Nature Prescriptions for Health: A Review of Evidence and Research Opportunities


Abstract
1. Introduction
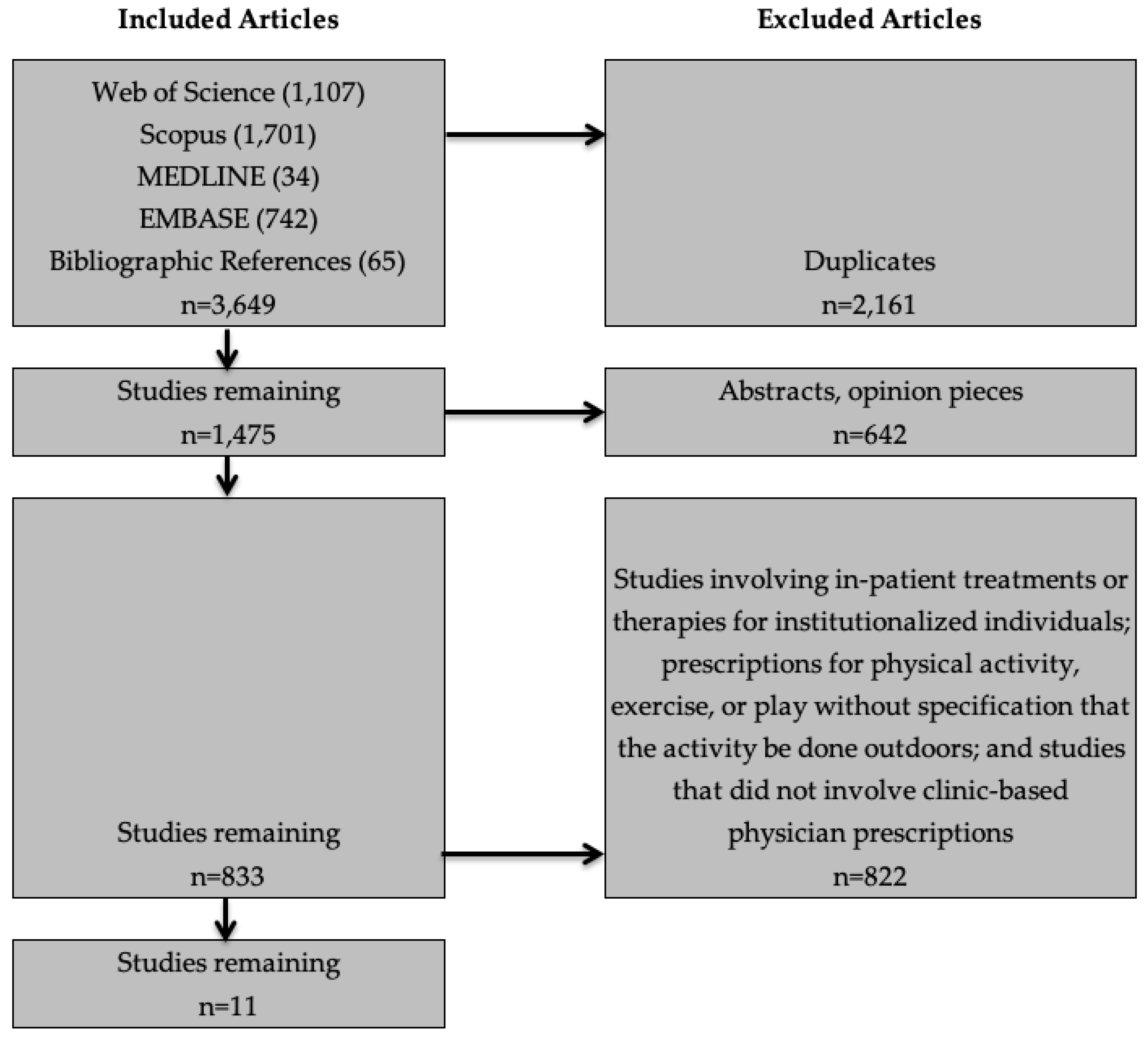
2. Materials and Methods
3. Results
3.1. Target Populations and Outcomes
3.2. Structural and Procedural Elements
3.2.1. Structured Versus Unstructured Program Components
3.2.2. Setting
3.2.3. Program Leadership, Implementation, and Partnerships
3.3. Empirical Studies: Impacts on Adherence and Health
3.3.1. Studies of Patients
3.3.2. Studies of Providers
4. Discussion and Agenda for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Buttorff, C.; Ruder, T.; Bauman, M. Multiple Chronic Conditions in the United States; RAND Corporation: Santa Monica, CA, USA, 2017. [Google Scholar]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; National Center for Health Statistics Data Brief No. 288; Centers for Disease Control and Prevention: Atlanta, GA, USA; National Center for Health Statistics: Hayesville, MD, USA, 2017.
- Van Cleave, J.; Gortmaker, S.L.; Perrin, J.M. Dynamics of obesity and chronic health conditions among children and youth. J. Am. Med. Assoc. 2010, 303, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Roberts, P.; Dhaliwal, S.; Della, P. Transitioning adolescent and young adults with chronic disease and/or disabilities from paediatric to adult care services—An integrative review. J. Clin. Nurs. 2016, 25, 3113–3130. [Google Scholar] [CrossRef]
- McManus, M.A.; Pollack, L.R.; Cooley, W.C.; McAllister, J.W.; Lotstein, D.; Strickland, B.; Mann, M.Y. Current Status of Transition Preparation Among Youth With Special Needs in the United States. Pediatrics 2013, 131, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Domingues-Montanari, S. Clinical and psychological effects of excessive screen time on children. J. Paediatr. Child Health 2017, 53, 333–338. [Google Scholar] [CrossRef]
- Trinh, L.; Wong, B.; Faulkner, G.E. The independent and interactive associations of screen time and physical activity on mental health, school connectedness and academic achievement among a population-based sample of youth. J. Can. Acad. Child Adolesc. Psychiatry 2015, 24, 17. [Google Scholar]
- Proper, K.I.; Singh, A.S.; Van Mechelen, W.; Chinapaw, M.J. Sedentary behaviors and health outcomes among adults: A systematic review of prospective studies. Am. J. Prev. Med. 2011, 40, 174–182. [Google Scholar] [CrossRef]
- Chen, W.; Adler, J.L. Assessment of Screen Exposure in Young Children, 1997 to 2014. JAMA Pediatr. 2019, 173, 391–393. [Google Scholar] [CrossRef]
- Kabali, H.K.; Irigoyen, M.M.; Nunez-Davis, R.; Budacki, J.G.; Mohanty, S.H.; Leister, K.P.; Bonner, R.L. Exposure and use of mobile media devices by young children. Pediatrics 2015, 136, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Hawkins, J.; Queen, B.; Lowry, R.; Olsen, E.O.; Chyen, D.; et al. Youth Risk Behavior Surveillance - United States, 2015. MMWR Surveill. Summ. 2016, 65, 1–174. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Physical Activity Facts; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- James, J.J.; Christiana, R.W.; Battista, R.A. A historical and critical analysis of park prescriptions. J. Leis. Res. 2019, 50, 311–329. [Google Scholar] [CrossRef]
- National ParksRx Initiative. ParkRx Program Directory; ParkRx: Tucson, AZ, USA, 2019. [Google Scholar]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef]
- Yasuda, K. Priorities for 2019 focus on health of children and physicians. Letter from the President. AAP News, 2 January 2019. [Google Scholar]
- National Physical Activity Plan Alliance. 2016 National Physical Activity Plan; National Physical Activity Plan Alliance: Columbia, SC, USA, 2016. [Google Scholar]
- Annerstedt, M.; Währborg, P. Nature-assisted therapy: Systematic review of controlled and observational studies. Scand. J. Public Health 2011, 39, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Clatworthy, J.; Hinds, J.; Camic, P.M. Gardening as a mental health intervention: A review. Ment. Health Rev. J. 2013, 18, 214–225. [Google Scholar] [CrossRef]
- Kamioka, H.; Tsutani, K.; Yamada, M.; Park, H.; Okuizumi, H.; Honda, T.; Okada, S.; Park, S.-J.; Kitayuguchi, J.; Abe, T. Effectiveness of horticultural therapy: A systematic review of randomized controlled trials. Complement. Ther. Med. 2014, 22, 930–943. [Google Scholar] [CrossRef]
- Barton, J.; Bragg, R.; Wood, C.; Pretty, J. Green Exercise: Linking Nature, Health and Well-Being; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The effects of green exercise on physical and mental wellbeing: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef]
- Mnich, C.; Weyland, S.; Jekauc, D.; Schipperijn, J. Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4266. [Google Scholar] [CrossRef]
- Gigliotti, C.M.; Jarrott, S.E. Effects of horticulture therapy on engagement and affect. Can. J. Aging/La Rev. Can. Vieil. 2005, 24, 367–377. [Google Scholar] [CrossRef]
- Kam, M.C.; Siu, A.M. Evaluation of a horticultural activity programme for persons with psychiatric illness. Hong Kong J. Occup. Ther. 2010, 20, 80–86. [Google Scholar] [CrossRef]
- Van Den Berg, A.E.; Custers, M.H. Gardening promotes neuroendocrine and affective restoration from stress. J. Health Psychol. 2011, 16, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Ackley, D.; Cole, L. The effect of a horticultural therapy program on children with cerebral palsy. J. Rehabil. 1987, 53, 70. [Google Scholar]
- Wichrowski, M.; Whiteson, J.; Haas, F.; Mola, A.; Rey, M.J. Effects of horticultural therapy on mood and heart rate in patients participating in an inpatient cardiopulmonary rehabilitation program. J. Cardiopulm. Rehabil. Prev. 2005, 25, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Hattie, J.; Marsh, H.W.; Neill, J.T.; Richards, G.E. Adventure education and Outward Bound: Out-of-class experiences that make a lasting difference. Rev. Educ. Res. 1997, 67, 43–87. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Thorne, S.; Malterud, K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur. J. Clin. Investig. 2018, 48, e12931. [Google Scholar] [CrossRef]
- Husk, K.; Lovell, R.; Garside, R. Prescribing gardening and conservation activities for health and wellbeing in older people. Maturitas 2018, 110, A1–A2. [Google Scholar] [CrossRef]
- Razani, N.; Meade, K.; Schudel, C.; Johnson, C.; Long, D. Healing through nature: A park-based health intervention for young people in Oakland, California. Child. Youth Environ. 2015, 25, 147–159. [Google Scholar] [CrossRef]
- Razani, N.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Flores, H.H.; Rutherford, G.W. Design and evaluation of a park prescription program for stress reduction and health promotion in low-income families: The Stay Healthy in Nature Everyday (SHINE) study protocol. Contemp. Clin. Trials 2016, 51, 8–14. [Google Scholar] [CrossRef]
- Messiah, S.E.; Jiang, S.; Kardys, J.; Hansen, E.; Nardi, M.; Forster, L. Reducing childhood obesity through coordinated care: Development of a park prescription program. World J. Clin. Pediatr. 2016, 5, 234. [Google Scholar] [CrossRef]
- Christiana, R.W.; Battista, R.A.; James, J.J.; Bergman, S.M. Pediatrician prescriptions for outdoor physical activity among children: A pilot study. Prev. Med. Rep. 2017, 5, 100–105. [Google Scholar] [CrossRef]
- Christiana, R.W.; James, J.J.; Battista, R.A. Prescribing Outdoor Physical Activity to Children: Health Care Providers’ Perspectives. Glob. Pediatr. Health 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Cimprich, B.; Ronis, D.L. An environmental intervention to restore attention in women with newly diagnosed breast cancer. Cancer Nurs. 2003, 26, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Coffey, J.S.; Gauderer, L. When Pediatric Primary Care Providers Prescribe Nature Engagement at a State Park, Do Children “Fill” the Prescription? Ecopsychology 2016, 8, 207–214. [Google Scholar] [CrossRef]
- James, A.K.; Hess, P.; Perkins, M.E.; Taveras, E.M.; Scirica, C.S. Prescribing Outdoor Play: Outdoors Rx. Clin. Pediatr. (Phila.) 2017, 56, 519–524. [Google Scholar] [CrossRef]
- Razani, N.; Niknam, K.; Wells, N.M.; Thompson, D.; Hills, N.K.; Kennedy, G.; Gilgoff, R.; Rutherford, G.W. Clinic and park partnerships for childhood resilience: A prospective study of park prescriptions. Health Place 2019, 57, 179–185. [Google Scholar] [CrossRef]
- Zarr, R.; Cottrell, L.; Merrill, C. Park prescription (DC Park Rx): A new strategy to combat chronic disease in children. J. Phys. Act. Health 2017, 14, 1–2. [Google Scholar] [CrossRef]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13, e0192921. [Google Scholar] [CrossRef]
- McCurdy, L.E.; Winterbottom, K.E.; Mehta, S.S.; Roberts, J.R. Using nature and outdoor activity to improve children’s health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 102–117. [Google Scholar] [CrossRef]
- Jepson, R.; Robertson, R.; Cameron, H. Green Prescription Schemes: Mapping and Current Practice; NHS Health Scotland: Edinburgh, Scotland, 2010. [Google Scholar]
- Bragg, R.; Leck, C. Good practice in social prescribing for mental health: The role of nature-based interventions. In Natural England Commissioned Reports Number 228; Natural England: York, UK, 2017. [Google Scholar]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Bloomfield, D.; Warber, S.; Pearson, M.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A protocol for a realist review. Syst. Rev. 2016, 5, 93. [Google Scholar] [CrossRef]
- Doherty, S.T.; Lemieux, C.J.; Canally, C. Tracking human activity and well-being in natural environments using wearable sensors and experience sampling. Soc. Sci. Med. 2014, 106, 83–92. [Google Scholar] [CrossRef]
- Doherty, S.T.; Oh, P. A multi-sensor monitoring system of human physiology and daily activities. Telemed. e-Health 2012, 18, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Walter, L.G.; Arroll, B.; Tilyard, M.W.; Russell, D.G. The green prescription study: A randomized controlled trial of written exercise advice provided by general practitioners. Am. J. Public Health 1998, 88, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.; Franklin, B.; Joy, L.; Ross, R.; Sabgir, D.; Stone, J. Strategies for promoting physical activity in clinical practice. Prog. Cardiovasc. Dis. 2015, 57, 375–386. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Program Descriptions | Population |
|---|---|---|
| Unstructured Prescriptions | ||
| Christiana et al. [37] | Patients receive counseling, education about local outdoor resources, and prescription for 60 min or more of outdoor physical activity per day | Children (ages 5–13) |
| Coffey and Gaurderer [40] | Participants receive counseling, education about local outdoor resources, and a 1-day free pass to any state park day use area | Children (ages 6–10) |
| Razani et al. [35,44] | Group 1: Patients receive counseling, education about local park resources, journals and pedometers | Children (low-income; ages 4–18) and parents |
| Razani et al. [42] | Group 1: Patients receive counseling and education about local park resources | Children (low-income; ages 7–17) and parents |
| Zarr et al. [43] | Patients receive education about local outdoor resources, and a prescription for outdoor physical activity | Children and adolescents (low-income) |
| Structured Prescriptions | ||
| Cimprich and Ronis [39] | Home-based program involving 120 min of exposure to the natural environment per week | Women with newly diagnosed breast cancer |
| James et al. [41] | Patients receive counseling and are referred to guided outdoor activities, with incentives | Children (low-income; ages 2–13) |
| Messiah et al. [36] | Patients receive counseling and referral to a park-based afterschool health and wellness program | Children and adolescents (low-income; ages 6–14) |
| Razani et al. [34] | Patients receive counseling, and are recruited to formal outings involving unstructured nature exploration and physical activity once a month | Infants, children and adolescents (low-income; ages 0–18) |
| Razani et al. [35,44] | Group 2: Patients recruited to 3 nature outings to parks where they engaged in unstructured nature play, physical activity and picnic, and quiet reflection | Children (low-income; ages 4–18) and parents |
| Razani et al. [42] | Group 2: Three organized group outings at three parks (among the seven parks highlighted in the map given to all families) over three weeks | Children (low-income; ages 7–17) and parents |
| Study | Target Study Population | Research Question or Aims | Target Health Outcomes | Study Design | Intervention | Methods | Results |
|---|---|---|---|---|---|---|---|
| Patient Studies | |||||||
| Cimprich and Ronis [39] | Female patients diagnosed with breast cancer (n = 157) | What is the effectiveness of an early natural restorative environmental intervention aimed at counteracting attentional fatigue? | Attentional fatigue and performance, time spent in nature | Pre-post test | Patients received 120 min of home-based exposure to the natural environment per week. Control patients received no intervention. | Self-reported capacity to direct attention assessed ~17 days before and 19 days after surgery. A home-based intervention was initiated after the first assessment and before any treatment. Participants recorded type of nature activity and time spent in each activity daily. | The intervention group showed greater recovery of capacity to direct attention after therapy, compared with the nonintervention group. |
| Christiana et al. [37] | (1) Patients (ages 5–13 years; n = 38) of 2 rural providers; (2) Patients (n = 32) of 5 non-participating providers | What is the effectiveness and feasibility of an intervention involving health care providers talking to their patients and parents about the importance of outdoor physical activity (PA) and prescribing outdoor activity for children? | Outdoor PA, sedentary behaviors, and time spent outdoors | Longitudinal pilot study | Patients received counseling about local outdoor resources and prescription for 60 min of outdoor PA per day. Control patients received no intervention. | Surveys administered to parents at baseline, 1 and 3 months after pediatrician visit; including items from Youth Risk Behavior Surveillance System; Leisure-Time Exercise Questionnaire; amount of time doing sedentary behaviors; how much time spent outdoors; parent view of prescriptions. | Changes in children’s outdoor PA, time spent in the outdoors, and sedentary activities were not significantly different between intervention and control groups. Wald chi-square values: Days in the past week child was physically active 60 min+ anywhere (3.97) or outdoors (2.46); Frequency of PA anywhere (1.28) or outdoors (2.34); Time spent outdoors (2.99); Time spent in sedentary activity on weekdays (1.80) and on weekend days (0.80). |
| Coffey and Gauderer [40] | (1) Patients (ages 6–10; n = 1935) | (1) Does a Park Rx encourage children to engage in a nature experience in the short term, as measured by redemption of the Park Rx at a local state park? | Increased time spent in nature | Quasi-experimental pilot study | Patients received counseling, education about local outdoor resources, and a 1-day free pass to any state park day use area. | Park staff counted redeemed ParkRx passes. Families had 15 weeks to redeem. | There was a 13% redemption rate. |
| Messiah et al. [36] | Low-income, minority children (ages 6–14; n = 50) diagnosed with overweight/obesity, hypertension, or family history of diabetes and/or cardiovascular disease | Can an affordable and accessible obesity prevention and treatment program reduce childhood obesity? | Increase in physical activity, decrease in BMI | Research design | Patients received education about local outdoor resources and prescription for outdoor physical activity. | Pediatric clinics patients were enrolled in the Fit-2-Play program. Focus groups were conducted with pediatricians, park coaches, and patients. | No results provided. |
| Razani et al. [34] | Patients (low income; ages 0–18; n= 20) | Help people engage in nature by diminishing the barriers (transportation, food, child care needs) | Combat stress and build resilience | Field report | Patients received counseling, and outings involving unstructured nature exploration and physical activity once a month. | Observation | Nature was a tool to deal with stressors associated with poverty; stress relief and time to relax with family motivated participation more than physical activity; variations in temperament and developmental stage make each child’s response unique; parents’ efforts to get their children outdoors should be acknowledged; being culturally responsive is important in nature. |
| Razani et al. [44] | Parents of patients (low income; ages 4–18; n = 78) | (1) Do park prescriptions improve parents’ stress, park visits, loneliness, physical activity and nature affinity? (2) Will a supported park prescription have a greater impact on stress and other outcomes than an unsupported prescription? | Physical activity, stress, loneliness, park visits per week | Randomized clinical trial with pre-post survey | Group 1: Patients received counseling, education about local park resources, journal and pedometer. Group 2: Patients recruited to 3 park outings where they engaged in unstructured nature play, physical activity and picnic, and quiet reflection. | Measures included Perceived Stress Scale, park visits, step counts, physical activity, UCLA Loneliness Score, salivary cortisol, and nature affinity. Measures occurred in both groups at 0, 1, and 3 months after enrollment. | Both groups saw decreases in stress (1.71 points); loneliness (1.03 points); cortisol level (0.05 μg/dL); and increases in park visits (1.22 visits per week); in time spent in moderate physical activity per week (24 min); and nature affinity (0.35 points). The unsupported group had a significant increase park visits compared to the supported group. |
| Razani et al. [42] | Patients (low-income; ages 7–17; n= 54) and their parent | (1) Are park visits associated with pediatric resilience over the three months after patients received a park prescription? (2) Are pediatric stress levels a mediating factor between weekly park visits and resilience? | Resilience, stress, park visits per week | Prospective longitudinal clinical trial | Patients recruited to 3 park outings over 3 weeks and received counseling. Patients assigned to intervention group received support in getting to the parks. | Parents reported their child’s park visits per week, baseline adverse childhood experience score, their own stress and coping; children reported resilience and stress. Measures occurred in both groups at 0, 1, and 3 months after enrollment. | Resilience improved with each 1-day increase in weekly park visits (0.04 points (0.01, 0.08) at every ACEs level. |
| Zarr et al. [43] | Patients (low-income; child & adolescent; n = 225 families) at risk for chronic illnesses | What is the impact of provider-based park prescriptions on outdoor physical activity? | Physical activity | Pre-post survey | Patients received education about local outdoor resources and prescription for outdoor physical activity. | Surveys administered to parents immediately before and 3 months after the intervention to assess changes in attitudes and behaviors around physical activity. | No significant changes in parental perceptions about parks or physical activity. Significant increase in the proportion of parents reporting of child’s park visits in the past year and that they believed that physical activity affected their child’s health. |
| Provider Studies | |||||||
| Christiana et al. [38] | Children’s health care providers (n = 15) | What are the barriers for health care providers to prescribing outdoor physical activity? | Physician perspective | Interviews | None | Semi-structured interviews to explore perspectives on outdoor PA prescription programs for children and barriers to implementation. | Providers’ lack of time, awareness of the benefits of parks/outdoors, and of programs’ effectiveness, and perceived patient barriers, were major barriers to program participation. |
| Coffey and Gauderer [40] | (2) Primary care providers (PCPs; n = 24) | (1) Does the PCP’s NR and/or participation in the pilot impact their likelihood of writing a park prescription? (2) Did study participation impact the PCP’s likelihood of discussing the value of nature during a well-child exam? | PCP Nature Relatedness (NR) score; likelihood to discuss the importance of nature during well-child exam | Quasi-experimental pilot study | Patients received counseling, education about local outdoor resources, and a one-day free pass to any state park day use area. | Surveyed providers about nature relatedness and likelihood to discuss nature with patients. | There were no difference in rate of park prescription between providers with low and high NR scores. Participation in the program increased PCP promotion of nature experiences. |
| James et al. [41] | Pediatricians participating in Outdoors Rx program (n = 23) | How do pediatricians view the utility of Outdoors Rx, barriers to success, and opportunities for improvement? | Pediatrician perspective | One-time survey | Providers gave patients counseling and referred them to guided outdoor activities, with incentives. | Surveyed pediatricians on Outdoors Rx: (a) referral patterns (b) impact on physical activity counseling, (c) perceived patient interest (d) barriers to success, and (e) suggestions for improvement. | Findings reveal providers’ referral patterns, participation impact on physical activity counseling, perceived patient interest, barriers to success, and suggestions for improvement. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondo, M.C.; Oyekanmi, K.O.; Gibson, A.; South, E.C.; Bocarro, J.; Hipp, J.A. Nature Prescriptions for Health: A Review of Evidence and Research Opportunities. Int. J. Environ. Res. Public Health 2020, 17, 4213. https://doi.org/10.3390/ijerph17124213
Kondo MC, Oyekanmi KO, Gibson A, South EC, Bocarro J, Hipp JA. Nature Prescriptions for Health: A Review of Evidence and Research Opportunities. International Journal of Environmental Research and Public Health. 2020; 17(12):4213. https://doi.org/10.3390/ijerph17124213
Chicago/Turabian StyleKondo, Michelle C., Kehinde O. Oyekanmi, Allison Gibson, Eugenia C. South, Jason Bocarro, and J. Aaron Hipp. 2020. "Nature Prescriptions for Health: A Review of Evidence and Research Opportunities" International Journal of Environmental Research and Public Health 17, no. 12: 4213. https://doi.org/10.3390/ijerph17124213
APA StyleKondo, M. C., Oyekanmi, K. O., Gibson, A., South, E. C., Bocarro, J., & Hipp, J. A. (2020). Nature Prescriptions for Health: A Review of Evidence and Research Opportunities. International Journal of Environmental Research and Public Health, 17(12), 4213. https://doi.org/10.3390/ijerph17124213