Children’s Respiratory Infections in Tianjin Area, China: Associations with Home Environments and Lifestyles



Abstract

1. Introduction
2. Materials and Methods
2.1. Questionnaire and Population
- Has your child ever had croup? (possible responses: yes; no)
- Has your child ever had doctor diagnosed pneumonia? (possible responses: yes; no)
- Has your child ever had ear infections? (possible responses: no; yes, 1–2 times; yes, 3–5 times; yes, >5 times)
- In the last 12 months, how many times did your child have a common cold? (possible responses: none; 1–2 times; 3–5 times; 6–10 times; >10 times)
2.2. Statistical Analysis
3. Results
3.1. Demographic Information and Respiratory Infections in Children
3.2. Home Environmental Factors Related to Respiratory Infections
3.2.1. Dampness, Odors and Respiratory Infections
- (1)
- Visible mold in child’s room;
- (2)
- Visible damp in child’s room;
- (3)
- Suspected moisture problem in child’s home;
- (4)
- Peeling or discolored floor covering in child’s room;
- (5)
- Flooding in child’s room;
- (6)
- Condensation on windowpane in winter in child’s room;
- (7)
- Perceived moldy odor;
- (8)
- Perceived dry air.
3.2.2. Building Characteristics and Respiratory Infections
3.2.3. Environmental Tobacco Smoke Exposure, Pet-Keeping and Respiratory Infections
3.3. Lifestyle Factors Related to Respiratory Infections
3.3.1. Daycare Attendance and Respiratory Infections
3.3.2. Food Habits, Outdoor Activity, Cleaning Habits and Respiratory Infections
3.4. Biological Factors
3.5. Multivariate Regression Model and Population Attributable Fraction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CCHH | China, Children, Homes and Health |
| TB | Tuberculosis |
| ETS | Environmental tobacco smoke |
| PAF | Population attributable fractions |
| AC | Air conditioner |
| AOR | Adjusted odds ratio |
| CI | Confidence interval |
| PM10 | Particles smaller than 10 microns |
| PVC | Poly vinyl chloride |
References
- World Health Statistics 2018: Monitoring Health for the SDGs, Sustainable Development Goals. Available online: www.who.int/gho/publications/world_health_statistics/en/ (accessed on 3 April 2020).
- UNICEF; WHO; World Bank & UN-DESA Population Division. Levels & Trends in Child Mortality Report 2018. 2018. Available online: https://childmortality.org/reports (accessed on 3 April 2020).
- Wong, G.W.K.; Hui, D.S.C.; Chan, H.H.; Fok, T.F.; Leung, R.; Zhong, N.S.; Chen, Y.Z.; Lai, C.K.W. Prevalence of respiratory and atopic disorders in Chinese schoolchildren. Clin. Exp. Allergy 2001, 31, 1225–1231. [Google Scholar] [CrossRef]
- Leech, J.A.; Nelson, W.C.; Burnett, R.T.; Aaron, S.; Raizenne, M.E. It’s about time: A comparison of Canadian and American time-activity patterns. J. Expo. Anal. Environ. Epidemiol. 2002, 12, 427–432. [Google Scholar] [CrossRef]
- Brasche, S.; Bischof, W. Daily time spent indoors in German homes-Baseline data for the assessment of indoor exposure of German occupants. Int. J. Hyg. Environ. Health 2006, 208, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Mizgerd, J.P. Lung infection-A public health priority. PLoS Med. 2006, 3, e76. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.H.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef]
- Bornehag, C.G.; Sundell, J.; Sigsgaard, T. Dampness in buildings and health (DBH): Reports from an ongoing epidemiological investigation on the association between indoor environmental factors and health effects among children in Sweden. Indoor Air 2004, 14, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Sundell, J.; Li, B.Z.; Zhang, Y.P. China, Children, Homes, Health (CCHH). Chin. Sci. Bull. 2013, 58, 4179–4181. [Google Scholar] [CrossRef]
- Sun, Y.X.; Hou, J.; Sheng, Y.; Kong, X.; Weschler, L.B.; Sundell, J. Modern life makes children allergic. A cross-sectional study: Associations of home environment and lifestyles with asthma and allergy among children in Tianjin region, China. Int. Arch. Occup. Environ. Health 2019, 92, 587–589. [Google Scholar] [CrossRef]
- Tham, K.W.; Zuraimi, M.S.; Koh, D.; Chew, F.T.; Ooi, P.L. Association between home dampness and presence of molds with asthma and allergic symptoms among young children in the tropics. Pediatric Allergy Immunol. 2010, 18, 418–424. [Google Scholar] [CrossRef]
- Tsao, Y.C.; Hwang, Y.H. Impact of a water-damaged indoor environment on kindergarten student absences due to upper respiratory infection. Build. Environ. 2013, 64, 1–6. [Google Scholar] [CrossRef]
- Kennedy, K.; Grimes, C. Indoor water and dampness and the health effects on children: A review. Curr. Allergy Asthma Rep. 2013, 13, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Mendell, M.J.; Mirer, A.G.; Cheung, K.; Tong, M.; Douwes, J. Respiratory and allergic health effects of dampness, mold, and dampness-related agents: A Review of the epidemiologic evidence. Environ. Health Perspect. 2011, 119, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Fisk, W.J.; Eliseeva, E.A.; Mendell, M.J. Association of residential dampness and mold with respiratory tract infections and bronchitis: A meta-analysis. Environ. Health 2010, 9, 72. [Google Scholar] [CrossRef]
- Bronswijk, J.E.M.H.V. House Dust Biology for Allergists, Acarologists and Mycologists; NIB Publisher: Zeist, The Netherlands, 1981. [Google Scholar]
- Waegemaekers, M.; Wageningen, N.V.; Brunekreef, B.; Boleij, J.S. Respiratory symptoms in damp homes—A pilot study. Allergy 2010, 44, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.H.; Cao, Y.; Ding, H.L.; Ma, Y.N.; Jin, J.; Zhao, Y.D.; He, Q.C. Effects of environmental tobacco smoke on respiratory health of boys and girls from kindergarten: Results from 15 districts of northern China. Indoor Air 2010, 17, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Mendell, M.J. Indoor residential chemical emissions as risk factors for respiratory and allergic effects in children: A review. Indoor Air 2007, 17, 259–277. [Google Scholar] [CrossRef]
- Nesti, M.M.; Goldbaum, M. Infectious diseases and daycare and preschool education. J. Pediatric 2007, 83, 299–312. [Google Scholar] [CrossRef]
- Yang, Z.; Qian, H.; Zheng, X.; Huang, C.; Zhang, Y.; Zhang, M.; Li, B.; Zhao, Z.; Deng, Q.; Yang, X.; et al. Residential risk factors for childhood pneumonia: A cross-sectional study in eight cities of China. Environ. Int. 2018, 116, 83–91. [Google Scholar]
- Holberg, C.J.; Wright, A.L.; Martinez, F.D.; Morgan, W.J.; Taussig, L.M. Child day care, smoking by caregivers, and lower respiratory tract illness in the first 3 years of life. Group health Medical Associates. Pediatrics 1993, 91, 885–892. [Google Scholar]
- Sun, Y.X.; Sundell, J. Early daycare attendance increase the risk for respiratory infections and asthma of children. J. Asthma 2011, 48, 790–796. [Google Scholar] [CrossRef]
- Louhiala, P.J.; Jaakkola, N.; Ruotsalainen, R.; Jaakkola, J.J. Form of day care and respiratory infections among Finnish children. Am. J. Public Health 1995, 85 Pt 1, 1109–1112. [Google Scholar] [CrossRef]
- Hardy, A.M.; Fowler, M.G. Child care arrangements and repeated ear infections in young children. Am. J. Public Health 1993, 83, 1321–1325. [Google Scholar] [CrossRef] [PubMed]
- Bosch, A.A.T.M.; Levin, E.; Van Houten, M.A.; Hasrat, R.; Kalkman, G.; Biesbroek, G.; de Piters, W.A.A.S.; de Groot, P.C.M.; Pernet, P.; Keijser, B.J.F.; et al. Development of upper respiratory tract microbiota in infancy is affected by mode of delivery. EBioMedicine 2016, 9, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Barros, A.J.D.; The WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed country: A pooled analysis. Lancet 2000, 355, 451–455. [Google Scholar]
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess. 2007, 153, 1. [Google Scholar]
- Arifeen, S.; Black, R.E.; Antelman, G.; Baqui, A.; Caulfield, L.; Becker, S. Exclusive breastfeeding reduces acute respiratory infection and diarrhea deaths among infants in Dhaka Slums. Pediatrics 2001, 108, e67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Mo, J.; Weschler, C.J. Reducing health risks from indoor exposures in rapidly developing urban China. Environ. Health Perspect. 2013, 121, 751–755. [Google Scholar] [CrossRef]
- Hou, J.; Zhang, Y.F.; Sun, Y.X.; Wang, P.; Zhang, Q.; Kong, X.; Sundell, J. Air change rates at night in northeast Chinese homes. Build. Environ. 2018, 132, 273–281. [Google Scholar] [CrossRef]
- Zhang, Y.P.; Li, B.Z.; Huang, C.; Yang, X.; Qian, H.; Deng, Q.; Zhao, Z.; Li, A.; Zhao, J.; Zhang, X.; et al. Ten cities cross-sectional questionnaire survey of children asthma and other allergies in China. Chin. Sci. Bull. 2013, 58, 4182–4189. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. 2018. Available online: http://data.Stats.gov.cn/search.htm?s=GDP (accessed on 3 April 2020).
- Meteorological Data Center of China Meteorological Administration. Statistics of Monthly Average Temperature. 2017. Available online: http://data.cma.cn/data/weatherBk.html (accessed on 3 April 2020).
- Rockhill, B.; Newman, B.; Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998, 88, 15–19. [Google Scholar] [CrossRef]
- Lumbiganon, P.; Laopaiboon, M.; Gülmezoglu, A.M.; Souza, J.P.; Taneepanichskul, S.; Ruyan, P.; Attygalle, D.E.; Shrestha, N.; Mori, R.; Nguyen, D.H.; et al. Method of delivery and pregnancy outcomes in Asia: The WHO global survey on maternal and perinatal health 2007-08. Lancet 2010, 375, 490–499. [Google Scholar] [CrossRef]
- Althabe, F.; José, M.B. Caesarean Section: The Paradox. Lancet 2006, 368, 1472–1473. [Google Scholar] [CrossRef]
- Wang, L.X.; Zhao, B.; Liu, C.; Lin, H.; Yang, X.; Zhang, Y. Indoor SVOC pollution in China: A review. Chin. Sci. Bull. 2010, 55, 1469–1478. [Google Scholar] [CrossRef]
- Park, J.S.; Ikeda, K. Variations of formaldehyde and VOC levels during 3 years in new and older homes. Indoor Air 2010, 16, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.H.; Sun, Y.X.; Zhang, Q.N.; Hou, J.; Wang, P.; Kong, X.; Sundell, J. Phthalate exposure in Chinese homes and its association with household consumer products. Sci. Total Environ. 2020, 719, 136965. [Google Scholar] [CrossRef] [PubMed]
- Tanner, E.M.; Hallerback, M.U.; Wikstrom, S.; Lindh, C.; Kiviranta, H.; Gennings, C.; Bornehag, C.-G. Early prenatal exposure to suspected endocrine disruptor mixtures is associated with lower IQ at age seven. Environ. Int. 2020, 134, 105185. [Google Scholar] [CrossRef]
- Shu, H.; Wikstrom, S.; Jonsson BA, G.; Lindh, C.H.; Svensson, Å.; Nånberg, E.; Bornehag, C.-G. Prenatal phthalate exposure was associated with croup in Swedish infants. Acta Paediatr. 2018, 107, 1011–1019. [Google Scholar] [CrossRef]
- Sundell, J.; Lindvall, T. Indoor air humidity and sensation of dryness as risk indicators of SBS. Indoor Air 1993, 3, 382–390. [Google Scholar] [CrossRef]
- Andersen, I.; Lundqvist, G.R.; Jensen, P.L.; Proctor, D.F. Human response to 78-h exposure to dry air. Arch. Environ. Health 1974, 29, 319–324. [Google Scholar] [CrossRef]
- Sun, Y.X.; Hou, J.; Cheng, R.S.; Sheng, Y.; Zhang, X.; Sundell, J. Indoor air quality, ventilation and their associations with sick building syndrome in Chinese homes. Energy Build. 2019, 197, 112–119. [Google Scholar] [CrossRef]
- Emenius, G.; Svartengren, M.; Korsgaard, J.; Nordvall, L.; Pershagen, G.; Wickman, M. Building characteristics, indoor air quality and recurrent wheezing in very young children (BAMSE). Indoor Air 2004, 14, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Brundage, J.F. Building-associated risk of febrile acute respiratory diseases in army trainees. JAMA 1988, 259, 2108–2112. [Google Scholar] [CrossRef] [PubMed]
- Milton, D.K.; Glencross, P.M.; Walters, M.D. Risk of sick leave associated with outdoor air supply rate, humidification, and occupant complaints. Indoor Air 2001, 10, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.X.; Wang, Z.G.; Zhang, Y.F.; Sundell, J. In China, students in crowded dormitories with a low ventilation rate have more common colds: Evidence for airborne transmission. PLoS ONE 2011, 6, e27140. [Google Scholar] [CrossRef]
- Fleming, D.W.; Cochi, S.L.; Hightower, A.W.; Broome, C.V. Childhood upper respiratory tract infections: To what degree is incidence affected by day-care attendance? Pediatrics 1987, 79, 55–60. [Google Scholar]
- Strangert, K. Respiratory illness in preschool children with different forms of day care. Pediatrics 1976, 57, 191. [Google Scholar]
- Smedje, G.; Wang, J.; Norback, D.; Nilsson, H.; Engvall, K. SBS symptoms in relation to dampness and ventilation in inspected single-family houses in Sweden. Int. Arch. Occup. Environ. Health 2017, 90, 703–711. [Google Scholar] [CrossRef]
- Henrickson, K.J. Viral pneumonia in children. Semin. Pediatric Infect. Dis. 1998, 9, 217–233. [Google Scholar] [CrossRef]
- Peltola, V.; Waris, M.; Österback, R.; Susi, P.; Ruuskanen, O.; Hyypiä, T. Rhinovirus transmission within families with children: Incidence of symptomatic and asymptomatic infections. J. Infect. Dis. 2008, 197, 382–389. [Google Scholar] [CrossRef]
- Heikkinen, T.; Järvinen, A. The common cold. Lancet 2003, 361, 51–59. [Google Scholar] [CrossRef]
- Jaakkola, J.J.; Heinonen, O.P. Shared office space and the risk of the common cold. Eur. J. Epidemiol. 1995, 11, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Hoge, C.W.; Reichler, M.R.; Dominguez, E.A.; Bremer, J.C.; Mastro, T.D.; Hendricks, K.A.; Musher, D.M.; Elliott, J.A.; Facklam, R.R.; Breiman, R.F. An epidemic of pneumococcal disease in an overcrowded, inadequately ventilated jail. N. Engl. J. Med. 1994, 331, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Qu, F.; Weschler, L.B.; Sun, Y.X.; Sundell, J. High pneumonia lifetime-ever incidence in Beijing children compared with locations in other countries, and implications for national PCV and Hib vaccination. PLoS ONE 2017, 12, e171438. [Google Scholar] [CrossRef] [PubMed]
- Norbäck, D.; Lu, C.; Zhang, Y.P.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y.; Sundell, J.; et al. Lifetime-ever pneumonia among pre-school children across China-Associations with pre-natal and post-natal early life environmental factors. Environ. Res. 2018, 167, 418–427. [Google Scholar] [CrossRef]

{kind=link}
| Croup | Pneumonia | Ear Infection | Common Cold >2 Times | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Lifetime-Ever Incidence | p-Value a | Lifetime-Ever Incidence | p-Value | Lifetime-Ever Incidence | p-Value | Incidence Per Year | p-Value | ||
| Total | 625 (9.2) | / | 1959 (28.7) | / | 794 (11.6) | / | 2044 (31.3) | / | |
| Gender | |||||||||
| Male | 364 (10.4) | 0.000 | 1043 (29.8) | 0.064 | 411 (11.7) | 0.707 | 1059 (31.8) | 0.445 | |
| Female | 254 (7.9) | 898 (27.8) | 373 (11.4) | 964 (30.9) | |||||
| Age | |||||||||
| 0–2 | 21 (10.0) | 0.755 | 52 (24.0) | 0.227 | 9 (4.3) | 0.001 | 70 (36.5) | 0.000 | |
| 3–5 | 268 (8.9) | 878 (29.3) | 378 (12.5) | 1112 (38.8) | |||||
| 6–8 | 336 (9.4) | 1029 (28.6) | 407 (11.2) | 862 (24.9) | |||||
| Family allergic history | |||||||||
| Yes | 156 (26.9) | 0.000 | 421 (45.3) | 0.000 | 176 (19.1) | 0.000 | 392 (43.8) | 0.000 | |
| No | 433 (7.8) | 1436 (25.8) | 584 (10.4) | 1575 (29.7) | |||||
| Home location | |||||||||
| Urban | 375 (11.0) | 0.000 | 1202 (35.2) | 0.000 | 545 (16.0) | 0.000 | 1137 (33.8) | 0.000 | |
| Suburban | 107 (7.7) | 333 (23.8) | 130 (9.2) | 406 (30.2) | |||||
| Rural | 105 (6.5) | 331 (20.5) | 75 (4.5) | 387 (26.3) | |||||
| Annual household income, $ | |||||||||
| <4225 | 89 (8.7) | 239 (23.1) | 73 (7.0) | 219 (23.0) | |||||
| 4225–7041 | 101 (7.2) | 380 (27.0) | 121 (8.5) | 383 (28.6) | |||||
| 7042–14,082 | 163 (9.1) | 597 (33.3) | 242 (13.4) | 612 (35.2) | |||||
| 14,083–28,164 | 159 (11.8) | 516 (38.3) | 189 (14.1) | 457 (34.8) | |||||
| >28,164 | 69 (12.5) | 0.000 | 202 (35.9) | 0.000 | 94 (16.8) | 0.000 | 199 (36.4) | 0.000 | |
| Adjusted Odds Ratio (AOR), 95% Confidence Interval (CI) | ||||
|---|---|---|---|---|
| Croup | Pneumonia | Ear Infection | Common Cold >2 Times | |
| Mold spot in child’s room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.42 (1.64, 3.56) | 1.23 (0.90, 1.69) | 1.52 (1.01, 2.30) | 1.42 (1.03, 1.94) |
| Damp spot in child’s room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.06 (1.46, 2.89) | 1.34 (1.03, 1.73) | 1.64 (1.16, 2.32) | 1.25 (0.96, 1.62) |
| Suspected moisture in room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.56 (1.23, 1.97) | 1.48 (1.26, 1.73) | 1.46 (1.18, 1.81) | 1.30 (1.10, 1.52) |
| Floor moisture in child’s room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.61 (1.10, 2.37) | 1.37 (1.04, 1.80) | 1.34 (0.92, 1.95) | 1.40 (1.06, 1.85) |
| Flooding in child’s room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.76 (0.95, 3.28) | 1.53 (0.95, 2.48) | 1.40 (0.75, 2.59) | 1.45 (0.88, 2.37) |
| Condensation on the windowpane in child’s room | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.53 (1.23, 1.91) | 1.34 (1.16, 1.55) | 1.09 (0.88, 1.34) | 1.60 (1.38, 1.84) |
| Perceived moldy odor in home | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.72 (1.35, 2.20) | 1.34 (1.13, 1.59) | 1.81 (1.44, 2.28) | 1.24 (1.04, 1.48) |
| Perceived dry air in home | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.41 (1.16, 1.71) | 1.28 (1.14, 1.45) | 1.32 (1.11, 1.57) | 1.43 (1.27, 1.62) |
| Adjusted Odds Ratio (AOR), 95% Confidence Interval (CI) | ||||
|---|---|---|---|---|
| Croup | Pneumonia | Ear Infection | Common Cold > 2 Times | |
| Fruit consumption | ||||
| Occasionally/never | 1.00 | 1.00 | 1.00 | 1.00 |
| ≥once/week | 0.60 (0.32, 1.13) | 0.70 (0.45, 1.08) | 0.65 (0.34, 1.21) | 1.35 (0.80, 2.25) |
| Fast food consumption | ||||
| Occasionally/never | 1.00 | 1.00 | 1.00 | 1.00 |
| ≥once/week | 1.09 (0.85, 1.40) | 1.08 (0.92, 1.27) | 1.05 (0.84, 1.32) | 0.96 (0.81, 1.13) |
| Watching TV | ||||
| <3 h per day | 1.00 | 1.00 | 1.00 | 1.00 |
| ≥3 h per day | 1.37 (0.97, 1.94) | 1.09 (0.86, 1.38) | 1.18 (0.83, 1.68) | 1.39 (1.10, 1.75) |
| Outdoor activity | ||||
| ≤2 times per week | 1.00 | 1.00 | 1.00 | 1.00 |
| >2 times per week | 1.18 (0.97, 1.43) | 0.94 (0.83, 1.06) | 1.00 (0.84, 1.19) | 1.03 (0.91, 1.16) |
| Cleaning room | ||||
| Everyday | 1.00 | 1.00 | 1.00 | 1.00 |
| Less than everyday | 1.09 (0.89, 1.33) | 1.12 (0.98, 1.27) | 1.46 (1.22, 1.73) | 1.13 (0.99, 1.29) |
| Opening window | ||||
| Everyday | 1.00 | 1.00 | 1.00 | 1.00 |
| Less than everyday | 1.00 (0.67, 1.50) | 1.04 (0.81, 1.33) | 0.76 (0.50, 1.15) | 1.01 (0.78, 1.30) |
| Sun-curing bed sheets | ||||
| Often | 1.00 | 1.00 | 1.00 | 1.00 |
| Not often | 1.28 (1.04, 1.57) | 1.46 (1.28, 1.65) | 1.53 (1.27, 1.85) | 1.28 (1.13, 1.45) |
| Adjusted Odds Ratio (AOR), 95% Confidence Interval (CI) | ||||
|---|---|---|---|---|
| Croup | Pneumonia | Ear Infection | Common Cold >2 Times | |
| Way of delivery | ||||
| Natural | 1.00 | 1.00 | 1.00 | 1.00 |
| cesarean | 1.22 (1.00, 1.48) | 1.28 (1.13, 1.44) | 1.25 (1.04, 1.49) | 0.96 (0.85, 1.09) |
| Period of breastfeeding | ||||
| >6 months | 1.00 | 1.00 | 1.00 | 1.00 |
| <6 months | 1.08 (0.88, 1.33) | 1.12 (0.98, 1.28) | 1.07 (0.89, 1.29) | 0.87 (0.76, 1.00) |
| Born on due week | ||||
| Yes | 1.00 | 1.00 | 1.00 | 1.00 |
| No | 1.16 (0.96, 1.41) | 1.28 (1.13, 1.45) | 1.07 (0.90, 1.27) | 0.98 (0.87, 1.12) |
| Birth weight | ||||
| >2.5 kg | 1.00 | 1.00 | 1.00 | 1.00 |
| <2.5 kg | 0.91 (0.58, 1.42) | 1.33 (1.03, 1.71) | 1.30 (0.91, 1.86) | 1.11 (0.85, 1.45) |
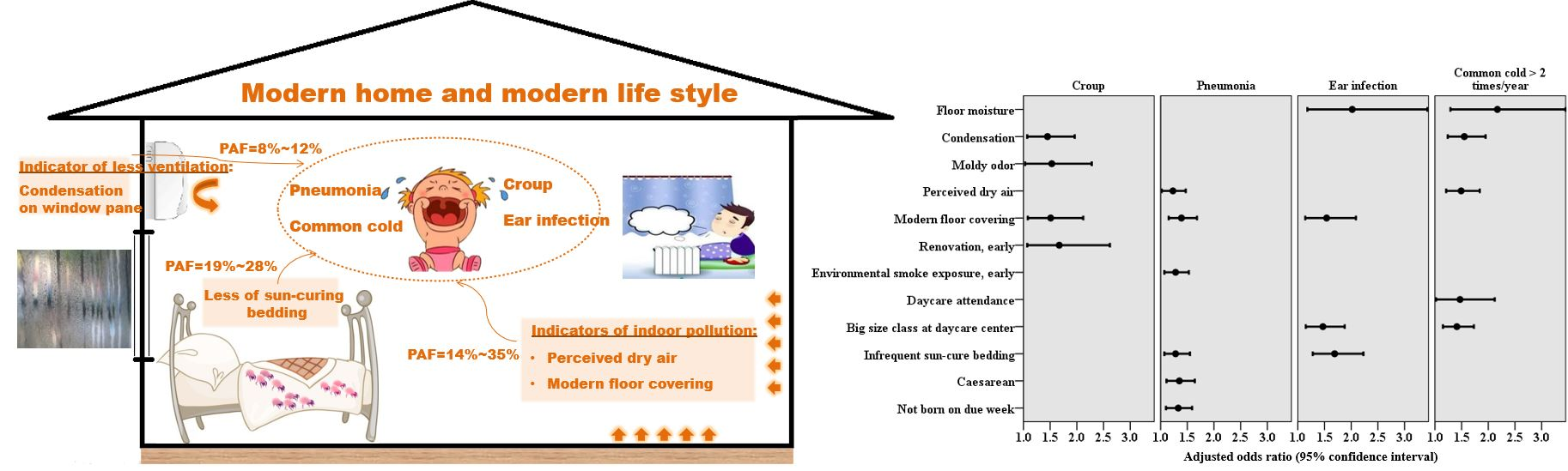
| Adjusted Odds Ratio (AOR), 95% Confidence Interval (CI) | ||||
|---|---|---|---|---|
| Croup | Pneumonia | Ear Infection | Common Cold >2 Times m | |
| Floor moisture a | 2.02 (1.18, 3.43) | 2.17 (1.29, 3.64) | ||
| Condensation b | 1.45 (1.07, 1.96) | 1.55 (1.24, 1.94) | ||
| Perceived moldy odor c | 1.53 (1.03, 2.28) | |||
| Perceived dry air d | 1.23 (1.02, 1.47) | 1.49 (1.21, 1.84) | ||
| Modern floor covering e | 1.51 (1.08, 2, 12) | 1.39 (1.15, 1.68) | 1.54 (1.14, 2.09) | |
| Renovation, early f | 1.67 (1.07, 2.62) | |||
| Environmental tobacco smoke (ETS) exposure, early g | 1.28 (1.07, 1.53) | |||
| Daycare attendance h | 1, 47 (1.02, 2.12) | |||
| Size of daycare center i | 1.47 (1.15, 1.88) | 1.41 (1.15, 1.73) | ||
| Sun-curing bedding j | 1.28 (1.07, 1.55) | 1.69 (1.28, 2.23) | ||
| Cesarean delivery k | 1.35 (1.11, 1.64) | |||
| Born on due week l | 1.33 (1.10, 1.59) | |||
| Croup, % | Pneumonia, % | Ear Infection, % | Common Cold >2 Times a, % | |
|---|---|---|---|---|
| Floor moisture | 0.9 | 1.4 | ||
| Condensation | 12.2 | 8.4 | ||
| Perceived moldy odor | 7.6 | |||
| Perceived dry air | 13.9 | 15.0 | ||
| Modern floor covering | 14.7 | 18.3 | 34.5 | |
| Renovation, early | 4.2 | |||
| Environmental tobacco smoke (ETS) exposure, early | 4.5 | |||
| Childcare at daycare center | 14.8 | |||
| High occupancy daycare center | 11.8 | 9.0 | ||
| Infrequent sun-curing bedding | 18.7 | 28.4 | ||
| Cesarean delivery | 13.8 | |||
| Not born on due week | 7.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, J.; Lv, D.; Sun, Y.; Wang, P.; Zhang, Q.; Sundell, J. Children’s Respiratory Infections in Tianjin Area, China: Associations with Home Environments and Lifestyles. Int. J. Environ. Res. Public Health 2020, 17, 4069. https://doi.org/10.3390/ijerph17114069
Hou J, Lv D, Sun Y, Wang P, Zhang Q, Sundell J. Children’s Respiratory Infections in Tianjin Area, China: Associations with Home Environments and Lifestyles. International Journal of Environmental Research and Public Health. 2020; 17(11):4069. https://doi.org/10.3390/ijerph17114069
Chicago/Turabian StyleHou, Jing, Dachao Lv, Yuexia Sun, Pan Wang, Qingnan Zhang, and Jan Sundell. 2020. "Children’s Respiratory Infections in Tianjin Area, China: Associations with Home Environments and Lifestyles" International Journal of Environmental Research and Public Health 17, no. 11: 4069. https://doi.org/10.3390/ijerph17114069
APA StyleHou, J., Lv, D., Sun, Y., Wang, P., Zhang, Q., & Sundell, J. (2020). Children’s Respiratory Infections in Tianjin Area, China: Associations with Home Environments and Lifestyles. International Journal of Environmental Research and Public Health, 17(11), 4069. https://doi.org/10.3390/ijerph17114069