Musculoskeletal Symptoms among Stone, Sand and Gravel Mine Workers and Associations with Sociodemographic and Job-Related Factors


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Sociodemographic Characteristics
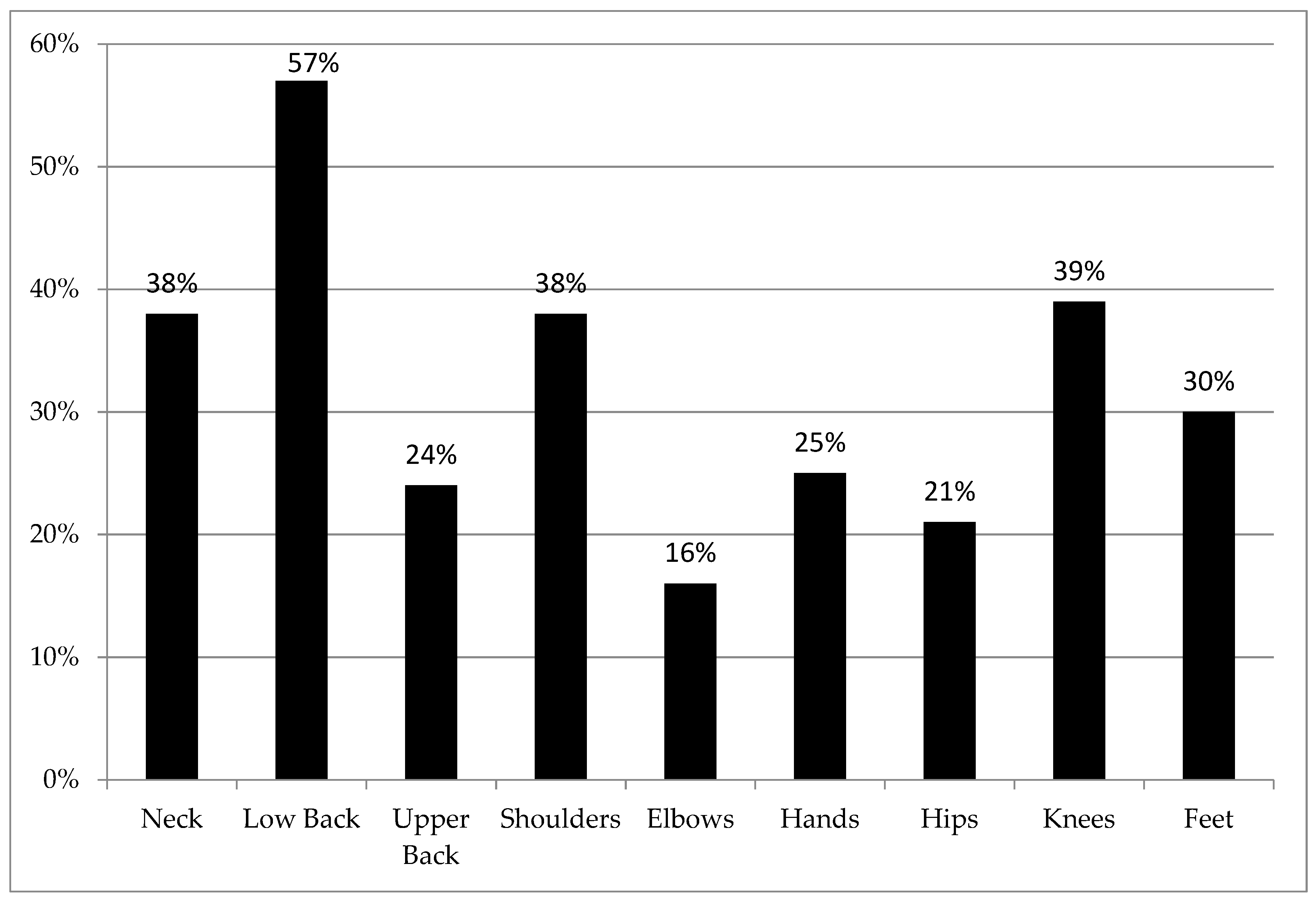
3.2. Prevalence
3.3. Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burdorf, A.; Sorock, G. Positive and negative evidence of risk factors for back disorders. Scand. J. Work. Environ. Health 1997, 23, 243–256. [Google Scholar] [CrossRef]
- Xu, G.; Pang, D.; Liu, F.; Pei, D.; Wang, S.; Li, L. Prevalence of low back pain and associated occupational factors among Chinese coal miners. BMC Public Health 2012, 12, 149. [Google Scholar] [CrossRef] [PubMed]
- BLS. Injuries, Illnesses, and Fatalities Data. Available online: https://www.bls.gov/iif/soii-chart-data-2018.htm (accessed on 1 April 2020).
- Skandfer, M.; Talykova, L.; Brenn, T.; Nilsson, T.; Vaktskjold, A. Low back pain among mineworkers in relation to driving, cold environment and ergonomics. Ergon. 2014, 57, 1541–1548. [Google Scholar] [CrossRef]
- De Sousa, M.N.A.; Santos, B.M.D.O.; Zaia, J.E.; Bertoncello, D.; Feitosa, A.D.N.A.; De Assis, E.V.; Batista, H.M.T.; Monteiro, C.B.D.M.; Maia, P.C.G.G.S.; Quemelo, P.R.V.; et al. Musculoskeletal Disorders In Informal Mining Workers. Int. Arch. Med. 2015, 8, 183. [Google Scholar] [CrossRef]
- Custodio, B.P.; Matias, A.C.; Soriano, V.J. Work-Related Musculoskeletal Symptoms Among Small Scale Gold Miners and Extraction Workers in the Philippines. In Advances in Intelligent Systems and Computing; Springer Science and Business Media LLC: Berlin, Germany, 2016; Volume 491, pp. 495–501. [Google Scholar]
- Rehn, B.; Bergdahl, I.; Ahlgren, C.; From, C.; Järvholm, B.; Lundström, R.; Nilsson, T.; Sundelin, G. MUSCULOSKELETAL SYMPTOMS AMONG DRIVERS OF ALL-TERRAIN VEHICLES. J. Sound Vib. 2002, 253, 21–29. [Google Scholar] [CrossRef]
- Waters, T.; Genaidy, A.; Viruet, H.B.; Makola, M. The impact of operating heavy equipment vehicles on lower back disorders. Ergon. 2008, 51, 602–636. [Google Scholar] [CrossRef]
- Kim, J.H.; Marin, L.S.; Dennerlein, J. Evaluation of commercially available seat suspensions to reduce whole body vibration exposures in mining heavy equipment vehicle operators. Appl. Ergon. 2018, 71, 78–86. [Google Scholar] [CrossRef]
- McPhee, B. Ergonomics in mining. Occup. Med. 2004, 54, 297–303. [Google Scholar] [CrossRef]
- Eiter, B.; Bellanca, J.; Helfrich, W.; Orr, T.; Hrica, J.; Macdonald, B.; Navoyski, J. Recognizing Mine Site Hazards: Identifying Differences in Hazard Recognition Ability for Experienced and New Mineworkers. In Proceedings of the Advances in Intelligent Systems and Computing, Los Angeles, CA, USA, 17–21 July 2017; Volume 591, pp. 104–115. [Google Scholar]
- Burke, M.J.; Salvador, R.O.; Smith-Crowe, K.; Chan-Serafin, S.; Smith, A.; Sonesh, S. The dread factor: How hazards and safety training influence learning and performance. J. Appl. Psychol. 2011, 96, 46–70. [Google Scholar] [CrossRef]
- NIOSH. Mining Facts-2015. Available online: https://www.cdc.gov/niosh/mining/works/statistics/factsheets/miningfacts2015.html (accessed on 2 April 2020).
- Weston, E.; Nasarwanji, M.; Pollard, J.P. Identification of Work-Related Musculoskeletal Disorders in Mining. J. Saf. Health Environ. Res. 2016, 12, 274–283. [Google Scholar]
- NIOSH. MSHA Data File Downloads. Accident / Injury / Illness Files. Available online: www.cdc.gov/niosh/mining/data/default.html (accessed on 2 April 2020).
- Nasarwanji, M.F.; Mayton, A.G.; Pollard, J. Why Slips, Trips, and Falls Are Still A Problem: A Hazard Assessment At Surface Mines. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting; SAGE Publications: Thousand Oaks, CA, USA, 2019; Volume 63, pp. 1856–1860. [Google Scholar]
- Nasarwanji, M.; Sun, K. Burden associated with nonfatal slip and fall injuries in the surface stone, sand, and gravel mining industry. Saf. Sci. 2019, 120, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Battelle Centers for Public Health Research and Evaluation. Analysis of the mine safety and health administration (MSHA) accident/injury database. In Work Authorization Number 2837-16 Phase III Report; United States Department of Health and Human Services: Washington, DC, USA, 1999. [Google Scholar]
- Hildebrandt, V.H.; Bongers, P.M.; Van Dijk, F.J.H.; Kemper, H.C.G.; Dul, J. Dutch Musculoskeletal Questionnaire: Description and basic qualities. Ergonomics 2001, 44, 1038–1055. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2009, 53, 285–323. [Google Scholar] [CrossRef] [PubMed]
- Forde, M.; Punnett, L.; Wegmann, D.H. Prevalence of musculoskeletal disorders in union ironworkers. J. Occup. Environ. Hyg. 2005, 2, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Tinubu, B.M.; Mbada, C.E.; Oyeyemi, A.; A Fabunmi, A. Work-Related Musculoskeletal Disorders among Nurses in Ibadan, South-west Nigeria: A cross-sectional survey. BMC Musculoskelet. Disord. 2010, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Widanarko, B.; Legg, S.; Stevenson, M.A.; Devereux, J.; Eng, A.; Mannetje, A.; Cheng, S.; Douwes, J.; Ellison-Loschmann, L.; McLean, D.; et al. Prevalence of musculoskeletal symptoms in relation to gender, age, and occupational/industrial group. Int. J. Ind. Ergon. 2011, 41, 561–572. [Google Scholar] [CrossRef]
- Dianat, I.; Bazazan, A.; Azad, M.A.S.; Salimi, S.S. Work-related physical, psychosocial and individual factors associated with musculoskeletal symptoms among surgeons: Implications for ergonomic interventions. Appl. Ergon. 2018, 67, 115–124. [Google Scholar] [CrossRef]
- Bovenzi, M.; Pinto, I.; Stacchini, N. Low Back Pain in Port Machinery Operators. J. Sound Vib. 2002, 253, 3–20. [Google Scholar] [CrossRef]
- Leroux, I.; E Dionne, C.; Bourbonnais, R.; Brisson, C. Prevalence of musculoskeletal pain and associated factors in the Quebec working population. Int. Arch. Occup. Environ. Health 2005, 78, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, E.C.; Stathi, I.-C.; Charizani, F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet. Disord. 2004, 5, 16. [Google Scholar] [CrossRef]
- He, Y.; Hu, J.; Yu, I.T.S.; Gu, W.; Liang, Y.-X. Determinants of Return to Work After Occupational Injury. J. Occup. Rehabil. 2010, 20, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Trinkoff, A.M.; Le, R.; Geiger-Brown, J.; Lipscomb, J.; Lang, G. Longitudinal relationship of work hours, mandatory overtime, and on-call to musculoskeletal problems in nurses. Am. J. Ind. Med. 2006, 49, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Mehrdad, R.; Dennerlein, J.; Morshedizadeh, M. Musculoskeletal disorders and ergonomic hazards among Iranian physicians. Arch. Iran. Med. 2012, 15, 370–374. [Google Scholar] [PubMed]
- Bodhare, T.; Valsangkar, S.; Bele, S. An Epidemiological Study of Work-Related Musculoskeletal Disorders Among Construction Workers in Karimnagar, Andhra Pradesh. Indian J. Community Med. 2011, 36, 304–307. [Google Scholar] [CrossRef]
- Hignett, S.; McAtamney, L. Rapid entire body assessment (REBA). Appl. Ergon. 2000, 31, 201–205. [Google Scholar] [CrossRef]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Haas, E.J.; Hoebbel, C.L.; Yorio, P.L. Assessing the Impact of Safety Climate Constructs on Worker Performance in the Mining Industry; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH): Pittsburgh, PA, USA, 2020.
- Yan, X.; Li, H.; Li, A.R.; Zhang, H. Wearable IMU-based real-time motion warning system for construction workers’ musculoskeletal disorders prevention. Autom. Constr. 2017, 74, 2–11. [Google Scholar] [CrossRef]
- Punnett, L.; Warren, N.; Henning, R.; Nobrega, S.; Cherniack, M. Participatory Ergonomics as a Model for Integrated Programs to Prevent Chronic Disease. J. Occup. Environ. Med. 2013, 55, S19–S24. [Google Scholar] [CrossRef]
- Carr, L.; Leonhard, C.; Tucker, S.J.; Fethke, N.; Benzo, R.; Gerr, F.; Information, P.E.K.F.C. Total Worker Health Intervention Increases Activity of Sedentary Workers. Am. J. Prev. Med. 2016, 50, 9–17. [Google Scholar] [CrossRef]
- Nobrega, S.; Kernan, L.; Plaku-Alakbarova, B.; Robertson, M.; Warren, N.; Henning, R. CPH-NEW Research Team Field tests of a participatory ergonomics toolkit for Total Worker Health. Appl. Ergon. 2017, 60, 366–379. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Mean (SD)/Frequency (%) |
|---|---|
| Age | 45 (14) |
| Sex | |
| Male | 423 (93%) |
| Female | 31 (7%) |
| Education | |
| Some High School | 43 (9.5%) |
| High School Graduate/GED | 188 (41.3%) |
| Some College or Technical/Vocational Training | 130 (28.6%) |
| Associate degree | 44 (9.7%) |
| Bachelor’s degree | 39 (8.6%) |
| Master’s degree | 8 (1.8%) |
| Race | |
| African American/Black | 4 (0.9%) |
| American Indian/Alaskan Native | 1 (0.2%) |
| Asian/Asian American | 1 (0.2%) |
| Hispanic, Latino/a/x | 17 (3.7%) |
| White | 426 (93.6%) |
| Job Category | |
| Office/Clerical/Professional | 71 (15.6%) |
| Maintenance/Mechanics | 81 (17.8%) |
| Laborers and Equipment Operators | 125 (27.5%) |
| Moving/Rubber Tire Equipment/Vehicle Operators | 82 (18.0%) |
| Supervisors | 51 (11.2%) |
| Miscellaneous/Others | 5 (1.1%) |
| Age | Neck | Low Back | Upper Back | Shoulders | Elbows | Hands | Hips | Knees | Feet |
|---|---|---|---|---|---|---|---|---|---|
| <25 (n = 40) | 13 (33%) | 21 (53%) | 8 (20%) | 14 (35%) | 6 (15%) | 9 (23%) | 10 (25%) | 17 (43%) | 12 (32%) |
| 25–34 (n = 81) | 30 (37%) | 49 (61%) | 19 (24%) | 27 (34%) | 16 (20%) | 14 (18%) | 13 (16%) | 36 (44%) | 30 (37%) |
| 35–44 (n = 96) | 39 (43%) | 63 (69%) | 28 (31%) | 40 (43%) | 19 (21%) | 35 (38%) | 19 (21%) | 39 (42%) | 28 (30%) |
| 45–54 (n = 97) | 33 (34%) | 46 (48%) | 20 (21%) | 36 (38%) | 9 (9%) | 16 (17%) | 19 (20%) | 33 (34%) | 25 (26%) |
| 55–64 (n = 113) | 51 (46%) | 67 (60%) | 30 (28%) | 41 (37%) | 17 (16%) | 29 (26%) | 28 (25%) | 36 (32%) | 28 (25%) |
| 65+ (n = 25) | 7 (28%) | 14 (56%) | 5 (22%) | 10 (42%) | 5 (20%) | 7 (28%) | 5 (20%) | 13 (52%) | 8 (32%) |
| Job Category | Neck | Low Back | Upper Back | Shoulders | Elbows | Hands | Hips | Knees | Feet |
|---|---|---|---|---|---|---|---|---|---|
| Office/Clerical Professional (n = 71) | 27 (39%) | 35 (49%) | 11 (16%) | 28 (41%) | 8 (11%) | 12 (17%) | 12 (17%) | 20 (28%) | 19 (27%) |
| Maintenance/Mechanics (n = 81) | 36 (46%) | 52 (66%) | 23 (30%) | 33 (42%) | 15 (19%) | 30 (39%) | 21 (27%) | 36 (46%) | 25 (32%) |
| Laborers and Equipment Operators (n = 125) | 42 (34%) | 70 (57%) | 34 (28%) | 41 (34%) | 16 (13%) | 36 (29%) | 27 (22%) | 52 (42%) | 37 (30%) |
| Moving/Rubber Tire Equipment Operators (n = 82) | 35 (43%) | 49 (61%) | 19 (24%) | 29 (35%) | 13 (16%) | 18 (23%) | 17 (21%) | 32 (40%) | 24 (30%) |
| Supervisors (n = 51) | 22 (43%) | 36 (71%) | 15 (31%) | 23 (45%) | 11 (22%) | 11 (22%) | 11 (22%) | 22 (43%) | 15 (29%) |
| Job Category | Low Back OR | Knee OR | Shoulder OR | Neck OR |
|---|---|---|---|---|
| Office/Clerical/Professional | Ref | Ref | Ref | Ref |
| Maintenance/Mechanics | 2.1 (1.1, 4.2) * | 2.2 (1.1, 4.6) * | 0.9 (0.5, 1.8) | 1.4 (0.7, 2.8) |
| Laborers and Equipment Operators | 1.6 (0.8, 2.9) | 2.0 (1.0, 3.9) * | 0.6 (0.3, 1.2) | 0.9 (0.5, 1.8) |
| Moving/Rubber Tire Equipment Operators | 1.7 (0.9, 3.4) | 1.7 (0.8, 3.5) | 0.7 (0.3, 1.3) | 1.3 (0.6, 2.5) |
| Supervisors | 2.8 (1.3, 6.2) * | 2.0 (0.9, 4.4) | 1 (0.5, 2.2) | 1.3 (0.6, 2.8) |
| Hours Worked Per Week | Low Back OR | Knees OR | Shoulder OR | Neck OR |
|---|---|---|---|---|
| Up to 40 (n = 64) | Ref | Ref | Ref | Ref |
| 41–50 (n = 213) | 1.7 (0.9, 3.0) | 1.4 (0.7, 2.5) | 1.3 (0.7, 2.5) | 1.7 (0.9, 3.3) |
| 51–60 (n = 128) | 1.4 (0.7, 2.5) | 1.1 (0.6, 2.2) | 1.3 (0.6, 2.4) | 2.7 (1.3, 5.3) ** |
| More than 60 (n = 47) | 4.7 (1.9, 11.5) ** | 4.5 (2.0, 10.3) ** | 1.6 (0.7, 3.6) | 5.1 (2.2, 11.8) ** |
| Age | Low Back OR | Knees OR | Shoulder OR | Neck OR |
|---|---|---|---|---|
| <25 (n = 40) | Ref | Ref | Ref | Ref |
| 25–34 (n = 81) | 1.4 (0.6, 3.0) | 1.1 (0.5, 2.3) | 1.0 (0.4, 2.3) | 1.1 (0.5, 2.6) |
| 35–44 (n = 96) | 1.8 (0.3, 3.8) | 1.0 (0.5, 2.2) | 1.6 (0.7, 3.5) | 1.5 (0.7, 3.3) |
| 45–54 (n = 97) | 0.8 (0.4, 1.7) | 0.7 (0.3, 1.5) | 1.3 (0.6, 2.7) | 1.1 (0.5, 2.3) |
| 55–64 (n = 113) | 1.3 (0.6, 2.6) | 0.6 (0.3, 1.3) | 1.2 (0.6, 2.6) | 1.6 (0.8, 3.5) |
| 65+ (n = 25) | 1.2 (0.4, 2.3) | 1.3 (0.5, 3.7) | 1.5 (0.5, 4.4) | 0.8 (0.3, 2.5) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balogun, A.O.; Smith, T.D. Musculoskeletal Symptoms among Stone, Sand and Gravel Mine Workers and Associations with Sociodemographic and Job-Related Factors. Int. J. Environ. Res. Public Health 2020, 17, 3512. https://doi.org/10.3390/ijerph17103512
Balogun AO, Smith TD. Musculoskeletal Symptoms among Stone, Sand and Gravel Mine Workers and Associations with Sociodemographic and Job-Related Factors. International Journal of Environmental Research and Public Health. 2020; 17(10):3512. https://doi.org/10.3390/ijerph17103512
Chicago/Turabian StyleBalogun, Abdulrazak O., and Todd D. Smith. 2020. "Musculoskeletal Symptoms among Stone, Sand and Gravel Mine Workers and Associations with Sociodemographic and Job-Related Factors" International Journal of Environmental Research and Public Health 17, no. 10: 3512. https://doi.org/10.3390/ijerph17103512
APA StyleBalogun, A. O., & Smith, T. D. (2020). Musculoskeletal Symptoms among Stone, Sand and Gravel Mine Workers and Associations with Sociodemographic and Job-Related Factors. International Journal of Environmental Research and Public Health, 17(10), 3512. https://doi.org/10.3390/ijerph17103512