports Phys. Ther. 2018. [Google Scholar] [CrossRef] [PubMed]
- Geremia, J.M.; Bobbert, M.F.; Casa Nova, M.; Ott, R.D.; De Aguiar Lemos, F.; De Oliveira Lupion, R.; Frasson, V.B.; Vaz, M.A. The structural and mechanical properties of the Achilles tendon 2 years after surgical repair. Clin. Biomech. 2015, 30, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Liang, Z.; Li, S. The Plantar Pressure Analysis of Open Stance Forehand in Female Tennis Players. Physical Activity and Health. 2019, 3, 63–70. [Google Scholar] [CrossRef]
- Wang, H.K.; Chiang, H.; Chen, W.S.; Shih, T.T.; Huang, Y.C.; Jiang, C.C. Early neuromechanical outcomes of the triceps surae muscle-tendon after an Achilles’ tendon repair. Arch. Phys. Med. Rehabil. 2013. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Gastrocnemii ATL (mm) | Soleus ATL (mm) | ||||||
|---|---|---|---|---|---|---|---|---|
| IS | US | ISATL/USATL | USATL/ISATL | IS | US | ISATL/USATL | USATL/ISATL | |
| 01 | 228.6 | 201.4 | 1.14 | 0.88 | 56.1 | 54.2 | 1.04 | 0.97 |
| 02 | 242.2 | 221.3 | 1.09 | 0.91 | 62.2 | 58.6 | 1.06 | 0.94 |
| 03 | 235.5 | 212.2 | 1.11 | 0.90 | 53.1 | 51.2 | 1.04 | 0.96 |
| 04 | 236.1 | 205.7 | 1.15 | 0.87 | 66.5 | 63.3 | 1.05 | 0.95 |
| 05 | 224.5 | 207.2 | 1.08 | 0.92 | 58.7 | 55.6 | 1.06 | 0.95 |
| 06 | 231.2 | 214.8 | 1.08 | 0.93 | 60.4 | 57.5 | 1.05 | 0.95 |
| Joint kinematics (°) | IS | US | p-Value | |
|---|---|---|---|---|
| Walking | Hip flexion | 25.3 ± 3.4 | 20.1 ± 2.9 | <0.001 |
| Hip extension | 18.3 ± 2.6 | 22.1 ± 1.8 | 0.03 | |
| Knee flexion | 37.4 ± 4.2 | 39.1 ± 3.7 | 0.42 | |
| Ankle dorsiflexion | 16.2 ± 2.3 | 11.3 ± 2.6 | <0.001 | |
| Ankle plantarflexion | 3.8 ± 2.5 | 10.1 ± 3.2 | <0.001 | |
| Subtalar inversion | 5.1 ± 3.3 | 4.2 ± 2.9 | 0.37 | |
| Subtalar eversion | 1.6 ± 1.1 | 2.2 ± 2.4 | 0.09 | |
| Jogging | Hip flexion | 21.2 ± 3.5 | 19.3 ± 4.4 | 0.28 |
| Hip extension | 10.1 ± 3.1 | 13.2 ± 3.9 | 0.02 | |
| Knee flexion | 35.2 ± 2.9 | 39.7 ± 3.6 | 0.01 | |
| Ankle dorsiflexion | 32.6 ± 4.1 | 27.3±2.9 | <0.001 | |
| Ankle plantarflexion | 5.3 ± 2.8 | 12.4±3.9 | <0.001 | |
| Subtalar inversion | 4.2 ± 3.2 | 8.1 ± 4.5 | <0.001 | |
| Subtalar eversion | 5.4 ± 3.4 | 2.1 ± 3.3 | <0.001 | |
| Running | Hip flexion | 22.3 ± 3.3 | 18.9±3.1 | 0.03 |
| Hip extension | 11.2 ± 2.9 | 13.6±2.8 | 0.01 | |
| Knee flexion | 35.1 ± 5.2 | 40.8±4.9 | 0.04 | |
| Ankle dorsiflexion | 32.3 ± 4.1 | 29.5±4.5 | 0.02 | |
| Ankle plantarflexion | 3.2 ± 2.9 | 10.1±4.3 | <0.001 | |
| Subtalar inversion | 6.2 ± 2.8 | 5.4±3.3 | 0.47 | |
| Subtalar eversion | 4.6 ± 2.5 | 1.3±2.2 | 0.01 |
| Joint Moments (Nm/kg) | IS | US | p-Value | |
|---|---|---|---|---|
| Walking | Hip flexion | 1.42 ± 0.15 | 1.39 ± 0.12 | 0.87 |
| Knee flexion | 0.26 ± 0.14 | 0.42 ± 0.21 | <0.001 | |
| Knee extension | 0.22 ± 0.18 | 0.13 ± 0.20 | <0.001 | |
| Ankle plantarflexion | 1.51 ± 0.16 | 1.50 ± 0.18 | 0.92 | |
| Subtalar eversion | 0.47 ± 0.18 | 0.52 ± 0.22 | 0.21 | |
| Jogging | Hip flexion | 0.71 ± 0.32 | 0.69 ± 0.26 | 0.45 |
| Knee extension | 1.58 ± 0.38 | 1.60 ± 0.42 | 0.33 | |
| Ankle plantarflexion | 2.21 ± 0.42 | 2.95 ± 0.56 | <0.001 | |
| Subtalar eversion | 0.64 ± 0.33 | 0.58 ± 0.25 | 0.02 | |
| Running | Hip flexion | 0.93 ± 0.22 | 0.88 ± 0.19 | 0.41 |
| Knee extension | 2.12 ± 0.44 | 1.74 ± 0.39 | <0.001 | |
| Ankle plantarflexion | 2.92 ± 0.33 | 3.23 ± 0.31 | 0.02 | |
| Subtalar eversion | 0.85 ± 0.25 | 0.62 ± 0.27 | <0.001 |
| Muscle forces (BW) | IS | US | p-Value | |
|---|---|---|---|---|
| Walking | Vastus medialis | 0.15 ± 0.04 | 0.19 ± 0.02 | <0.001 |
| Vastus lateralis | 0.29 ± 0.05 | 0.40 ± 0.02 | <0.001 | |
| Vastus intermedius | 0.17 ± 0.04 | 0.23 ± 0.03 | 0.01 | |
| Rectus femoris | 2.24 ± 0.33 | 2.27 ± 0.28 | 0.43 | |
| Jogging | Vastus medialis | 0.85 ± 0.12 | 0.68 ± 0.17 | <0.001 |
| Vastus lateralis | 1.76 ± 0.38 | 1.44 ± 0.45 | 0.01 | |
| Vastus intermedius | 1.15 ± 0.22 | 0.82 ± 0.16 | <0.001 | |
| Rectus femoris | 1.57 ± 0.19 | 2.23 ± 0.28 | <0.001 | |
| Running | Vastus medialis | 1.32 ± 0.11 | 1.05 ± 0.24 | <0.001 |
| Vastus lateralis | 2.08 ± 0.23 | 1.77 ± 0.41 | <0.001 | |
| Vastus intermedius | 1.38 ± 0.12 | 1.15 ± 0.33 | <0.001 | |
| Rectus femoris | 1.69 ± 0.24 | 1.58 ± 0.27 | 0.02 |
| Muscle forces (BW) | IS | US | p-Value | |
|---|---|---|---|---|
| Walking | Gastrocnemius medialis | 1.12 ± 0.43 | 1.26 ± 0.36 | 0.02 |
| Gastrocnemius lateralis | 0.28 ± 0.08 | 0.37 ± 0.03 | <0.001 | |
| Soleus | 2.12 ± 0.26 | 2.78 ± 0.31 | <0.001 | |
| Jogging | Gastrocnemius medialis | 1.51 ± 0.32 | 1.92 ± 0.46 | 0.01 |
| Gastrocnemius lateralis | 0.63 ± 0.23 | 0.84 ± 0.46 | <0.001 | |
| Soleus | 4.95 ± 0.44 | 4.88 ± 0.39 | 0.52 | |
| Running | Gastrocnemius medialis | 1.81 ± 0.32 | 2.02 ± 0.29 | 0.03 |
| Gastrocnemius lateralis | 0.86 ± 0.21 | 0.87 ± 0.18 | 0.94 | |
| Soleus | 5.15 ± 0.92 | 5.19 ± 0.76 | 0.23 |
| Joint reaction forces (BW) | IS | US | p-Value | |
|---|---|---|---|---|
| Walking | Hip | 5.92 ± 1.03 | 4.86 ± 1.11 | 0.01 |
| Knee | 4.67 ± 0.86 | 3.12 ±0.97 | <0.001 | |
| Ankle | 4.39 ± 0.94 | 5.81 ±1.21 | <0.001 | |
| Jogging | Hip | 8.22 ± 0.68 | 5.94 ±1.32 | <0.001 |
| Knee | 11.22 ± 2.33 | 6.85 ±1.78 | <0.001 | |
| Ankle | 10.62 ± 2.46 | 9.21 ± 3.85 | 0.04 | |
| Running | Hip | 7.94 ± 1.31 | 7.88 ± 2.44 | 0.36 |
| Knee | 8.05 ± 1.05 | 10.24 ± 1.97 | 0.01 | |
| Ankle | 10.54 ± 1.54 | 11.96 ± 1.32 | 0.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, D.; Fekete, G.; Baker, J.S.; Mei, Q.; István, B.; Zhang, Y.; Gu, Y. A Pilot Study of Musculoskeletal Abnormalities in Patients in Recovery from a Unilateral Rupture-Repaired Achilles Tendon. Int. J. Environ. Res. Public Health 2020, 17, 4642. https://doi.org/10.3390/ijerph17134642
Sun D, Fekete G, Baker JS, Mei Q, István B, Zhang Y, Gu Y. A Pilot Study of Musculoskeletal Abnormalities in Patients in Recovery from a Unilateral Rupture-Repaired Achilles Tendon. International Journal of Environmental Research and Public Health. 2020; 17(13):4642. https://doi.org/10.3390/ijerph17134642
Chicago/Turabian StyleSun, Dong, Gusztáv Fekete, Julien S. Baker, Qichang Mei, Bíró István, Yan Zhang, and Yaodong Gu. 2020. "A Pilot Study of Musculoskeletal Abnormalities in Patients in Recovery from a Unilateral Rupture-Repaired Achilles Tendon" International Journal of Environmental Research and Public Health 17, no. 13: 4642. https://doi.org/10.3390/ijerph17134642
APA StyleSun, D., Fekete, G., Baker, J. S., Mei, Q., István, B., Zhang, Y., & Gu, Y. (2020). A Pilot Study of Musculoskeletal Abnormalities in Patients in Recovery from a Unilateral Rupture-Repaired Achilles Tendon. International Journal of Environmental Research and Public Health, 17(13), 4642. https://doi.org/10.3390/ijerph17134642