Therapeutic Atmosphere in Psychotherapy Sessions

 ,
, 
Abstract
1. Introduction
Theoretical Framework
2. Method
2.1. FEST
2.1.1. Patients and Therapists
2.1.2. Treatment
2.1.3. Assessment/Measures
2.1.4. FEST Results
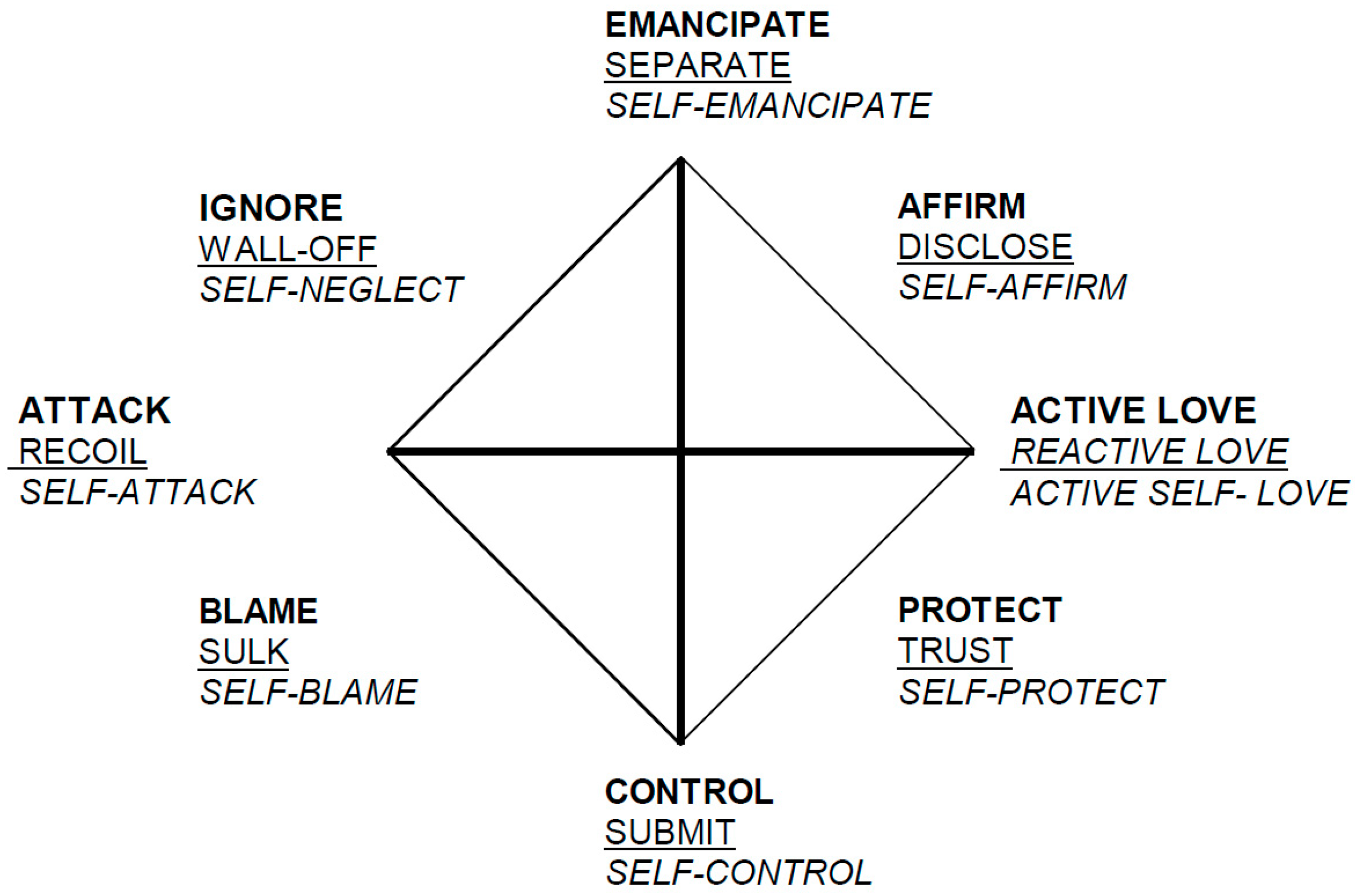
2.2. SASB
2.2.1. Patients
2.2.2. Statistical Analysis
3. Results
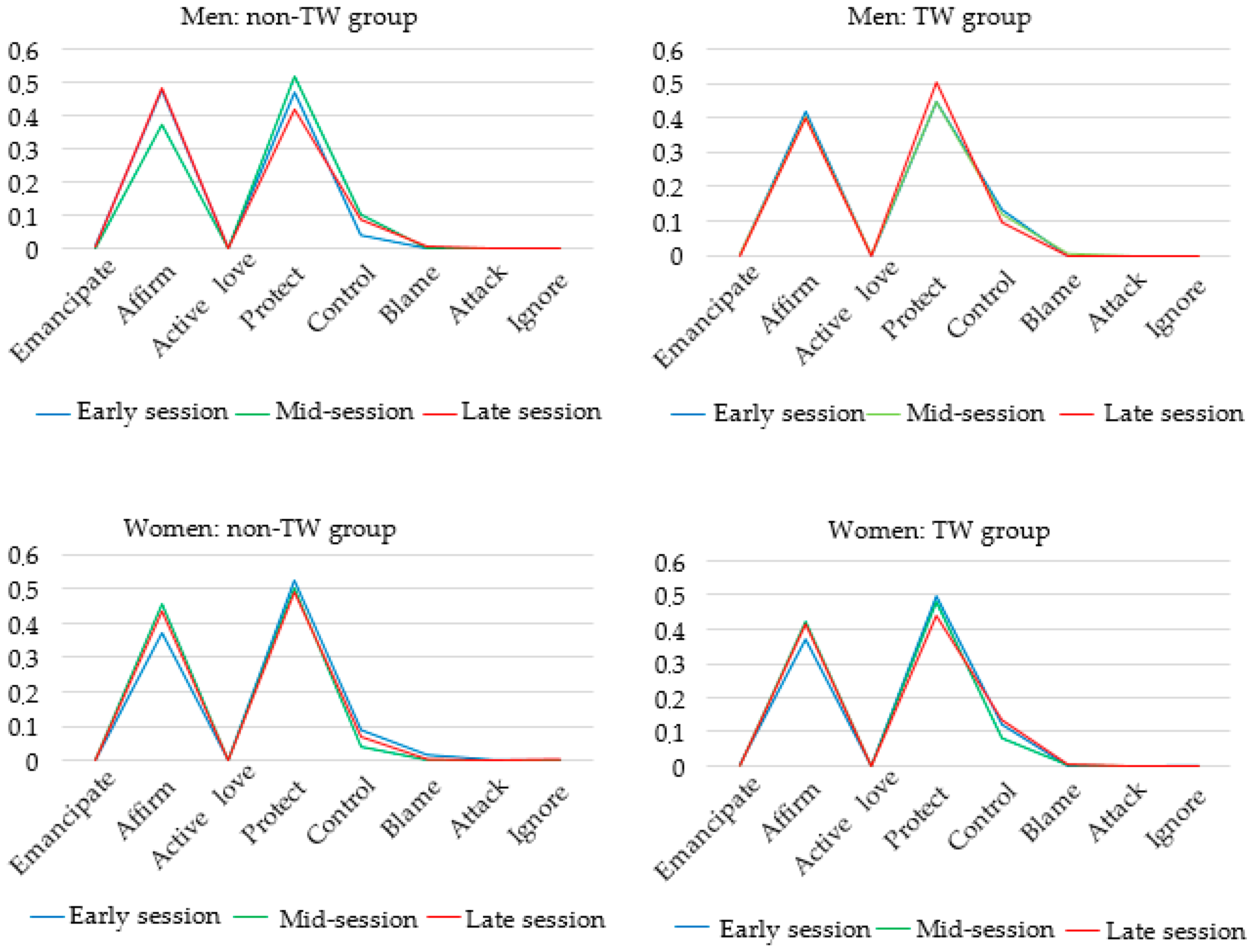
3.1. Line Charts
3.2. ANOVA
3.3. Multilevel Modeling
4. Discussion
4.1. Limitations
4.2. Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lambert, M.J. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change, 6th ed.; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar]
- Smith, M.L.; Glass, G.V. Meta-analysis of psychotherapy outcome studies. Am. Psychol. 1977, 32, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Wampold, B.E.; Imel, Z.E. The Great Psychotherapy Debate: The Evidence for What Makes Psychotherapy Work, 2nd ed.; Routledge/Taylor & Francis Group: New York, NY, USA, 2015. [Google Scholar]
- Kazdin, A.E. Understanding how and why psychotherapy leads to change. Psychother. Res. 2009, 19, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Wampold, B.E. How important are the common factors in psychotherapy? An update. World Psychiatry 2015, 14, 270–277. [Google Scholar] [CrossRef]
- Harper, F.D.; Bruce-Sanford, G.C. Counseling Techniques: An Outline & Overview; Douglass Publishers: Charlottesville, VA, USA, 1989. [Google Scholar]
- Linden, M.; Linden, U.; Schwantes, U. Disability and functional burden of disease because of mental in comparison to somatic disorders in general practice patients. Eur. Psychiatry 2015, 30, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Shedler, J. The efficacy of psychodynamic psychotherapy. Am. Psychol. 2010, 65, 98–109. [Google Scholar] [CrossRef]
- Girard, J.M.; Wright, A.G.C.; Beeney, J.E.; Lazarus, S.A.; Scott, L.N.; Stepp, S.D.; Pilkonis, P.A. Interpersonal problems across levels of the psychopathology hierarchy. Comp. Psychiatry 2017, 79, 53–69. [Google Scholar] [CrossRef]
- Safran, J.D. Psychoanalysis and Psychoanalytic Therapies; American Psychological Association: Washington, DC, USA, 2012. [Google Scholar]
- Freud, S. Fragments of an analysis of a case of hysteria. In The Complete Psychological Works of Sigmund Freud (1905); Stratchey, J., Ed.; Hogarth Press: London, UK, 1953; Volume 1, pp. 3–122. [Google Scholar]
- Pallini, S.; Baiocco, R.; Schneider, B.H.; Madigan, S.; Atkinson, L. Early child-parent attachment and peer relations: A meta-analysis of recent research. J. Fam. Psychol. 2014, 28, 118–123. [Google Scholar] [CrossRef]
- Henry, W.P. Structural analysis of social behavior as a common metric for programmatic psychopathology and psychotherapy research. J. Consult. Clin. Psychol. 1996, 64, 1263–1275. [Google Scholar] [CrossRef]
- Mitchell, S.A. Freud and Beyond: A History of Modern Psychoanalytic Thought, 2nd ed.; Basic Books: New York, NY, USA, 2016. [Google Scholar]
- Levy, K.N.; Scala, J.W. Transference, transference interpretations, and transference-focused psychotherapies. Psychotherapy 2012, 49, 391–403. [Google Scholar] [CrossRef]
- Høglend, P.; Amlo, S.; Marble, A.; Bogwald, K.P.; Sorbye, O.; Sjaastad, M.C.; Heyerdahl, O. Analysis of the patient-therapist relationship in dynamic psychotherapy: An experimental study of transference interpretations. Am. J. Psychiatry 2006, 163, 1739–1746. [Google Scholar] [CrossRef]
- Piper, W.E.; Duncan, S.C. Object relations theory and short term dynamic psychotherapy: Findings form the Quality of Object Relations Scale. Clin. Psychol. Rev. 1999, 19, 669–685. [Google Scholar] [CrossRef]
- Høglend, P. Long-Term Effects of Brief Dynamic Psychotherapy. J. Soc. Psychother. Res. 2003, 13, 271–292. [Google Scholar] [CrossRef]
- Høglend, P.; Bøgwald, K.-P.; Amlo, S.; Marble, A.; Ulberg, R.; Sjaastad, M.C.; Sørbye, Ø.; Heyerdahl, O.; Johansson, P. Transference interpretations in dynamic psychotherapy: Do they really yield sustained effects? Am. J. Psychiatry 2008, 165, 763–771. [Google Scholar] [CrossRef]
- Ulberg, R.; Johansson, P.; Marble, A.; Hoglend, P. Patient sex as moderator of effects of transference interpretation in a randomized controlled study of dynamic psychotherapy. Can. J. Psychiatry 2009, 54, 78–86. [Google Scholar] [CrossRef]
- Benjamin, L.S. Structural analysis of social behavior. Psychol. Rev. 1974, 81, 392–425. [Google Scholar] [CrossRef]
- Constantino, M.J. Interpersonal process in psychotherapy through the lens of the structural analysis of social behavior. Appl. Prev. Psychol. 2000, 9, 153–172. [Google Scholar] [CrossRef]
- Henry, W.P.; Schacht, T.E.; Strupp, H.H. Structural analysis of social behavior: Application to a study of interpersonal process in differential psychotherapeutic outcome. J. Consult. Clin. Psychol. 1986, 54, 27–31. [Google Scholar] [CrossRef]
- Henry, W.P.; Schacht, T.E.; Strupp, H.H. Patient and therapist introject, interpersonal process, and differential psychotherapy outcome. J. Consult. Clin. Psychol. 1990, 58, 768–774. [Google Scholar] [CrossRef]
- Critchfield, K.L.; Henry, W.P.; Castonguay, L.G.; Borkovec, T.D. Interpersonal process and outcome in variants of cognitive–behavioral psychotherapy. J. Clin. Psychol. 2007, 63, 31–51. [Google Scholar] [CrossRef]
- Von der Lippe, A.L.; Monsen, J.T.; Rønnestad, M.H.; Eilertsen, D.E. Treatment failure in psychotherapy: The pull of hostility. Psychother. Res. 2008, 18, 420–432. [Google Scholar] [CrossRef]
- Høglend, P. Dynamisk kortidsterapi (Brief dynamic Psychotherapy). In Poliklinikken Psykiatrisk Klinikk 25 år; Alnes, R., Ekern, P., Jarval, P., Eds.; Psykiatrisk Klinikk Vinderen, Universitetet i Oslo: Oslo, Norway, 1990; pp. 27–38. [Google Scholar]
- Høglend, P.; Bøgwald, K.-P.; Amlo, S.; Heyerdahl, O.; Sørbye, Ø.; Marble, A.; Sjaastad, M.C.; Bentsen, H. Assessment of change in dynamic psychotherapy. J. Psychother. Pract. Res. 2000, 9, 190–199. [Google Scholar] [PubMed]
- Bøgwald, K.-P.; Dahlbender, R.W. Procedures for testing some aspects of the content validity of the psychodynamic functioning Scales and the Global Assessment of Functioning Scale. Psychother. Res. 2004, 14, 453–468. [Google Scholar] [CrossRef]
- Hagtvet, K.A.; Heglend, P.A. Assessing Precision of Change Scores in Psychodynamic Psychotherapy: A Generalizability Theory Approach. Meas. Eval. Couns. Dev. 2008, 41, 162–178. [Google Scholar] [CrossRef]
- Johansson, P.; Hoglend, P.; Ulberg, R.; Amlo, S.; Marble, A.; Bogwald, K.P.; Sorbye, O.; Sjaastad, M.C.; Heyerdahl, O. The mediating role of insight for long-term improvements in psychodynamic therapy. J. Consult. Clin. Psychol. 2010, 78, 438–448. [Google Scholar] [CrossRef]
- Ulberg, R.; Høglend, P.; Marble, A.; Sørbye, Ø. From submission to autonomy: Approaching independent decision making. A single-case study in a randomized, controlled study of long-term effects of dynamic psychotherapy. Am. J. Psychother. 2009, 63, 227–243. [Google Scholar] [CrossRef]
- Ulberg, R.; Hoglend, P.; Marble, A.; Johansson, P. Women respond more favorably to transference intervention than men: A randomized study of long-term effects. J. Nerv. Ment. Dis. 2012, 200, 223–229. [Google Scholar] [CrossRef]
- Benjamin, L.S. Structural analysis of social behavior: The Rosetta Stone for Interpersonal Reconstructive Therapy case formulation and treatment models. In Interpersonal Reconstructive Therapy for Anger, Anxiety, and Depression: It’s about Broken Hearts, Not Broken Brains; American Psychological Association: Washington, DC, USA, 2018; pp. 53–81. [Google Scholar]
- Benjamin, L.S. A clinician-friendly version of the Interpersonal Circumplex: Structural Analysis of Social Behavior (SASB). J. Pers. Assess. 1996, 66, 248–266. [Google Scholar] [CrossRef]
- Benjamin, L.S.; Cushing, G. Reference Manual for Coding Social Interactions in Terms of Structural Analysis of Social Behavior; University of Utah: Salt Lake City, UT, USA, 2000. [Google Scholar]
- Benjamin, L.S. Interpersonal Diagnosis and Treatment of Personality Disorders, 2nd ed.; Guilford Press: New York, NY, USA, 1996. [Google Scholar]
- Alden, L.E.; Wiggins, J.S.; Pincus, A.L. Construction of circumplex scales for the Inventory of Interpersonal Problems. J. Pers. Assess. 1990, 55, 521–536. [Google Scholar] [CrossRef]
- Derogatis, L. SCL-90–R: Administration, Scoring and Procedures Manual II; Clinical Psychometric Research: Towson, M.D, USA, 1983. [Google Scholar]
- IBM. IBM SPSS Statistics for Windows, 25.0; IBM: Armonk, NY, USA, 2017. [Google Scholar]
- Sullivan, H.S. The Interpersonal Theory of Psychiatry; W W Norton & Co: New York, NY, USA, 1953; pp. xviii, 393-xviii, 393. [Google Scholar]
- Horvath, A.O.; Del Re, A.C.; Fluckiger, C.; Symonds, D. Alliance in individual psychotherapy. Psychotherapy 2011, 48, 9–16. [Google Scholar] [CrossRef]
- Høglend, P.; Hersoug, A.G.; Bogwald, K.P.; Amlo, S.; Marble, A.; Sorbye, O.; Rossberg, J.I.; Ulberg, R.; Gabbard, G.O.; Crits-Christoph, P. Effects of transference work in the context of therapeutic alliance and quality of object relations. J. Consult. Clin. Psychol. 2011, 79, 697–706. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Barlow, D.H. Evidence-based psychological interventions and the common factors approach: The beginnings of a rapprochement? Psychotherapy. 2014, 51, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Laska, K.M.; Gurman, A.S.; Wampold, B.E. Expanding the lens of evidence-based practice in psychotherapy: A common factors perspective. Psychotherapy 2014, 51, 467–481. [Google Scholar] [CrossRef]
- Monsen, J.T.; Hagtvet, K.A.; Havik, O.E.; Eilertsen, D.E. Circumplex structure and personality disorder correlates of the Interpersonal Problems model (IIP-C): Construct validity and clinical implications. Psychol. Assess. 2006, 18, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Crits-Christoph, P.; Gibbons, M.B.C.; Temes, C.M.; Elkin, I.; Gallop, R. Interpersonal accuracy of interventions and the outcome of cognitive and interpersonal therapies for depression. J. Consult. Clin. Psychol. 2010, 78, 420–428. [Google Scholar] [CrossRef]
- Bøgwald, K.P.; Høglend, P.; Sørbye, O.; Bøgwald, K.P. Measurement of transference interpretations. J. Psychother. Pract. Res. 1999, 8, 264–273. [Google Scholar]
- Tasca, G.A.; McMullen, L.M. Interpersonal complementarity and antitheses within a stage model of psychotherapy. Psychother. Theory Res. Pract. Train. 1992, 29, 515–523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1. The therapist was to address transactions in the patient–therapist relationship. |
| 2. The therapist was to encourage the exploration of thoughts and feelings about the therapy and therapist. |
| 3. The therapist was to encourage patients to discuss how they believed the therapist might feel or think about them. |
| 4. The therapist was to include him/herself explicitly in interpretive linking of dynamic elements (conflicts), direct manifestations of transference, and allusions to the transference. |
| 5. The therapist was to interpret repetitive interpersonal patterns (including genetic interpretations) and link these patterns to transactions between the patient and the therapist. |
| Low QOR Women (N = 21) | High QOR Men (N = 21) | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | TW Group (N = 11) | Non-TW Group (N = 10) | TW Group (N = 11) | Non-TW Group (N = 10) | ||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age | 32.6 | 7.3 | 34.7 | 9.5 | 40.7 | 9.8 | 40.4 | 9.8 |
| IIP-C * | 1.2 | 0.3 | 1.3 | 0.5 | 1.2 | 0.6 | 1.2 | 0.5 |
| GSI (SL-90) ** | 1.2 | 0.8 | 1.2 | 0.4 | 1.1 | 0.6 | 0.8 | 0.5 |
| PFS *** | 61.8 | 1.8 | 59 | 4.8 | 65.1 | 3.7 | 67.6 | 3.1 |
| PD-Criteria (SCID-II) | 11.5 | 6.3 | 11.5 | 7.6 | 7.3 | 6.4 | 3.9 | 3.1 |
| N | % | N | % | N | % | N | % | |
| Single | 6 | 54.5 | 4 | 40 | 1 | 9 | 1 | 10 |
| Caucasian | 11 | 100 | 10 | 100 | 11 | 100 | 10 | 100 |
| Personality Disorder | 7 | 63.6 | 6 | 60 | 3 | 27.3 | 1 | 10 |
| Active employment | 5 | 45.5 | 7 | 70 | 10 | 90.9 | 6 | 60 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegel, M.L.; Gullestad Binder, E.M.; Dahl, H.S.J.; Czajkowski, N.O.; Critchfield, K.L.; Høglend, P.A.; Ulberg, R. Therapeutic Atmosphere in Psychotherapy Sessions. Int. J. Environ. Res. Public Health 2020, 17, 4105. https://doi.org/10.3390/ijerph17114105
Siegel ML, Gullestad Binder EM, Dahl HSJ, Czajkowski NO, Critchfield KL, Høglend PA, Ulberg R. Therapeutic Atmosphere in Psychotherapy Sessions. International Journal of Environmental Research and Public Health. 2020; 17(11):4105. https://doi.org/10.3390/ijerph17114105
Chicago/Turabian StyleSiegel, Marte L., Eva M. Gullestad Binder, Hanne Sofie J. Dahl, Nikolai O. Czajkowski, Kenneth L. Critchfield, Per A. Høglend, and Randi Ulberg. 2020. "Therapeutic Atmosphere in Psychotherapy Sessions" International Journal of Environmental Research and Public Health 17, no. 11: 4105. https://doi.org/10.3390/ijerph17114105
APA StyleSiegel, M. L., Gullestad Binder, E. M., Dahl, H. S. J., Czajkowski, N. O., Critchfield, K. L., Høglend, P. A., & Ulberg, R. (2020). Therapeutic Atmosphere in Psychotherapy Sessions. International Journal of Environmental Research and Public Health, 17(11), 4105. https://doi.org/10.3390/ijerph17114105