Predictors of High Resource Consumption in Alcohol Intoxicated Patients in the Emergency Department

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Site
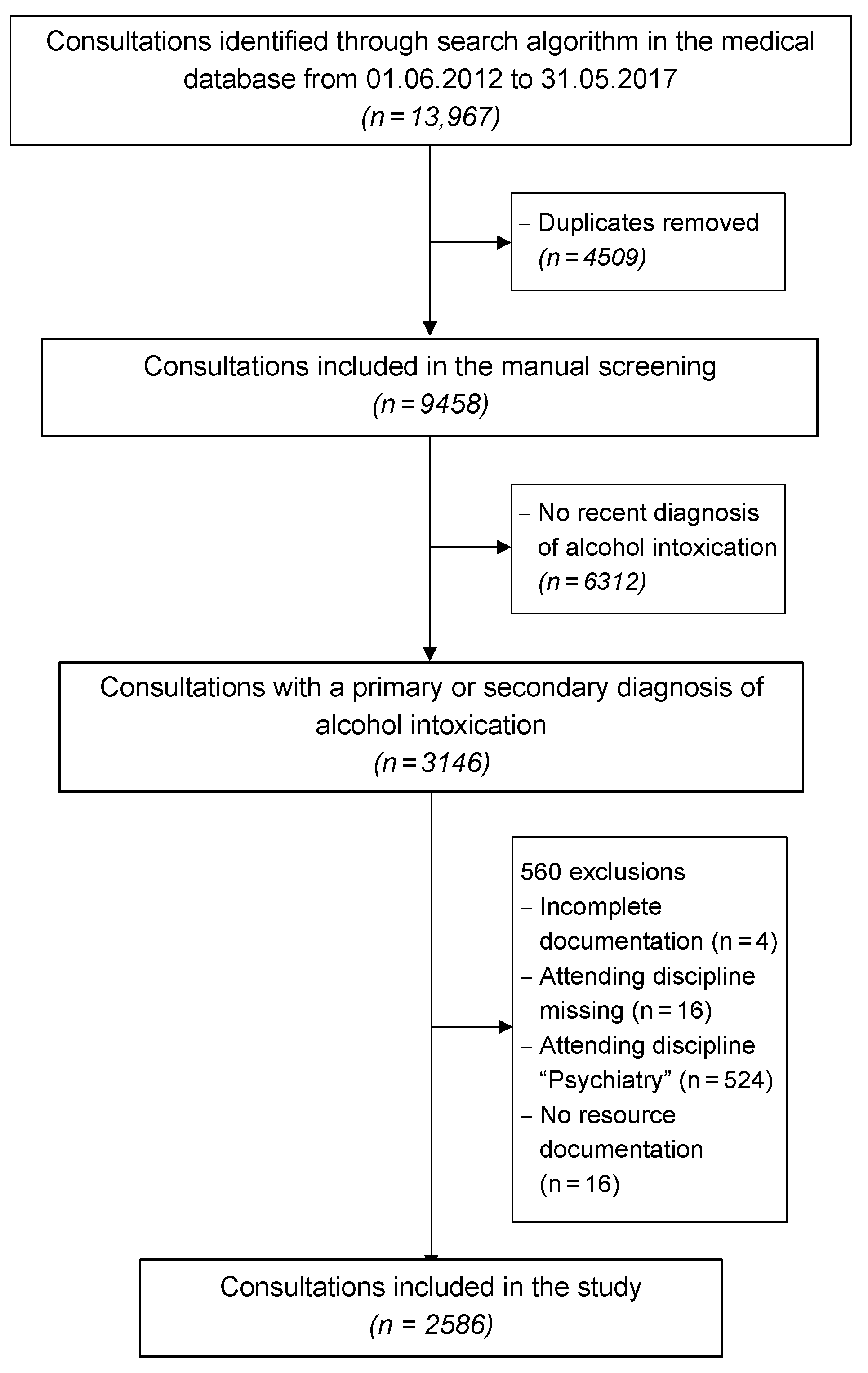
2.2. Data Collection and Eligibility Criteria
2.3. Data Extraction
- demographic data such as age, sex, and nationality;
- breath alcohol concentration, estimated blood alcohol concentration, or laboratory variables to estimate the blood alcohol concentration, i.e., sodium, potassium, urea, glucoses, and osmolality [22];
- signs of mixed intoxication;
- clinical presentation, i.e., any signs of aggression (verbal or physical), vital signs including the Glasgow Coma Scale (GCS), trauma grouped by fractures, traumatic brain injuries, cerebral bleeding, flesh or abrasion wounds, contusion, dislocation, and others (e.g., abdominal bleeding);
- treatment at the ED—intubation for respiratory compromise or police attendance needed;
- discharge procedure, such as emergency surgery, outpatient setting, or hospitalisation, as well as initial type of referral (walk-in, ambulance etc.).
- physicians’ work (including patient time and administrative time and costs);
- nurses’ work (including patient time and administrative time and costs);
- material expenses (e.g., injections, infusion, bandages, costs);
- laboratory resources (number, costs);
- radiology resources (ultrasound, computed tomography, X-rays, magnetic resonance imaging);
- total work or resources (sum of the above).
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Consultation Characteristics
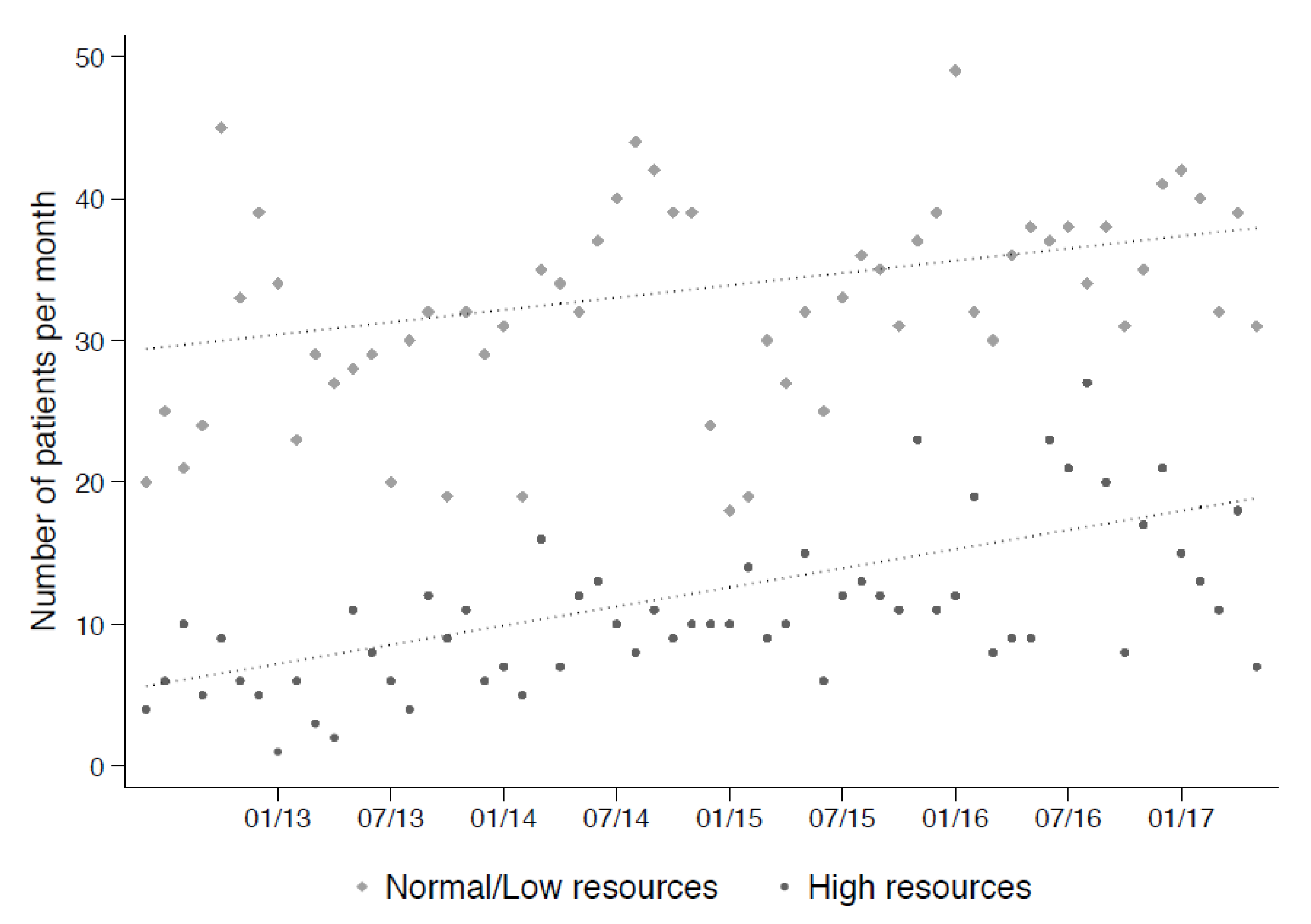
3.2. Resource Consumption
3.3. Predictors of Resource Consumption
4. Discussion
4.1. Proportional Incidence and Characteristics
4.2. Need of Resources
4.3. Predictors and Risk Factors
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mullins, P.M.; Mazer-Amirshahi, M.; Pines, J.M. Alcohol-Related Visits to US Emergency Departments, 2001–2011. Alcohol Alcohol. 2017, 52, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Holzer, B.; Minder, C.E.; Schätti, G.; Rosset, N.; Battegay, E.; Müller, S.; Zimmerli, L. Ten-Year Trends in Intoxications and Requests for Emergency Ambulance Service. Prehosp. Emerg. Care 2012, 16, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Verelst, S.; Moonen, P.-J.; Desruelles, D.; Gillet, J.-B. Emergency Department Visits Due to Alcohol Intoxication: Characteristics of Patients and Impact on the Emergency Room. Alcohol Alcohol. 2012, 47, 433–438. [Google Scholar] [CrossRef] [PubMed]
- O’Farrell, A.; Allwright, S.; Downey, J.; Bedford, D.; Howell, F. The burden of alcohol misuse on emergency in-patient hospital admissions among residents from a health board region in Ireland. Addiction 2004, 99, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO] Europe. Fact Sheet on Alcohol Consumption, Alcohol Attributable Harm and Alcohol Policy Responses in European Union Member States, Norway and Switzerland (2018). Available online: http://www.euro.who.int/en/health-topics/disease-prevention/alcohol-use/publications/2018/fact-sheet-on-alcohol-consumption,-alcohol-attributable-harm-and-alcohol-policy-responses-in-european-union-member-states,-norway-and-switzerland-2018 (accessed on 8 April 2020).
- World Health Organization [WHO]. World Health Statistics Data Visualization Dashbord. Harmful Use of Alcohol 2016. Last Updated: 20 March 2018. Available online: https://apps.who.int/gho/data/node.sdg.3-5-viz?lang=en (accessed on 8 April 2020).
- Swiss Federal Office of Public Health. Alcohol Consumption in Switzerland 2016, Fact Sheet. (Bundesamt für Gesundheit [BAG], Alkoholkonsum in der Schweiz im Jahr 2016, Faktenblatt). (PDF, 128kB). Available online: https://www.bag.admin.ch/bag/de/home/gesund-leben/sucht-und-gesundheit/alkohol.html (accessed on 13 October 2017).
- Gmel, G.; Kuendig, H.; Rehm, J.; Schreyer, N.; Daeppen, J.-B. Alcohol and cannabis use as risk factors for injury—A case-crossover analysis in a Swiss hospital emergency department. BMC Public Health 2009, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Mayor, S. Small increase in alcohol duty may cut violence related emergency department visits. BMJ 2016, 354, i3829. [Google Scholar] [CrossRef] [PubMed]
- Zeisser, C.; Stockwell, T.; Chikritzhs, T.; Cherpitel, C.; Ye, Y.; Gardner, C.; Cherpitel, C.J. A systematic review and meta-analysis of alcohol consumption and injury risk as a function of study design and recall period. Alcohol. Clin. Exp. Res. 2013, 37 (Suppl. 1), E1–E8. [Google Scholar] [CrossRef]
- Gmel, G.; Kuendig, H.; Gaume, J.; Daeppen, J.-B. Alcohol-related injuries—An emergency department study in the Lausanne University Hospital. Rev. Med. Suisse 2007, 3, 1964–1967. [Google Scholar] [PubMed]
- Mitra, B.; Charters, K.; Spencer, J.C.; Fitzgerald, M.; Cameron, P.A. Alcohol intoxication in non-motorised road trauma. Emerg. Med. Australas. 2017, 29, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Sethi, M.; Heyer, J.H.; Wall, S.P.; DiMaggio, C.; Shinseki, M.; Slaughter, D.; Frangos, S. Alcohol use by urban bicyclists is associated with more severe injury, greater hospital resource use, and higher mortality. Alcohol 2016, 53, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Downes, M.A.; Healy, P.; Page, C.B.; Bryant, J.L.; Isbister, G.K. Structured team approach to the agitated patient in the emergency department. Emerg. Med. Australas. 2009, 21, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Swiss Federal Office of Public Health. Final Report of the Study: Alcohol-Related Costs in Switzerland. (Bundesamt für Gesundheit [BAG], Schlussbericht Studie: Alkoholbedingte Kosten in der Schweiz (PDF, 985 kB). Available online: https://www.bag.admin.ch/bag/de/home/gesund-leben/sucht-und-gesundheit/alkohol/soziale-folgen/kosten.html (accessed on 8 April 2020).
- Swiss Federal Office of Public Health. The Compulsory Health Insurance in a Nutshell. (Bundesamt für Gesundheit [BAG] (PDF, 756 kB). Available online: https://www.bag.admin.ch/bag/en/home/versicherungen/krankenversicherung/krankenversicherung-das-wichtigste-in-kuerze.html (accessed on 10 January 2020).
- Homma, Y.; Yamauchi, S.; Mizobe, M.; Nakashima, Y.; Takahashi, J.; Funakoshi, H.; Urayama, K.Y.; Ohde, S.; Takahashi, O.; Shiga, T. Emergency department outpatient treatment of alcohol-intoxicated bicyclists increases the cost of medical care in Japan. PLoS ONE 2017, 12, e0174408. [Google Scholar] [CrossRef] [PubMed]
- Exadaktylos, A.K.; Hautz, W.E. Emergency Medicine in Switzerland. ICU Manag. Pract. 2015, 15, 160–163. [Google Scholar]
- Vonghia, L.; Leggio, L.; Ferrulli, A.; Bertini, M.; Gasbarrini, G.; Addolorato, G. Acute alcohol intoxication. Eur. J. Intern. Med. 2008, 19, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Philadelphia, PA, USA, 1994.
- TARMED Suisse. TARMED 01.08.0000. Available online: http://www.tarmedsuisse.ch/pdf-tarifbrowser.html (accessed on 24 June 2017).
- Purssell, R.A.; Pudek, M.; Brubacher, J.; Abu-Laban, R.B. Derivation and validation of a formula to calculate the contribution of ethanol to the osmolal gap. Ann. Emerg. Med. 2001, 38, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.; Keliher, T.; Fisher, J.; Ritchie, F.; Bell, C.; Chekroud, M.; Clarey, F.; Blackwood, L.; Barry, L.; Paton, E.; et al. Quantifying alcohol-related emergency admissions in a UK tertiary referral hospital: A cross-sectional study of chronic alcohol dependency and acute alcohol intoxication. BMJ Open 2016, 6, e010005. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, K.N.; Newbury-Birch, D.; Phillipson, A.; Hindmarch, P.; Kaner, E.; Stamp, E.; Vale, L.; Wright, J.; Connolly, J. Prevalence of alcohol related attendance at an inner city emergency department and its impact: A dual prospective and retrospective cohort study. Emerg. Med. J. 2016, 33, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Eidgenössische Alkoholverwaltung [Federal Alcohol Administration]. Alcohol in Numbers [Alkohol in Zahlen 2017—Statistiken der Eidgenōssischen Alkoholverwaltung]. Available online: https://www.ezv.admin.ch/dam/ezv/de/dokumente/abgaben/AAT/Alkohol%20in%20Zahlen/alkohol_in_zahlen_2017.pdf.download.pdf/alkohol_in_zahlen_d_2017.pdf (accessed on 2 October 2018).
- Mica, L.; Oesterle, L.; Werner, C.M.; Simmen, H.-P. Age and Gender as Independent Predictors of Violence under the Influence of Alcohol in Zurich, Switzerland. Praxis 2015, 104, 397–401. [Google Scholar] [CrossRef]
- Stiell, I.G.; Clement, C.M.; Rowe, B.H.; Schull, M.J.; Brison, R.J.; Cass, D.; Eisenhauer, M.A.; McKnight, R.D.; Bandiera, G.; Holroyd, B.; et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in Patients with Minor Head Injury. JAMA 2005, 294, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Faouzi, M.; Yersin, B.; Bodenmann, P.; Daeppen, J.-B.; Bertholet, N. Women and Men Admitted for Alcohol Intoxication at an Emergency Department: Alcohol Use Disorders, Substance Use and Health and Social Status 7 Years Later. Alcohol Alcohol. 2016, 51, 567–575. [Google Scholar] [CrossRef]
- Page, N.; Sivarajasingam, V.; Matthews, K.; Heravi, S.; Morgan, P.; Shepherd, J. Preventing violence-related injuries in England and Wales: A panel study examining the impact of on-trade and off-trade alcohol prices. Inj. Prev. 2017, 23, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Wurdak, M.; Wolstein, J.; Kuntsche, E. Effectiveness of a drinking-motive-tailored emergency-room intervention among adolescents admitted to hospital due to acute alcohol intoxication—A randomized controlled trial. Prev. Med. Rep. 2016, 3, 83–89. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 2586) | High (n = 646) | Low/Normal (n = 1940) | p |
|---|---|---|---|---|
| Mixed intoxication, (n (%)) | 840 (32.5) | 164 (25.4) | 676 (34.8) | <0.001 |
| Blood alcohol concentration *, (median (IQR)) | 1.6 (1.1–2.2) | 1.6(1.2–2.2) | 1.6 (1.1–2.2) | 0.422 |
| Sex, (n (%)) | ||||
| Male | 1645 (63.6) | 461 (71.4) | 1184 (61.0) | <0.001 |
| Age, (median (IQR)) | 38 (26–52) | 47 (31–60) | 35(24–50) | <0.001 |
| Type of admission, (n (%)) | ||||
| Ambulance | 1815 (70.2) | 483 (74.8) | 1332 (68.7) | 0.003 |
| General Practitioner | 24 (0.9) | 9 (1.4) | 15 (0.8) | 0.155 |
| External Hospital | 100 (3.9) | 27 (4.2) | 73(3.8) | 0.634 |
| Police | 153 (5.9) | 22 (3.4) | 131 (6.8) | 0.002 |
| Air Rescue | 37 (1.4) | 31 (4.8) | 6(0.3) | <0.001 |
| Walk-In | 457 (17.7) | 74 (11.5) | 383 (19.7) | <0.001 |
| Triage, (n (%)) | ||||
| Life-threatening | 208 (8.0) | 130 (20.1) | 78 (4.0) | <0.001 |
| Urgent conditions | 959(37.1) | 280 (43.3) | 679 (35.0) | <0.001 |
| Semi-urgent conditions | 1293 (50.0) | 201 (31.1) | 1092 (56.3) | <0.001 |
| Non-urgent conditions | 74 (2.9) | 11 (1.7) | 63 (3.2) | 0.041 |
| Missing | 52 (2.0) | 24 (3.7) | 28 (1.4) | <0.001 |
| Discipline, (n (%)) | ||||
| Internal medicine | 1721 (66.6) | 224 (34.7) | 1497 (77.2) | <0.001 |
| Surgery | 853 (33.0) | 422 (65.3) | 431 (22.2) | <0.001 |
| Fast-Track | 12 (0.5) | 0 (0.0) | 12 (0.6) | 0.045 |
| Trauma room, (n (%)) | 270 (10.4) | 212 (32.8) | 58 (3.0) | <0.001 |
| Discharge, (n (%)) | ||||
| Outpatient treatment | 1747 (67.6) | 365 (56.5) | 1382 (71.2) | <0.001 |
| Hospital admission | 839(32.4) | 281 (43.5) | 558 (28.8) | <0.001 |
| Resource Group | Total (n = 2586) | High (n = 646) | Low/Normal (n = 1940) | p |
|---|---|---|---|---|
| Total work (TP) | 1200 (790–1901) | 2615 (2219–3490) | 986 (679–1314) | <0.001 |
| Physicians’ work | ||||
| Total physicians’ work (TP) | 465 (329–633) | 712 (539–929) | 415 (309–535) | <0.001 |
| Patient time (TP) | 160 (115–231) | 231 (169–329) | 151 (107–195) | <0.001 |
| Admin time (TP) | 160 (89–231) | 249 (160–355) | 124 (89–195) | <0.001 |
| Report time (TP) | 39 (39–71) | 71 (39–103) | 39 (39–71) | <0.001 |
| Nurses’ work | ||||
| Total nurses’ work (TP) | 290 (164–374) | 360 (275–433) | 270 (124–348) | <0.001 |
| Nurse patient time (TP) | 255 (105–300) | 285 (209–345) | 235 (88–285) | <0.001 |
| Nurse other effort (TP) | 35 (0–93) | 62 (35–98) | 35 (0–93) | <0.001 |
| Material expenses (TP) | 9 (5–25) | 35 (17–74) | 8 (4–11) | <0.001 |
| Laboratory resources | ||||
| Total laboratory effort (TP) | 195 (88–330) | 315 (176–441) | 155 (76–293) | <0.001 |
| Blood taken (yes), n (%) | 2214 (85.6) | 628 (97.2) | 1586 (81.8) | <0.001 |
| Radiology resources | ||||
| Total effort radiology (TP) | 0 (0–746) | 1147 (851–1820) | 0 (0–164) | <0.001 |
| Ultrasound, n (%) | 269 (10.4) | 210 (32.5) | 59 (3.0) | <0.001 |
| X-ray, n (%) | 1126 (43.5) | 628 (97.2) | 498 (25.7) | <0.001 |
| CT, n (%) | 875 (33.8) | 566 (87.6) | 309 (15.9) | <0.001 |
| MRI, n (%) | 50 (1.9) | 47 (7.3) | 3 (0.2) | <0.001 |
| High Resource Consumption | Odds Ratio | 95% Conf. Interval | p |
|---|---|---|---|
| Circumstances | |||
| Age, (per year) | 1.03 | 1.03, 1.04 | <0.001 |
| Sex, (male) | 1.59 | 1.31, 1.93 | <0.001 |
| Mixed intoxication, (yes) | 0.64 | 0.52, 0.78 | <0.001 |
| Suicidal intent, (yes) | 0.49 | 0.35, 0.71 | <0.001 |
| Aggressive, (yes) | 1.03 | 0.71, 1.49 | 0.882 |
| GCS ≤ 9, (yes) | 2.52 | 1.84, 3.46 | <0.001 |
| Accompanying injuries | |||
| Fracture, (yes) | 6.54 | 4.97, 8.6 | <0.001 |
| Traumatic brain injury, (yes) | 6.92 | 5.05, 9.48 | <0.001 |
| Cerebral bleeding, (yes) | 6.50 | 3.73, 11.33 | <0.001 |
| Dislocation, (yes) | 5.03 | 2.36, 10.7 | <0.001 |
| Contusion, (yes) | 3.98 | 2.88, 5.49 | <0.001 |
| Flesh wound, (yes) | 3.79 | 3, 4.78 | <0.001 |
| Abrasion wound, (yes) | 4.14 | 3.33, 5.13 | <0.001 |
| Blood alcohol concentration*, (per g/Kg) | 1.00 | 0.89, 1.13 | 0.961 |
| Procedure | |||
| Police attendance, (yes) | 0.90 | 0.72, 1.12 | 0.354 |
| Emergency surgery, (yes) | 3.30 | 2.33, 4.65 | <0.001 |
| Intubation needed, (yes) | 5.45 | 2.93, 10.14 | <0.001 |
| (A) High Resource Consumption | Odds Ratio | 95% Conf. Interval | p |
|---|---|---|---|
| Age | 1.03 | 1.03, 1.04 | <0.001 |
| GCS ≤ 9 | 2.83 | 1.89, 4.23 | <0.001 |
| Suicidal intent | 0.56 | 0.38, 0.82 | 0.003 |
| Aggressive | 1.41 | 0.95, 2.11 | 0.090 |
| Fracture | 3.88 | 2.83, 5.32 | <0.001 |
| Traumatic brain injury | 3.52 | 2.44, 5.06 | <0.001 |
| Dislocation | 3.65 | 1.46, 9.13 | 0.006 |
| Contusion | 2.55 | 1.75, 3.70 | <0.001 |
| Flesh wound | 1.78 | 1.23, 2.59 | 0.002 |
| Abrasion wound | 2.15 | 1.52, 3.04 | <0.001 |
| Intubation | 2.04 | 0.90, 4.61 | 0.088 |
| (B) Total resources | Coefficient | 95% Conf. Interval | p |
| Age | 12 | 10, 15 | <0.001 |
| Mixed intoxication | 113 | 32, 193 | 0.006 |
| GCS ≤ 9 | 653 | 490, 816 | <0.001 |
| Fracture | 925 | 791, 1060 | <0.001 |
| Traumatic brain injury | 672 | 518, 826 | <0.001 |
| Cerebral bleeding | 249 | −18, 515 | 0.067 |
| Dislocation | 329 | −25, 683 | 0.068 |
| Contusion | 460 | 304, 617 | <0.001 |
| Flesh wound | 142 | −13, 297 | 0.073 |
| Abrasion wound | 338 | 193, 483 | <0.001 |
| Intubation | 590 | 274, 906 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rönz, K.; Hirschi, T.; Becker, S.; Krummrey, G.; Exadaktylos, A.K.; Sauter, T.C.; Hautz, W.E.; Müller, M. Predictors of High Resource Consumption in Alcohol Intoxicated Patients in the Emergency Department. Int. J. Environ. Res. Public Health 2020, 17, 4122. https://doi.org/10.3390/ijerph17114122
Rönz K, Hirschi T, Becker S, Krummrey G, Exadaktylos AK, Sauter TC, Hautz WE, Müller M. Predictors of High Resource Consumption in Alcohol Intoxicated Patients in the Emergency Department. International Journal of Environmental Research and Public Health. 2020; 17(11):4122. https://doi.org/10.3390/ijerph17114122
Chicago/Turabian StyleRönz, Katharina, Trevor Hirschi, Sebastian Becker, Gert Krummrey, Aristomenis K. Exadaktylos, Thomas C. Sauter, Wolf E. Hautz, and Martin Müller. 2020. "Predictors of High Resource Consumption in Alcohol Intoxicated Patients in the Emergency Department" International Journal of Environmental Research and Public Health 17, no. 11: 4122. https://doi.org/10.3390/ijerph17114122
APA StyleRönz, K., Hirschi, T., Becker, S., Krummrey, G., Exadaktylos, A. K., Sauter, T. C., Hautz, W. E., & Müller, M. (2020). Predictors of High Resource Consumption in Alcohol Intoxicated Patients in the Emergency Department. International Journal of Environmental Research and Public Health, 17(11), 4122. https://doi.org/10.3390/ijerph17114122