The Effects of Cross-Legged Sitting on the Trunk and Pelvic Angles and Gluteal Pressure in People with and without Low Back Pain



Abstract
1. Introduction
2. Subjects and Methods
2.1. Participants
2.2. Protocol
2.3. Outcome Measurements
2.4. Data Analysis
3. Results
3.1. General Characteristics of Subjects
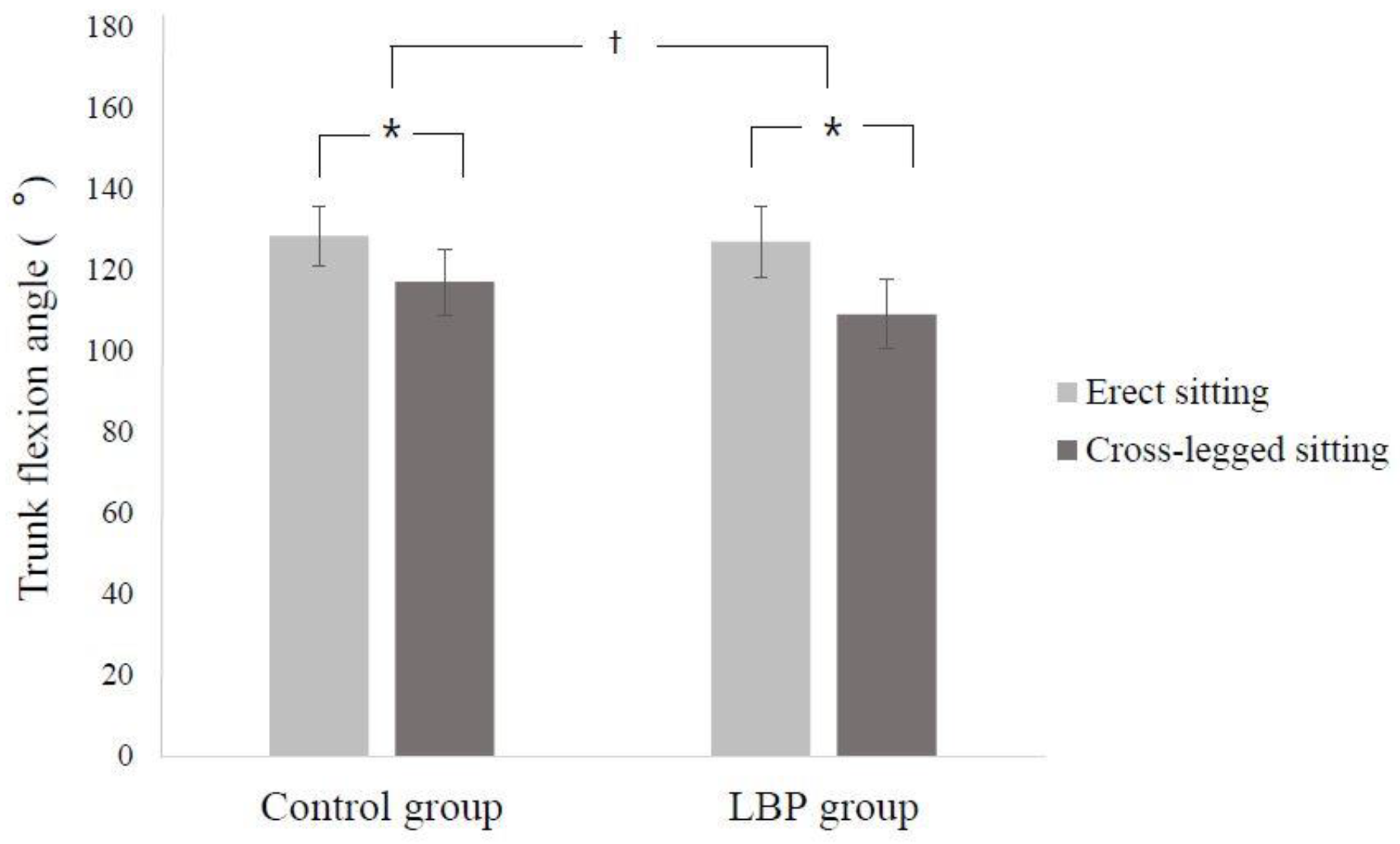
3.2. Comparison of Trunk Flexion Angle
3.3. Comparison of Pelvic Obliquity
3.4. Comparison of Peak Pressure Ratio
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef]
- Wilke, H.J.; Neef, P.; Caimi, M.; Hoogland, T.; Claes, L.E. New in vivo measurements of pressures in the intervertebral disc in daily life. Spine 1999, 24, 755–762. [Google Scholar] [CrossRef]
- Nachemson, A.; Morris, J.M. In Vivo Measurements of Intradiscal Pressure. Discometry, a Method for the Determination of Pressure in the Lower Lumbar Discs. J. Bone Joint Surg. 1964, 46, 1077–1092. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation; Mosby: St. Louis, MO, USA, 2002. [Google Scholar]
- Kwon, Y.R.; Kim, J.W.; Heo, J.H.; Jeon, H.M.; Choi, E.B.; Eom, G.M. The effect of sitting posture on the loads at cervico-thoracic and lumbosacral joints. Technol. Health Care 2018, 26, 409–418. [Google Scholar] [CrossRef]
- Edmondston, S.J.; Sharp, M.; Symes, A.; Alhabib, N.; Allison, G.T. Changes in mechanical load and extensor muscle activity in the cervico-thoracic spine induced by sitting posture modification. Ergonomics 2011, 54, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.W.; Wong, C.G.; Lau, E.T.; Tan, K.A.; Lau, L.L.; Liu, K.G.; Wong, H.K. Differences in erect sitting and natural sitting spinal alignment-insights into a new paradigm and implications in deformity correction. Spine J. 2017, 17, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Akkarakittichoke, N.; Janwantanakul, P. Seat Pressure Distribution Characteristics During 1 Hour Sitting in Office Workers with and Without Chronic Low Back Pain. Saf. Health Work 2017, 8, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Astfalck, R.G.; O’Sullivan, P.B.; Straker, L.M.; Smith, A.J.; Burnett, A.; Caneiro, J.P.; Dankaerts, W. Sitting postures and trunk muscle activity in adolescents with and without nonspecific chronic low back pain: An analysis based on subclassification. Spine 2010, 35, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Fann, A.V. The prevalence of postural asymmetry in people with and without chronic low back pain. Arch. Phys. Med. Rehabil. 2002, 83, 1736–1738. [Google Scholar] [CrossRef]
- Snijders, C.J.; Hermans, P.F.; Kleinrensink, G.J. Functional aspects of cross-legged sitting with special attention to piriformis muscle and sacroiliac joint. Clin. Biomech. 2006, 21, 116–121. [Google Scholar] [CrossRef]
- Snijders, C.J.; Slaqter, A.H.; Van Strik, R.; Vleeming, A.; Stoeckart, R.; Stam, H.J. Why leg crossing? The influence of common postures on Abdominal muscle activity. Spine 1995, 20, 1989–1993. [Google Scholar] [CrossRef] [PubMed]
- Schamberger, W. The Malalignment Syndrome: Implications for Medicine and Sport, 1st ed.; Churchill Livingstone: London, UK, 2002. [Google Scholar]
- Lee, J.H.; Park, S.Y.; Yoo, W.G. Changes in craniocervical and trunk flexion angles and gluteal pressure during VDT work with continuous cross-legged sitting. J. Occup. Health 2011, 53, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.S.; An, D.H. Differences in lumbar and pelvic angles and gluteal pressure in different sitting postures. J. Phys. Ther. Sci. 2015, 27, 1333–1335. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P.B.; Grahamslaw, K.M.; Kendell, M.; Lapenskie, S.C.; Möller, N.E.; Richards, K.V. The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine 2002, 27, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Egan, D.A.; Cole, J.; Twomey, L. An alternative method for the measurement of pelvic skeletal asymmetry and the association between asymmetry and back pain. In Three Dimensional Analysis of Spinal Deformities; D’Amico, M., Merolli, A., Santambrogio, G., Eds.; IOS Press: Washington, DC, USA, 1995; pp. 171–177. [Google Scholar]
- Michaud, S.B.; Gard, S.A.; Childress, D.S. A preliminary investigation of pelvic obliquity patterns during gait in persons with transtibial and transfemoral amputation. J. Rehabil. Res. Dev. 2000, 37, 1–10. [Google Scholar]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: A systematic review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef]
- Keegan, J.J. Alteration of the lumbar curve related to posture and seating. J. Bone Joint Surg. 1953, 35, 589–603. [Google Scholar] [CrossRef]
- Murphy, S.; Buckle, P.; Stubbs, D. Classroom posture and self-reported back and neck pain in schoolchildren. Appl. Ergon. 2004, 35, 113–120. [Google Scholar] [CrossRef]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L. Differences in sitting postures are associated with nonspecific chronic low back pain disorders when patients are subclassified. Spine 2006, 31, 698–704. [Google Scholar] [CrossRef]
- O’Sullivan, P.B.; Burnett, A.; Floyd, A.N.; Gadsdon, K.; Logiudice, J.; Miller, D.; Quirke, H. Lumbar repositioning deficit in a specific low back pain population. Spine 2003, 28, 1074–1079. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine: Ⅰ. Function, dysfunction, adaptation, and enhancement. J. Spinal Disord. 1992, 5, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Shirazi-Adl, A.; Drouin, G. Load-bearing role of facets in a lumbar segment under sagittal plane loadings. J. Biomech. 1987, 20, 601–613. [Google Scholar] [CrossRef]
- Dankaerts, W.; O’Sullivan, P.; Burnett, A.; Straker, L. Altered Patterns of Superficial Trunk Muscle Activation During Sitting in Nonspecific Chronic Low Back Pain Patients. Spine 2006, 31, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Chaléat-Valayer, E.; Mac-Thiong, J.M.; Paquet, J.; Berthonnaud, E.; Siani, F.; Roussouly, P. Sagittal spino-pelvic alignment in chronic low back pain. Eur. Spine J. 2011, 20, S634–S640. [Google Scholar] [CrossRef]
- Tsauo, J.Y.; Jang, Y.; Du, C.L.; Liang, H.W. Incidence and risk factors of neck discomfort: A 6-month sedentary-worker cohort study. J. Occup. Rehabil. 2007, 17, 171–179. [Google Scholar] [CrossRef]
- Deyo, R.A.; Dworkin, S.F.; Amtmann, D.; Andersson, G.; Borenstein, D.; Carragee, E.; Carrino, J.; Chou, R.; Cook, K.; Delitto, A.; et al. Focus article report of the NIH Task Force on Research Standards for Chronic Low Back Pain. Clin. Biomech. 2014, 30, 701–702. [Google Scholar]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sorensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Abboud, J.; Nougarou, F.; Page, I.; Cantin, V.; Massicotte, D.; Descarreaux, M. Trunk motor variability in patients with non-specific chronic low back pain. Eur. J. Appl. Physiol. 2014, 114, 2645–2654. [Google Scholar] [CrossRef]
- Falla, D.; Gizzi, L.; Tschapek, M.; Erlenwein, J.; Petzke, F. Reduced task-induced variations in the distribution of activity across back muscle regions in individuals with low back pain. Pain 2014, 155, 944–953. [Google Scholar] [CrossRef]
- Biering-Sørensen, F. Physical measurements as risk indicators for low back trouble over a one year period. Spine 1984, 9, 106–119. [Google Scholar] [CrossRef]
- Solomonow, M.; Hatipkarasulu, S.; Zhou, B.H.; Baratta, R.V.; Aghazadeh, F. Biomechanics and electro-myography of a common idiophatic low back disorder. Spine 2003, 28, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Solomonow, M.; Zhou, B.H.; Baratta, R.V.; Burger, E. Biomechanics and electromyography of a cumulative lumbar disorder: Response to static flexion. Clin. Biomech. 2003, 18, 890–898. [Google Scholar] [CrossRef]
- Lis, A.; Black, K.; Korn, H.; Nordin, M. Association between sitting and occupational LBP. Eur. Spine J. 2007, 16, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Pooriput, W.; Bala, S.R.; Prawit, J. Perceived body discomfort and trunk muscle activity in three prolonged sitting postures. J. Phys. Ther. Sci. 2015, 27, 2183–2187. [Google Scholar]
- Waongenngarm, P.; Areerak, K.; Janwantanakul, P. The effects of breaks on low back pain, discomfort, and work productivity in office workers: A systematic review of randomized and non-randomized controlled trials. Appl. Ergon. 2018, 68, 230–239. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | LBP Group (n = 30) | Control Group (n = 30) | p |
|---|---|---|---|
| Sex (Male/Female) | 22/8 | 20/10 | 0.779 b |
| Age (years) | 24.43 ± 2.73 a | 24.17 ± 2.77 | 0.708 c |
| Height (cm) | 170.47 ± 7.53 | 171.37 ± 9.19 | 0.684 c |
| Weight (kg) | 65.50 ± 12.79 | 66.90 ± 10.80 | 0.649 c |
| NPRS | 4.90 ± 0.96 | 0.0 ± 0.0 | |
| Postures that make symptoms worse (lumbar flexion/extension) | (27/3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, K.-s.; Jung, J.-h.; In, T.-s. The Effects of Cross-Legged Sitting on the Trunk and Pelvic Angles and Gluteal Pressure in People with and without Low Back Pain. Int. J. Environ. Res. Public Health 2020, 17, 4621. https://doi.org/10.3390/ijerph17134621
Jung K-s, Jung J-h, In T-s. The Effects of Cross-Legged Sitting on the Trunk and Pelvic Angles and Gluteal Pressure in People with and without Low Back Pain. International Journal of Environmental Research and Public Health. 2020; 17(13):4621. https://doi.org/10.3390/ijerph17134621
Chicago/Turabian StyleJung, Kyoung-sim, Jin-hwa Jung, and Tae-sung In. 2020. "The Effects of Cross-Legged Sitting on the Trunk and Pelvic Angles and Gluteal Pressure in People with and without Low Back Pain" International Journal of Environmental Research and Public Health 17, no. 13: 4621. https://doi.org/10.3390/ijerph17134621
APA StyleJung, K.-s., Jung, J.-h., & In, T.-s. (2020). The Effects of Cross-Legged Sitting on the Trunk and Pelvic Angles and Gluteal Pressure in People with and without Low Back Pain. International Journal of Environmental Research and Public Health, 17(13), 4621. https://doi.org/10.3390/ijerph17134621