The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study

 ,
, 
 , , ,
, , ,  , ,
, ,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Sample
2.2. Demographic Characteristics, OPA and ST
- How many hours do you usually spend sitting per day? The question covered any activity in which the person had to be sitting (i.e., watching television, reading, sewing, etc.) and it referred to the present time. The question was answered by 610 participants at both baseline and follow-up.Hours sitting per day were used to classify subjects into non-sedentary (<4 h/day) and sedentary (≥4 h/day). The cut-off points to define this sedentary behavior (SB) are based on receiver operating characteristic curves carried out with the same sample and reported in a previous study [20].According to the answer to the first question, participants were divided into two groups:
- NON-SEDENTARY: A group of participants who had never been sedentary or had showed a positive change (passing from sedentary at baseline to non-sedentary in the follow-up).
- SEDENTARY: A group of participants who were sedentary in both evaluations or showed a negative change (were non-sedentary at baseline but were in the follow-up).
- 2.
- Are you currently engaged in organized physical activity? The question covered any organized physical activity understood as a collective guided and supervised activity that was developed by an instructor. All participants that answered YES at baseline were included in the study (642 participants).According to the answers to the OPA question, participants were classified as:
- ALWAYS OPA: Performed OPA at both baseline and follow-up.
- STOPPED OPA: Performed OPA at baseline but not at follow-up.
- OPA-ACTIVE: Performed OPA longitudinally and were never sedentary or stopped being sedentary (223 females and 62 males).
- OPA-SEDENTARY: Performed OPA longitudinally and were always sedentary or started being sedentary (160 females and 45 males).
- SEDENTARY-INACTIVE: Stopped performing OPA and were always sedentary or started being sedentary (60 females and 16 males).
- NON-SEDENTARY-INACTIVE: Were not sedentary longitudinally or stopped being sedentary and stopped engaging in OPA (34 females and 10 males).
2.3. Fitness Tests
- -
- Anthropometry: body weight, height and body mass index (BMI)
- -
- One leg balance test: to evaluate static balance.
- -
- Thirty-second chair stand test: to evaluate lower extremities strength.
- -
- Arm curl test: to evaluate upper extremities strength.
- -
- Chair sit-and-reach test: to evaluate lower extremities flexibility.
- -
- Back scratch test: to evaluate upper extremities flexibility.
- -
- Eight-Foot up-and-go test: to evaluate agility.
- -
- Brisk walking test: to evaluate walking speed.
- -
- Six-Minute walk test (6MWT): to assess endurance capacity.
2.4. Statistical Analyses
3. Results
3.1. Retention Rates and Differences between Samples
3.2. Descriptive Characteristics
3.3. Physical Fitness
3.3.1. Physical Fitness Changes during the 8-Year Period Stratifying by Sex
3.3.2. Physical Fitness Changes during the 8-Year Period Stratifying by Sex According to Age Group
Males
Females
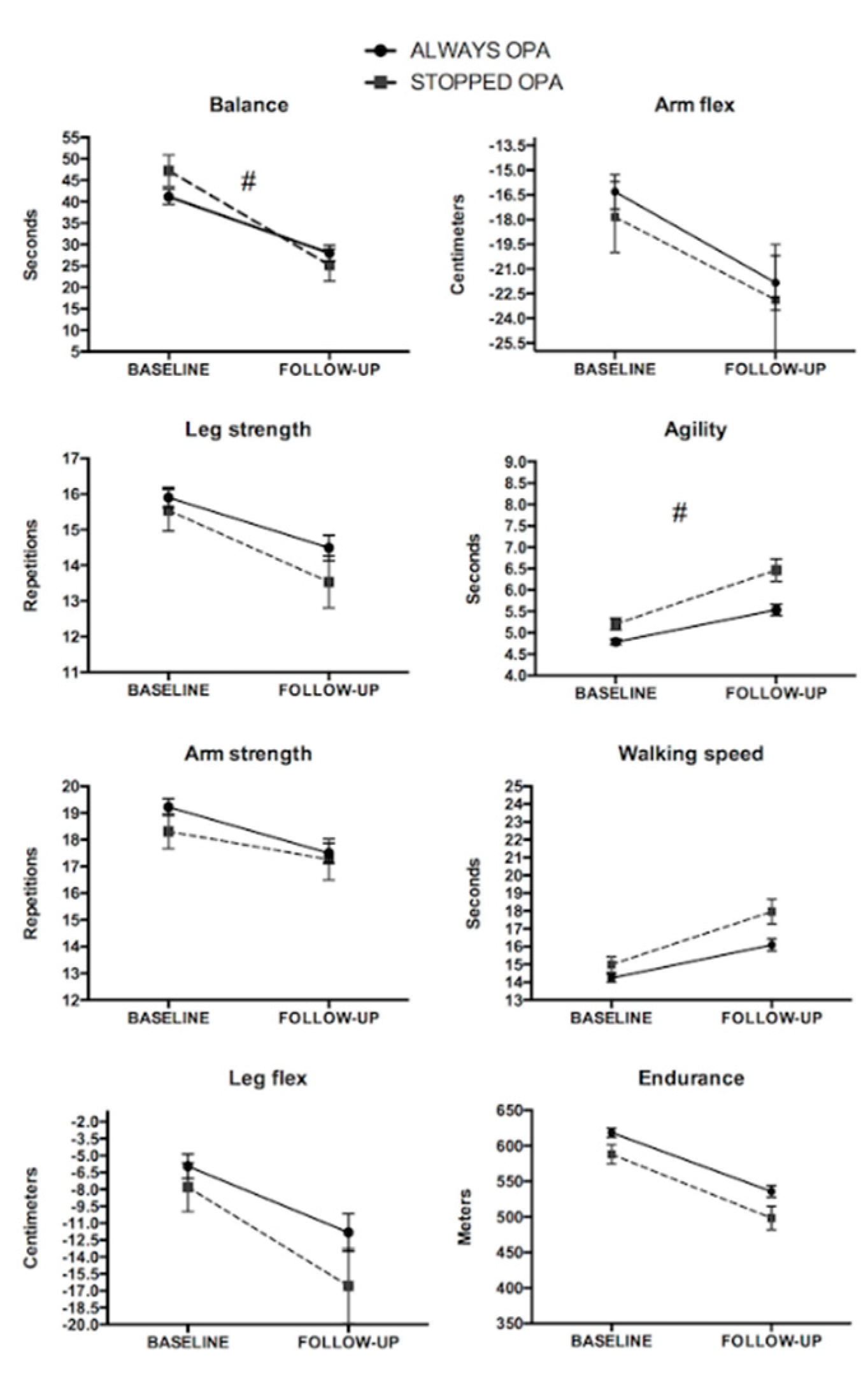
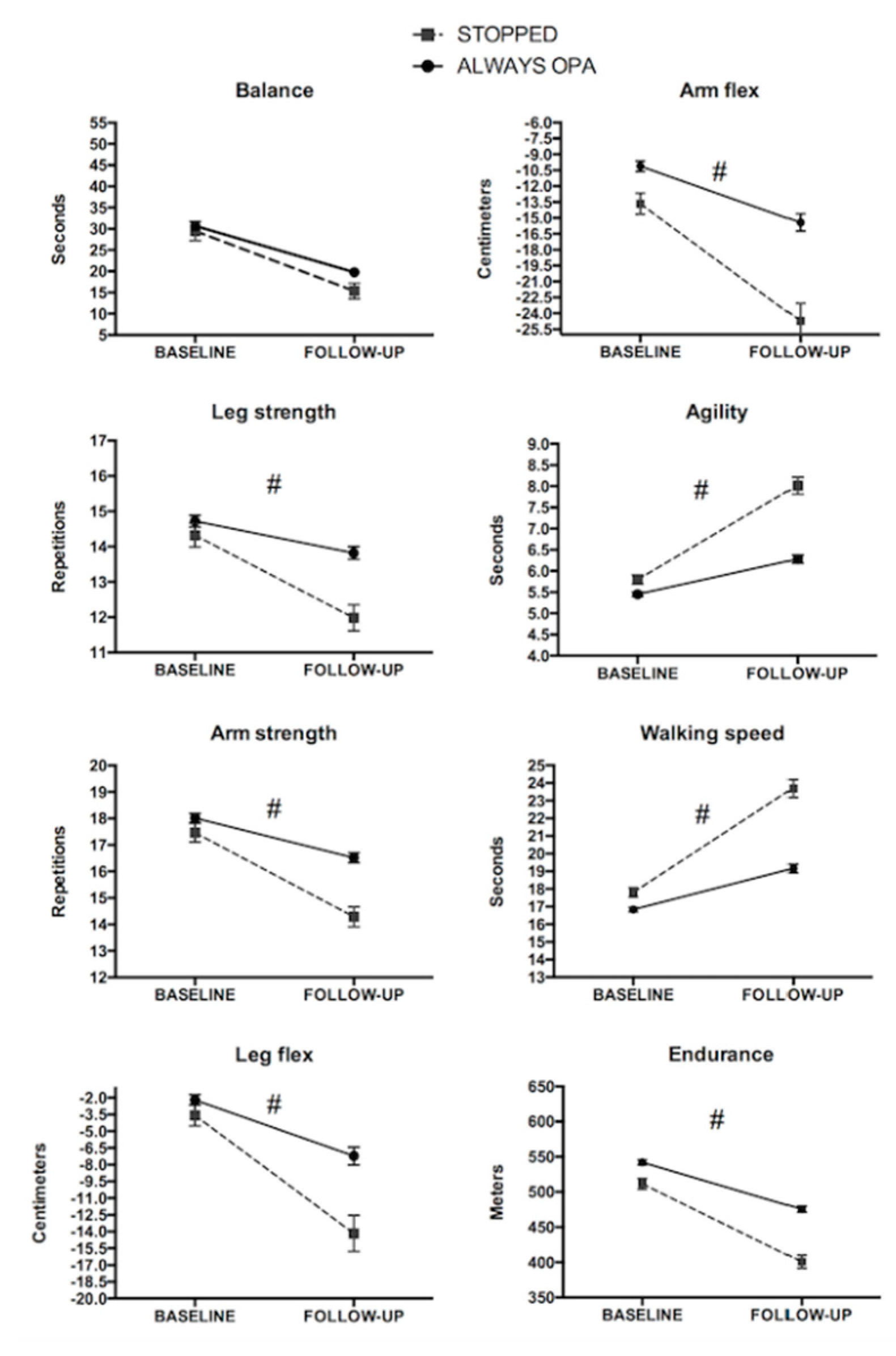
3.3.3. Physical Fitness Changes Stratifying by Sex According to Change in Organized Physical Activity
Males
Females
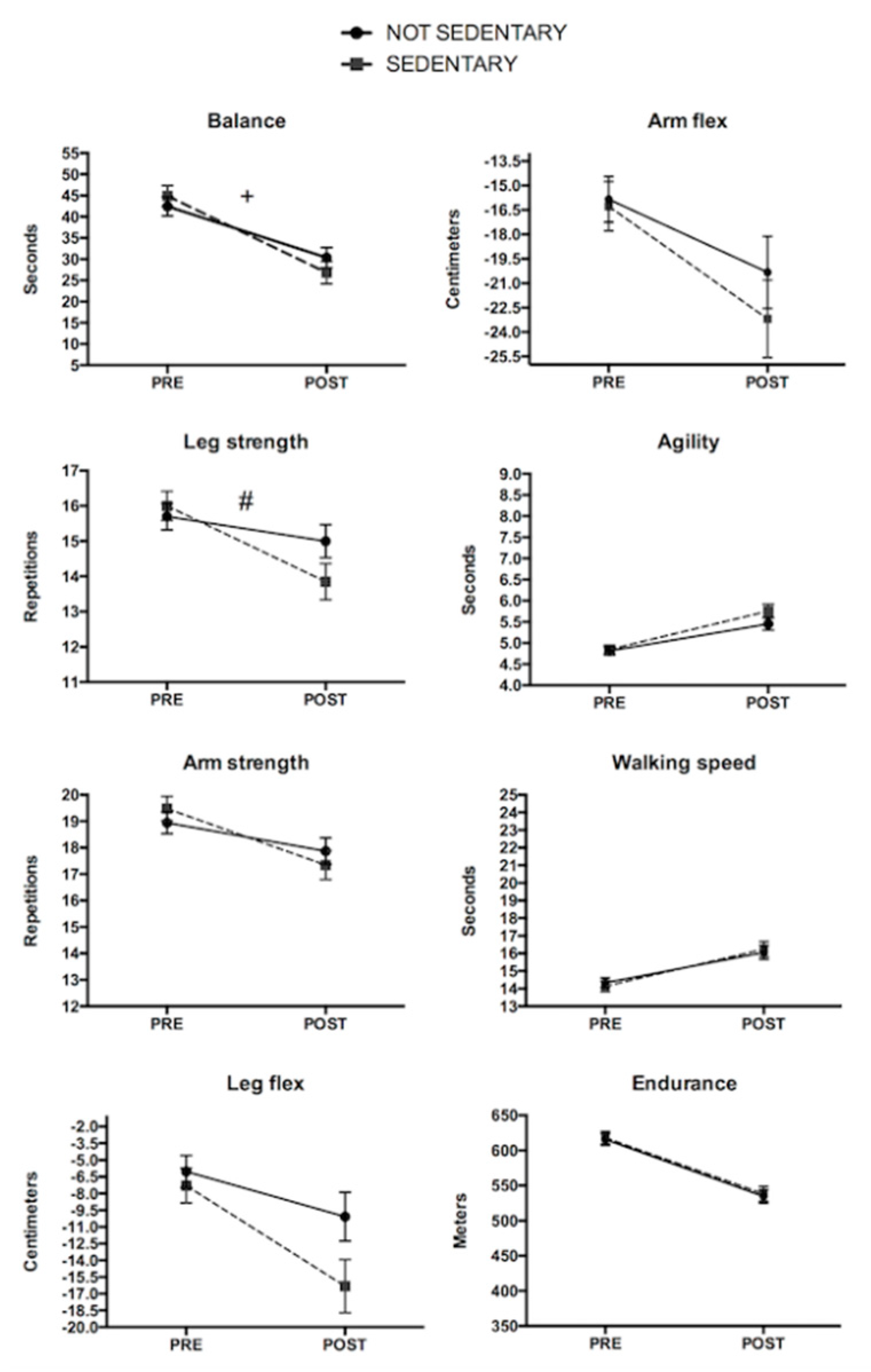
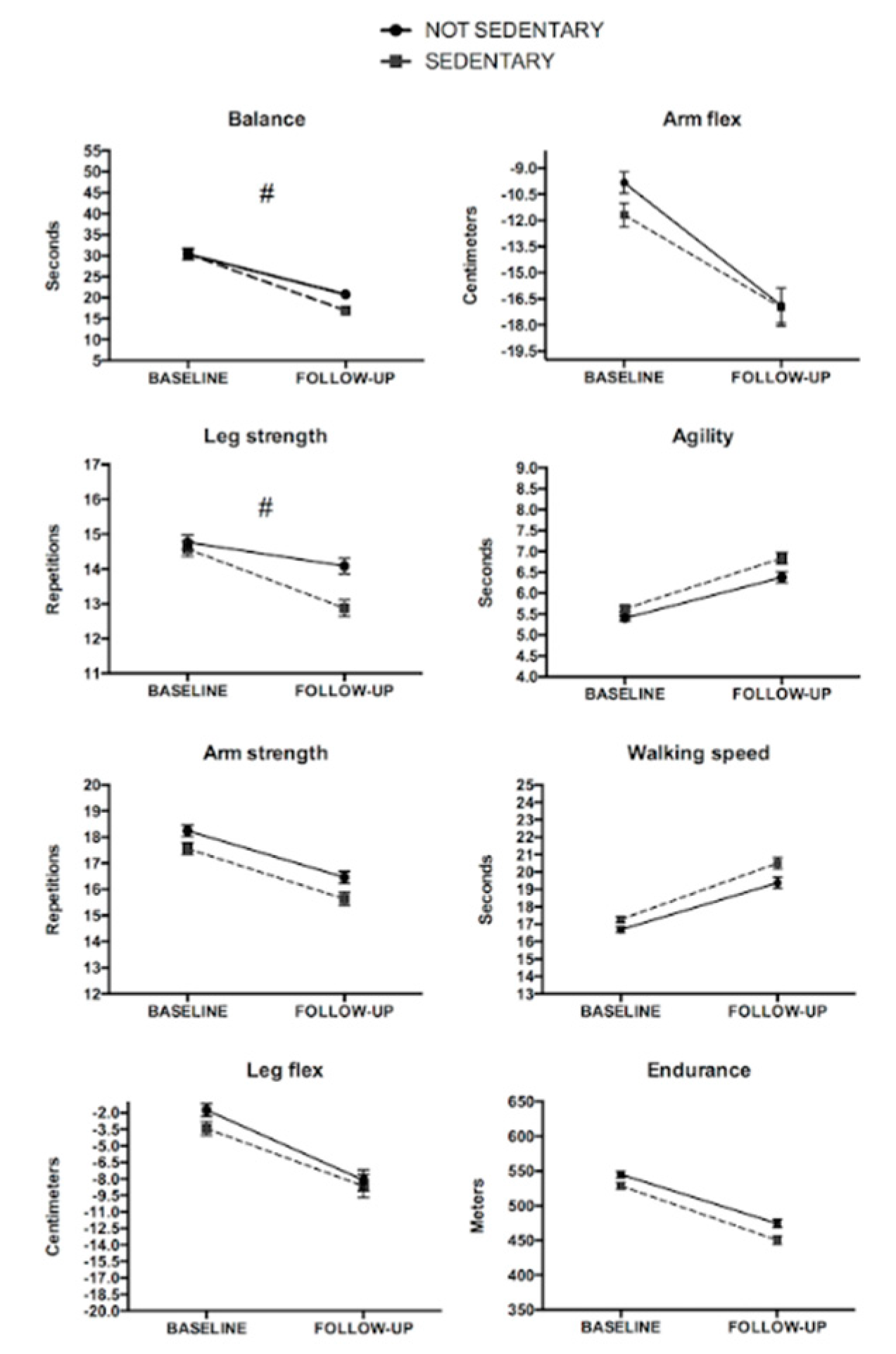
3.3.4. Physical Fitness Changes Stratifying by Sex According to Sitting Time
Males
Females
3.3.5. Physical Fitness Changes Stratifying by Sex According to Change in Organized Physical Activity and Sedentary Behaviors.
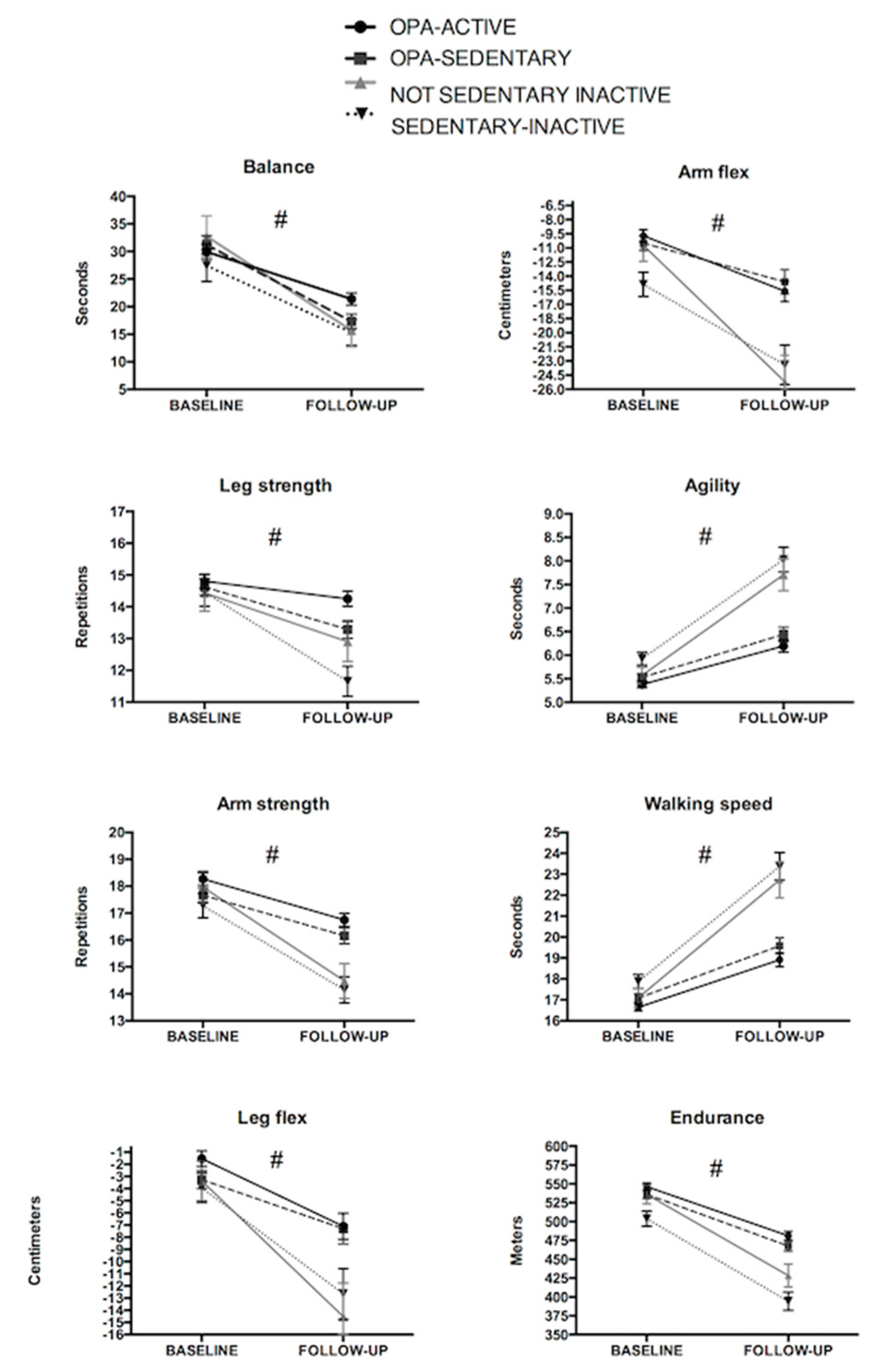
Females
OPA-ACTIVE vs. OPA-SEDENTARY
OPA-ACTIVE vs. NON-SEDENTARY INACTIVE
OPA-ACTIVE vs. SEDENTARY-INACTIVE
OPA-SEDENTARY vs. NON-SEDENTARY INACTIVE
OPA-SEDENTARY vs. SEDENTARY-INACTIVE
NON-SEDENTARY INACTIVE vs. SEDENTARY-INACTIVE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Glisky, E.L. Changes in Cognitive Function in Human Aging; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2007; ISBN 0849338182. [Google Scholar]
- Brady, A.O.; Straight, C.R.; Evans, E.M. Body composition, muscle capacity, and physical function in older adults: An integrated conceptual model. J. Aging Phys. Act. 2014, 22, 441–452. [Google Scholar] [CrossRef]
- Paterson, D.H.; Govindasamy, D.; Vidmar, M.; Cunningham, D.A.; Koval, J.J. Longitudinal Study of Determinants of Dependence in an Elderly Population. J. Am. Geriatr. Soc. 2004, 52, 1632–1638. [Google Scholar] [CrossRef]
- Reid, K.F.; Fielding, R.A. Skeletal muscle power: A critical determinant of physical functioning in older adults. Exerc. Sport Sci. Rev. 2012, 40, 4–12. [Google Scholar] [CrossRef]
- Myers, J.; Doom, R.; King, R.; Fonda, H.; Chan, K.; Kokkinos, P.; Rehkopf, D.H. Association Between Cardiorespiratory Fitness and Health Care Costs: The Veterans Exercise Testing Study. Mayo Clin. Proc. 2018, 93, 48–55. [Google Scholar] [CrossRef]
- Laukkanen, J.A.; Mäkikallio, T.H.; Rauramaa, R.; Kiviniemi, V.; Ronkainen, K.; Kurl, S. Cardiorespiratory Fitness Is Related to the Risk of Sudden Cardiac Death. J. Am. Coll. Cardiol. 2010, 56, 1476–1483. [Google Scholar] [CrossRef]
- Pijnappels, M.; van der Burg, (Petra) J.C.E.; Reeves, N.D.; van Dieën, J.H. Identification of elderly fallers by muscle strength measures. Eur. J. Appl. Physiol. 2008, 102, 585–592. [Google Scholar] [CrossRef]
- Waller, B.; Ogonowska-Słodownik, A.; Vitor, M.; Rodionova, K.; Lambeck, J.; Heinonen, A.; Daly, D. The effect of aquatic exercise on physical functioning in the older adult: A systematic review with meta-analysis. Age Ageing 2016, 45, 594–602. [Google Scholar] [CrossRef]
- Guizelini, P.C.; de Aguiar, R.A.; Denadai, B.S.; Caputo, F.; Greco, C.C. Effect of resistance training on muscle strength and rate of force development in healthy older adults: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 51–58. [Google Scholar] [CrossRef]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef]
- Bouaziz, W.; Lang, P.O.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- Daskalopoulou, C.; Stubbs, B.; Kralj, C.; Koukounari, A.; Prince, M.; Prina, A.M. Physical activity and healthy ageing: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 2017, 38, 6–17. [Google Scholar] [CrossRef]
- Lazarus, N.R.; Harridge, S.D.R. Exercise, physiological function, and the selection of participants for aging research. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65 A, 854–857. [Google Scholar] [CrossRef]
- Sagarra-Romero, L.; Vicente-Rodríguez, G.; Pedrero-Chamizo, R.; Vila-Maldonado, S.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; González-Gross, M.; Casajús, J.A.; Ara, I.; et al. Is Sitting Time Related with Physical Fitness in Spanish Elderly Population? The Exernet Multicenter Study. J. Nutr. Heal. Aging 2019, 23, 401–407. [Google Scholar] [CrossRef]
- Mañas, A.; del Pozo-Cruz, B.; García-García, F.J.; Guadalupe-Grau, A.; Ara, I. Role of objectively measured sedentary behaviour in physical performance, frailty and mortality among older adults: A short systematic review. Eur. J. Sport Sci. 2017, 17, 940–953. [Google Scholar] [CrossRef]
- Gomez-Cabello, A.; Pedrero-Chamizo, R.; Olivares, P.R.; Luzardo, L.; Juez-Bengoechea, A.; Mata, E.; Albers, U.; Aznar, S.; Villa, G.; Espino, L.; et al. Prevalence of overweight and obesity in non-institutionalized people aged 65 or over from Spain: The elderly EXERNET multi-centre study. Obes. Rev. 2011, 12, 583–592. [Google Scholar] [CrossRef]
- Rezende, L.F.M.; Sá, T.H.; Mielke, G.I.; Viscondi, J.Y.K.; Rey-López, J.P.; Garcia, L.M.T. All-Cause Mortality Attributable to Sitting Time. Am. J. Prev. Med. 2016, 51, 253–263. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects (revised October 7, 2000). HIV Clin. Trials 2001, 2, 92–95. [CrossRef]
- López-Rodríguez, C.; Laguna, M.; Gómez-Cabello, A.; Gusi, N.; Espino, L.; Villa, G.; Pedrero-Chamizo, R.; Casajus, J.A.; Ara, I.; Aznar, S. Validation of the self-report EXERNET questionnaire for measuring physical activity and sedentary behavior in elderly. Arch. Gerontol. Geriatr. 2017, 69, 156–161. [Google Scholar] [CrossRef]
- Gómez-Cabello, A.; Pedrero-Chamizo, R.; Olivares, P.R.; Hernández-Perera, R.; Rodríguez-Marroyo, J.A.; Mata, E.; Aznar, S.; Villa, J.G.; Espino-Torón, L.; Gusi, N.; et al. Sitting time increases the overweight and obesity risk independently of walking time in elderly people from Spain. Maturitas 2012, 73, 337–343. [Google Scholar] [CrossRef]
- Pedrero-Chamizo, R.; Gómez-Cabello, A.; Delgado, S.; Rodríguez-Llarena, S.; Rodríguez-Marroyo, J.A.; Cabanillas, E.; Meléndez, A.; Vicente-Rodríguez, G.; Aznar, S.; Villa, G.; et al. Physical fitness levels among independent non-institutionalized Spanish elderly: The elderly EXERNET multi-center study. Arch. Gerontol. Geriatr. 2012, 55, 406–416. [Google Scholar] [CrossRef]
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. Assumption in large public health datasets. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Cohen, D. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum, Ed.; Lawrence Erlbaum Associates Publishers: Hillsdale, MI, USA, 1988. [Google Scholar]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef]
- Tuna, H.D.; Edeer, A.O.; Malkoc, M.; Aksakoglu, G. Effect of age and physical activity level on functional fitness in older adults. Eur. Rev. Aging Phys. Act. 2009, 6, 99–106. [Google Scholar] [CrossRef]
- Kim, K.M.; Lim, S.; Oh, T.J.; Moon, J.H.; Choi, S.H.; Lim, J.Y.; Kim, K.W.; Park, K.S.; Jang, H.C. Longitudinal Changes in Muscle Mass and Strength, and Bone Mass in Older Adults: Gender-Specific Associations Between Muscle and Bone Losses. J. Gerontol. Ser. A 2018, 73, 1062–1069. [Google Scholar] [CrossRef]
- Pereira, C.; Baptista, F.; Cruz-Ferreira, A. Role of physical activity, physical fitness, and chronic health conditions on the physical independence of community-dwelling older adults over a 5-year period. Arch. Gerontol. Geriatr. 2016, 65, 45–53. [Google Scholar] [CrossRef]
- Vermeulen, J.; Neyens, J.C.; van Rossum, E.; Spreeuwenberg, M.D.; de Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef]
- Vianna, L.C.; Oliveira, R.B.; Araújo, C.G.S. Age-Related Decline in Handgrip Strength Differs According to Gender. J. Strength Cond. Res. 2007, 21, 1310. [Google Scholar] [CrossRef]
- Samson, M. Relationships between physical performance measures, age, height and body weight in healthy adults. Age Ageing 2000, 29, 235–242. [Google Scholar] [CrossRef]
- Essen-gustavsson, B.; Borges, O. Histochemical and metabolic characteristics of human skeletal muscle in relation to age. Acta Physiol. Scand. 1986, 126, 107–114. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Servicios Sociales e Igualdad. Informe Encuesta Europea de Salud 2014. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/EncuestaEuropea/pdf/EESE14_inf.pdf (accessed on 15 June 2020).
- Puszczalowska-Lizis, E.; Bujas, P.; Jandzis, S.; Omorczyk, J.; Zak, M. Inter-gender differences of balance indicators in persons 60–90 years of age. Clin. Interv. Aging 2018, 13, 903–912. [Google Scholar] [CrossRef]
- Gómez-Cabello, A.; Carnicero, J.A.; Alonso-Bouzón, C.; Tresguerres, J.Á.; Alfaro-Acha, A.; Ara, I.; Rodriguez-Mañas, L.; García-García, F.J. Age and gender, two key factors in the associations between physical activity and strength during the ageing process. Maturitas 2014, 78, 106–112. [Google Scholar] [CrossRef]
- Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Relationship between customary physical activity, muscle strength and physical performance in older men and women: findings from the Hertfordshire Cohort Study. Age Ageing 2008, 37, 589–593. [Google Scholar] [CrossRef]
- Bassey, E.J.; Bendall, M.J.; Pearson, M. Muscle strength in the triceps surae and objectively measured customary walking activity in men and women over 65 years of age. Clin. Sci. 1988, 74, 85–89. [Google Scholar] [CrossRef]
- Ku, P.W.; Fox, K.R.; Chen, L.J. Leisure-time physical activity, sedentary behaviors and subjective well-being in older adults: an eight-year longitudinal research. Soc. Indic. Res. 2016, 127, 1349–1361. [Google Scholar] [CrossRef]
- Harvey, J.A.; Chastin, S.F.M.; Skelton, D.A. How Sedentary Are Older People? A Systematic Review of the Amount of Sedentary Behavior. J. Aging Phys. Act. 2015, 23, 471–487. [Google Scholar] [CrossRef]
- Sen, A.; Gider, P.; Cavalieri, M.; Freudenberger, P.; Farzi, A.; Schallert, M.; Reichmann, F.; Watzinger, N.; Zweiker, R.; Schmidt, R.; et al. Association of cardiorespiratory fitness and morphological brain changes in the elderly: results of the austrian stroke prevention study. Neurodegener. Dis. 2012, 10, 135–137. [Google Scholar] [CrossRef]
- Bhamra, S.; Tinker, A.; Mein, G.; Ashcroft, R.; Askham, J. The retention of older people in longitudinal studies: A review of the literature. Qual. Ageing 2008, 9, 27–35. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Dawson Hughes, B.; Scott, D.; Sanders, K.M.; Rizzoli, R. Nutritional strategies for maintaining muscle mass and strength from middle age to later life: A narrative review. Maturitas 2020, 132, 57–64. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Males | Females | |||||
|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p Value | Baseline | Follow-Up | p Value | ||
| Anthropometric characteristics | |||||||
| Age (years) | 70.3 ± 4.3 | 77.8 ± 4.6 | <0.001 | 70.7 ± 4.4 | 78.3 ± 4.7 | <0.001 | |
| Weight (kg) | 78.3 ± 9.5 | 77.7 ± 9.8 | 0.920 | 67.5 ± 10.0 | 66.5 ± 10.7 | <0.001 | |
| Height (cm) | 165.6 ± 3.1 | 164.6 ± 5.9 | <0.001 | 152.5 ± 5.8 | 151.5 ± 5.9 | <0.001 | |
| BMI (kg/m2) | 28.6 ± 3.1 | 28.6 ± 3.2 | 0.967 | 29.0 ± 4.0 | 29.0 ± 4.3 | 0.811 | |
| Physical activity and sedentarism | |||||||
| OPA | yes (%) | 147 (100%) | 118 (80.3%) | 495 (100%) | 397 (80.2%) | ||
| no (%) | 0 (0%) | 29 (19.7%) | 0 (0%) | 98 (19.8%) | |||
| Daily sitting time | <1 h | 1 (0.8%) | 1 (0.8%) | 0.426 | 10 (2.1%) | 2 (0.4%) | <0.001 |
| 1–2 h | 12 (9.0%) | 9 (6.8%) | 54 (11.3%) | 47 (9.9%) | |||
| 2–3 h | 42 (31.6%) | 31 (23.3%) | 147 (30.8%) | 100 (21.0%) | |||
| 3–4 h | 40 (30.1%) | 31 (23.3%) | 125 (26.2%) | 108 (22.6%) | |||
| 4–5 h | 19 (14.3%) | 33 (24.8%) | 76 (15.9%) | 109 (22.9) | |||
| >5 h | 19 (14.3%) | 28 (21.1%) | 65 (13.6%) | 111 (23.3%) | |||
| Daily walking time | <1 h | 35 (24.5%) | 27 (18.9%) | 0.032 | 166 (33.9%) | 198 (40.5%) | <0.001 |
| 1–2 h | 75 (52.4%) | 74 (51.7%) | 244 (49.9%) | 222 (45.4%) | |||
| 2–3 h | 27 (18.9%) | 29 (20.3%) | 68 (13.9%) | 40 (8.2%) | |||
| 3–4 h | 3 (2.1%) | 9 (6.3%) | 7 (1.4%) | 14 (2.9%) | |||
| 4–5 h | 3 (2.1%) | 3 (2.1%) | 2 (0.4%) | 7 (1.4%) | |||
| >5 h | - | 1 (0.7%) | 2 (0.4%) | 8 (1.6%) | |||
| Sedentary | Yes | 38 (28.6%) | 61 (45.9%) | 0.011 | 141 (29.6%) | 220 (46.1%) | <0.001 |
| No | 95 (71.4%) | 72 (54.1%) | 336 (70.4%) | 257(53.9%) | |||
| Variables | Males | Females | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-up | ηp2 | Baseline | Follow-up | ηp2 | |
| Balance (Seconds) | 42.3 ± 20.4 | 27.5 ± 22.2 | 0.400 * | 30.5 ± 20.9 | 19.0 ± 17.6 | 0.269 * |
| Leg strength (repetitions) | 15.8 ± 2.3 | 14.3 ± 3.9 | 0.144 * | 14.7 ± 3.2 | 13.5 ± 3.6 | 0.099 * |
| Arm strength (repetitions) | 19.0 ± 3.8 | 17.5 ± 4.2 | 0.139 * | 17.9 ± 3.4 | 16.1 ± 3.9 | 0.182 * |
| Leg flexibility (centimetres) | −6.3 ± 11.7 | −12.8 ± 17.8 | 0.147 * | −2.5 ± 9.4 | −8.6 ± 16.0 | 0.137 * |
| Arm flexibility (centimetres) | −16.6 ± 11.4 | −22.0 ± 17.8 | 0.107 * | −10.8 ± 9.9 | −17.3 ± 16.6 | 0.161 * |
| Agility (seconds) | 4.9 ± 0.8 | 5.7 ± 1.6 | 0.307 * | 5.5 ± 1.0 | 6.6 ± 2.2 | 0.264 * |
| Walking speed (seconds) | 14.4 ± 2.3 | 16.5 ± 4.1 | 0.307 * | 17.0 ± 2.6 | 20.0 ± 5.3 | 0.326 * |
| Endurance (meters) | 612.6 ± 74.1 | 528.6 ± 98.9 | 0.516 * | 536.6 ± 72.1 | 462.1 ± 93.1 | 0.469 * |
| Title | Males | Within | GxT | Females | Within | GxT | |||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-up | ηp2 | p | Baseline | Follow-up | ηp2 | p | ||
| Balance (seconds) | 65–70y | 49.5 ± 17.8 | 37.8 ± 2.8 | 0.184 * | 0.045 | 35.2 ± 21.1 | 25.4 ± 20.0 | 0.110 * | 0.211 |
| 70–75y | 34.4 ± 21.0 | 17.8 ± 18.9 | 0.206 * | 28.7 ± 20.2 | 15.4 ± 13.2 | 0.144 * | |||
| >75y | 34.2 ± 19.6 | 12.3 ± 15.0 | 0.205* | 22.7 ± 18.8 | 10.5 ± 12.4 | 0.077 * | |||
| Leg strength (repetitions) | 65–70y | 16.1 ± 2.9 | 15.2 ± 3.6 | 0.032 * | 0.117 | 14.8 ± 3.0 | 14.0 ± 3.4 | 0.024 * | 0.008 |
| 70–75y | 15.8 ± 2.9 | 13.5 ± 4.0 | 0.108 * | 14.5 ± 3.3 | 13.4 ± 3.6 | 0.030 * | |||
| >75y | 15.2 ± 3.3 | 13.3 ± 4.1 | 0.048 * | 14.6 ± 3.4 | 12.4 ± 3.8 | 0.072 * | |||
| Arm strength (repetitions) | 65–70y | 19.6 ± 3.5 | 18.2 ± 3.6 | 0.062 * | 0.833 | 18.5 ± 3.5 | 17.0 ± 3.7 | 0.059 * | <0.001 |
| 70–75y | 18.9 ± 3.0 | 17.1 ± 5.1 | 0.058 * | 17.6 ± 3.5 | 16.0 ± 3.9 | 0.054 * | |||
| >75y | 17.5 ± 4.0 | 15.7 ± 3.4 | 0.035 * | 17.3 ± 2.9 | 14.3 ± 3.5 | 0.121 * | |||
| Leg flexibility (centimetres) | 65–70y | −5.8 ± 12.3 | −12.9 ± 20.0 | 0.102 * | 0.822 | −1.8 ± 8.9 | −8.6 ± 17.6 | 0.080 * | 0.600 |
| 70–75y | −5.5 ± 10.7 | −10.7 ± 12.9 | 0.028 * | −2.0 ± 9.9 | −7.2 ± 14.0 | 0.037 * | |||
| >75y | −8.9 ± 11.2 | −15.4 ± 17.2 | 0.032 * | −4.6 ± 8.9 | −10.8 ± 15.5 | 0.035 * | |||
| Arm flexibility (centimetres) | 65–70y | −15.6 ± 10.7 | −22.2 ± 20.9 | 0.088 * | 0.224 | −9.6 ± 8.9 | −16.1 ± 17.8 | 0.081 * | 0.902 |
| 70–75y | −16.8 ± 11.9 | −18.7 ± 13.4 | 0.004 | −10.8 ± 9.7 | −16.9 ± 15.3 | 0.055 * | |||
| >75y | −19.2 ± 12.7 | −26.8 ± 12.5 | 0.041 * | −13.4 ± 11.9 | −20.3 ± 15.7 | 0.044 * | |||
| Agility (seconds) | 65–70y | 4.7 ± 0.7 | 5.2 ± 0.8 | 0.078 * | <0.001 | 5.3 ± 0.9 | 6.0 ± 1.4 | 0.062 * | <0.001 |
| 70–75y | 4.9 ± 0.7 | 6.0 ± 1.8 | 0.194 * | 5.6 ± 1.1 | 6.6 ± 2.0 | 0.102 * | |||
| >75y | 5.3 ± 0.9 | 6.7 ± 2.1 | 0.215 * | 5.8 ± 1.0 | 7.9 ± 3.0 | 0.239 * | |||
| Walking speed (seconds) | 65–70y | 13.9 ± 2.1 | 15.1 ± 2.5 | 0.082 * | <0.001 | 16.4 ± 2.2 | 18.7 ± 4.0 | 0.114 * | <0.001 |
| 70–75y | 14.7 ± 2.4 | 17.1 ± 4.7 | 0.168 * | 17.2 ± 2.5 | 20.0 ± 1.1 | 0.134 * | |||
| >75y | 15.4 ± 2.5 | 19.4 ± 4.8 | 0.258 * | 18.0 ± 3.2 | 22.9 ± 7.9 | 0.224 * | |||
| Endurance (seconds) | 65–70y | 635.1 ± 64.2 | 566.1 ± 70.1 | 0.288 * | 0.005 | 549.0 ± 72.2 | 483.6 ± 86.1 | 0.237 * | 0.014 |
| 70–75y | 594.0 ± 74.7 | 511.9 ± 98.1 | 0.241 * | 536.5 ± 68.5 | 461.8 ± 82.6 | 0.238 * | |||
| >75y | 579.2 ± 80.9 | 450.6 ± 117.6 | 0.337 * | 509.8 ± 71.4 | 415.6 ± 107.4 | 0.228 * | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomez-Bruton, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Vila-Maldonado, S.; Gesteiro, E.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; et al. The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 4312. https://doi.org/10.3390/ijerph17124312
Gomez-Bruton A, Navarrete-Villanueva D, Pérez-Gómez J, Vila-Maldonado S, Gesteiro E, Gusi N, Villa-Vicente JG, Espino L, Gonzalez-Gross M, Casajus JA, et al. The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4312. https://doi.org/10.3390/ijerph17124312
Chicago/Turabian StyleGomez-Bruton, Alejandro, David Navarrete-Villanueva, Jorge Pérez-Gómez, Sara Vila-Maldonado, Eva Gesteiro, Narcis Gusi, Jose Gerardo Villa-Vicente, Luis Espino, Marcela Gonzalez-Gross, Jose A. Casajus, and et al. 2020. "The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study" International Journal of Environmental Research and Public Health 17, no. 12: 4312. https://doi.org/10.3390/ijerph17124312
APA StyleGomez-Bruton, A., Navarrete-Villanueva, D., Pérez-Gómez, J., Vila-Maldonado, S., Gesteiro, E., Gusi, N., Villa-Vicente, J. G., Espino, L., Gonzalez-Gross, M., Casajus, J. A., Ara, I., Gomez-Cabello, A., & Vicente-Rodríguez, G. (2020). The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. International Journal of Environmental Research and Public Health, 17(12), 4312. https://doi.org/10.3390/ijerph17124312