Resilience in the Surgical Scheduling to Support Adaptive Scheduling System

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Context
2.3. Data Analysis
3. Results
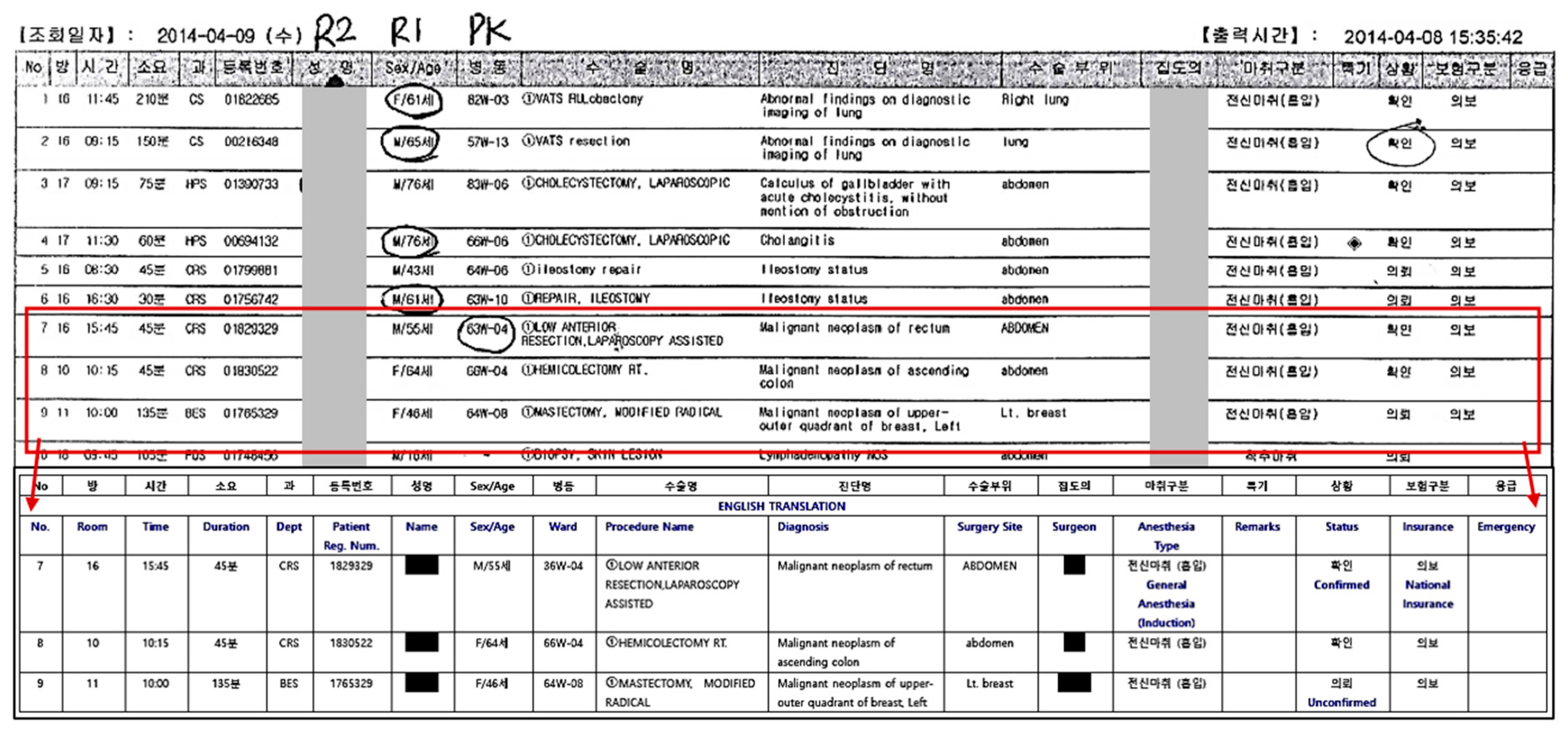
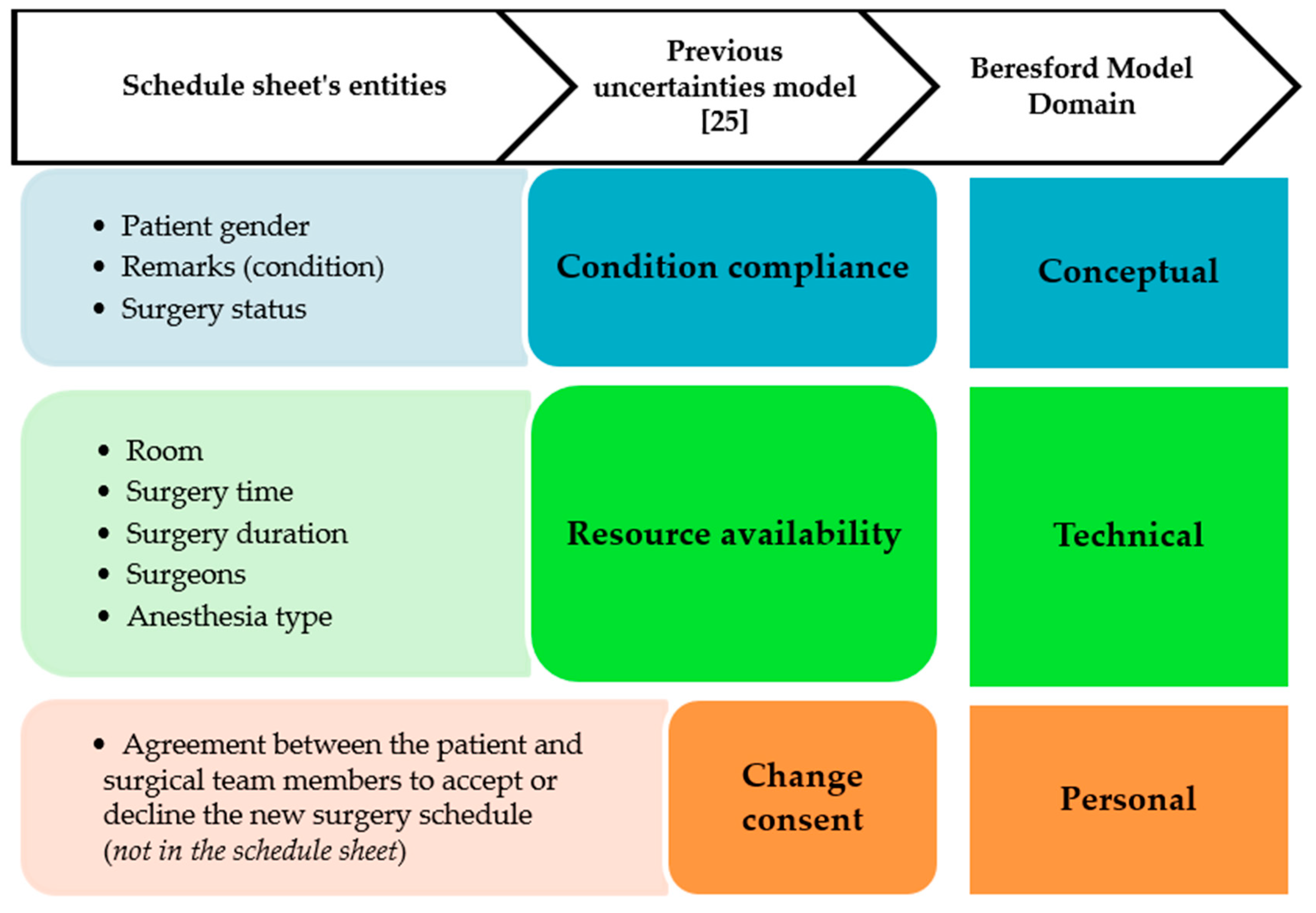
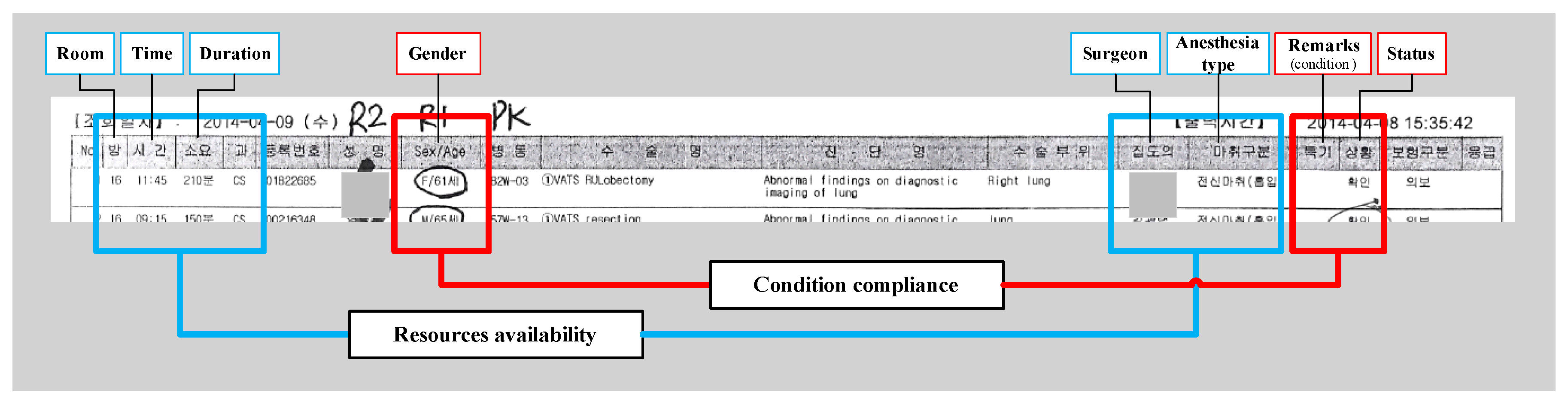
3.1. Dimension of Uncertainties Derived from the Schedule Sheet
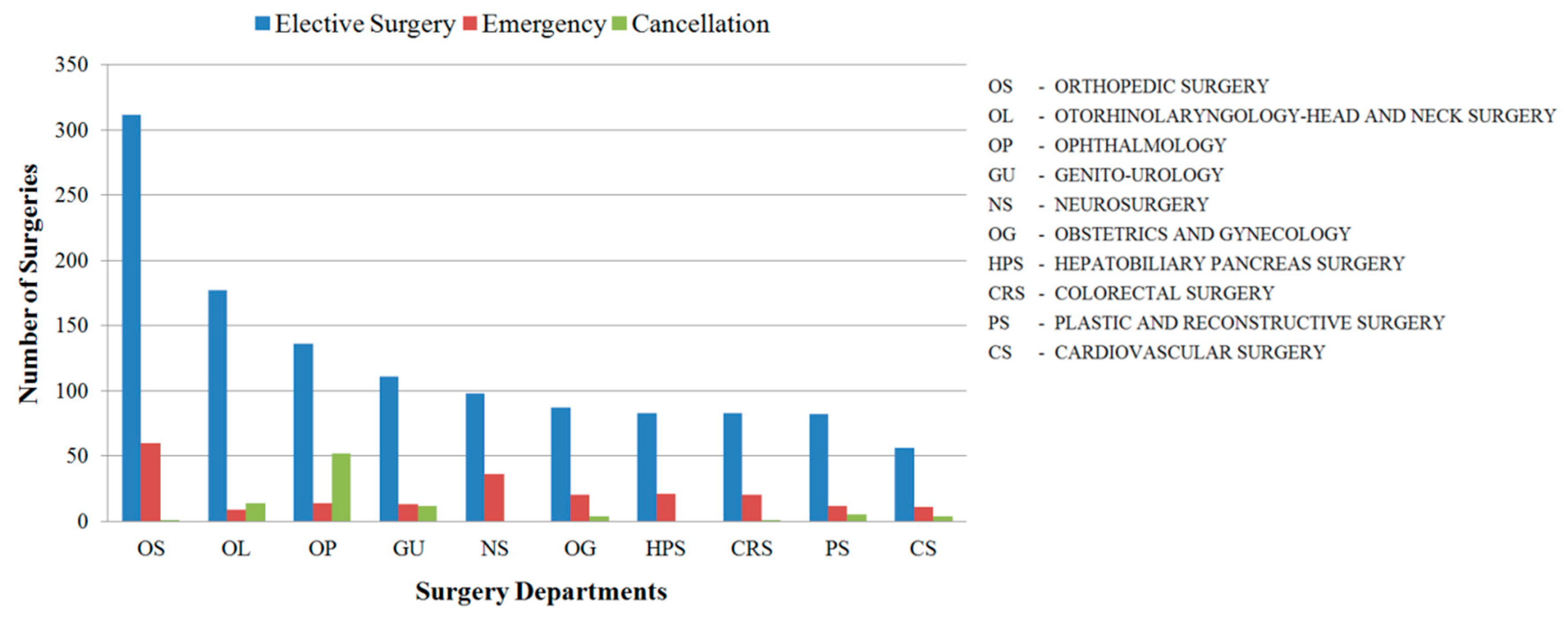
3.2. Prevalence of Surgeries
3.3. Pre- and Post-Surgical Scheduling Differences
3.4. Observation Results
3.4.1. Preparation
3.4.2. Indeterminate Schedule
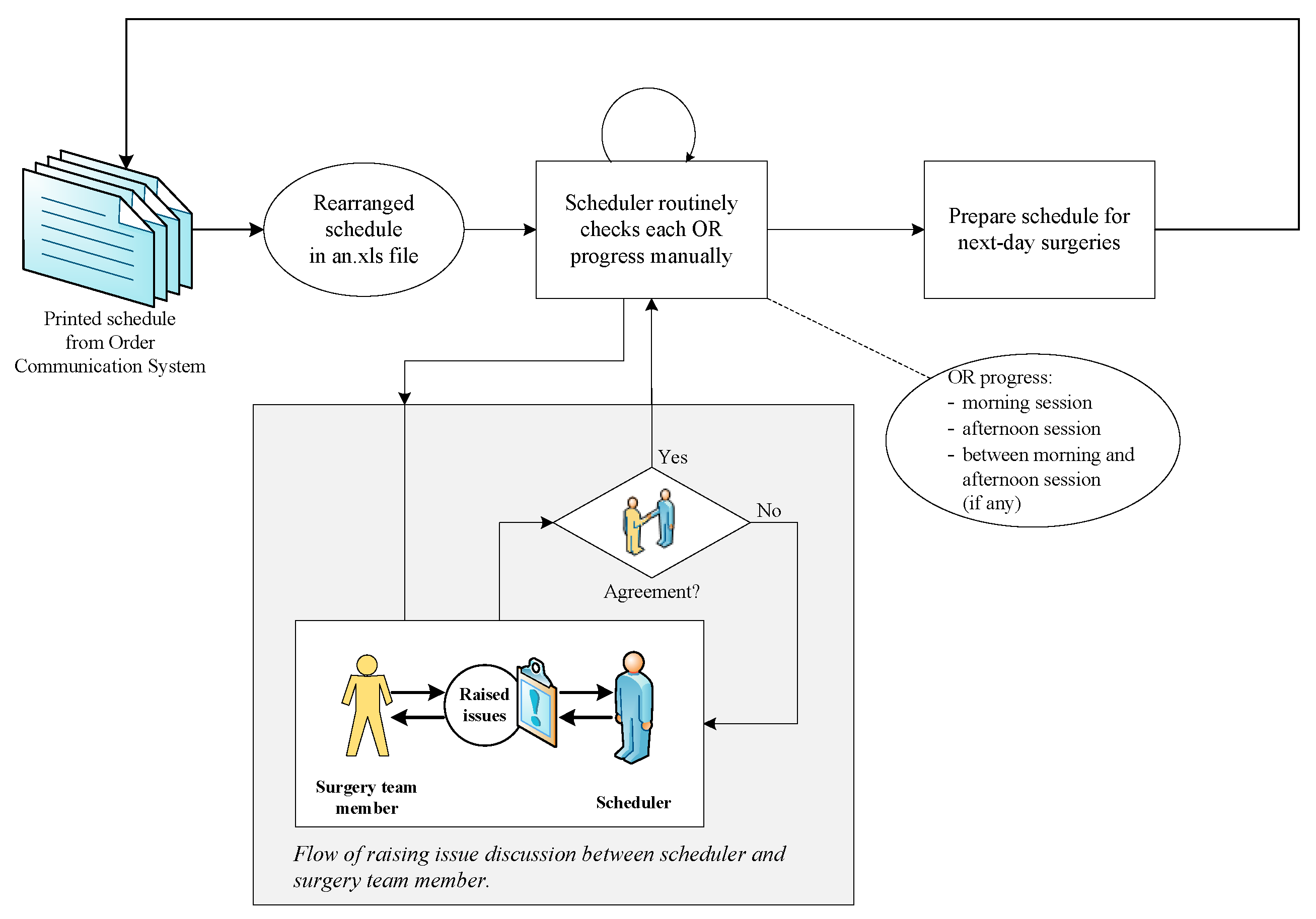
3.4.3. Communication
3.4.4. Schedule Updates
3.4.5. Scheduling Conflict
4. Discussion
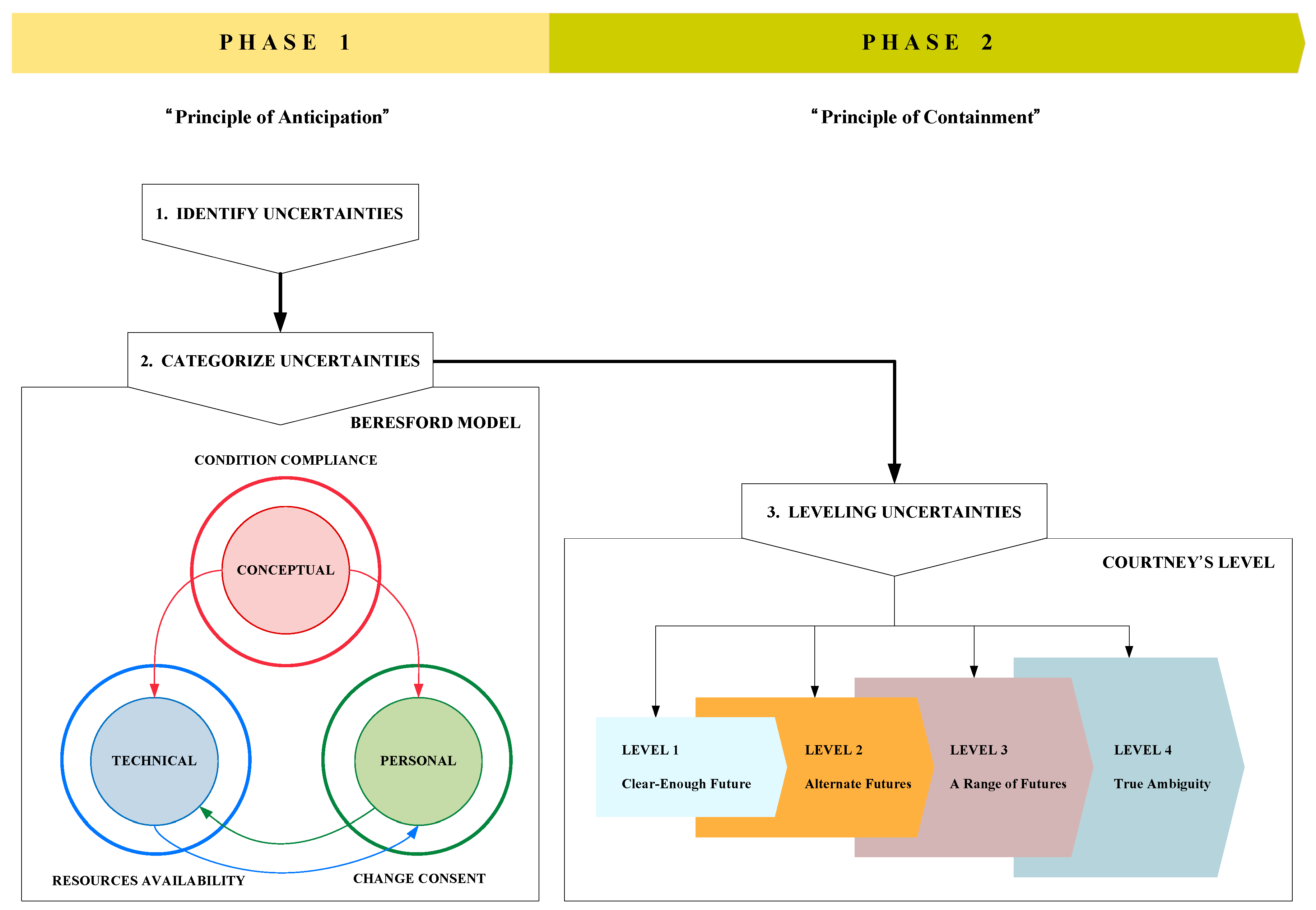
4.1. Categorization of Uncertainties
4.2. Resilience for Scheduling Change Management
4.3. Applications of the Proposed Framework
4.4. Toward an Adaptive Scheduling System
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| OR | Operating Room |
| HRO | High-Reliability Organization |
| OCS | Order Communication System |
| OS | Orthopedic Surgery |
| OL | Otorhinolaryngology-Head and Neck Surgery |
| GU | Genito-Urology |
| CRS | Colorectal Surgery |
| CS | Thoracic & Cardiovascular Surgery |
| SMS | Short Message Service |
| IM | Instant Messaging Service |
| ASA | American Society of Anesthesiologists |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Observation Category | Observed Results |
|---|---|
| Preparation | Scene 1: At approximately 8:15 AM, the OR manager began visiting each OR, confirmed its first surgery and instructed the attending surgeon to proceed on time at 8:30 AM. After all first surgeries had been confirmed, the OR manager returned to his appointed surgery by 8:30 AM and prepared anesthesia induction to his patient in OR 16. |
| Indeterminate schedule | Scene 2: At 2:20 PM, Surgeon S1 asked the OR manager whether it was possible to perform his scheduled surgery at 3:00 PM in OR 18. However, at this time, the OR manager could not confidently answer, because the current ongoing surgery started late and was still in progress; thus, he asked Surgeon S1 to wait and see if this surgery could finish by the scheduled time. |
| Communication | Scene 3: The OR manager received a phone call from Surgeon S1 at 3:00 PM asking whether he could use OR 18 for a transplantation vascular surgery. The OR manager then asked Surgeon S1 whether the surgery in progress was near conclusion and the patient of Surgeon S1 was ready for the surgery. Surgeon S1 replied that the current surgery was almost finished and his patient was ready for the surgery. The OR manager confirmed to Surgeon S1 that he could prepare the surgery in OR 18. Note that the OR manager and Surgeon S1 were in different rooms. |
| Scene 4: At 11:15 AM, Anesthesiologist P3 visited OR 16 and confirmed to the OR manager that the next surgery at 1:00 PM in OR 6 could proceed as scheduled. She explained the most up-to-date medical status of the patient and assured the OR manager that the patient was ready for the surgery. The OR manager updated the afternoon session and continued the room assignment for the afternoon session. | |
| Schedule updates | Scene 5: The OR manager checked the in-progress schedule for each room whenever he was not occupied by the surgery in OR 16. During a schedule inspection, the OR manager found that the current surgery was near completion; thus, he immediately contacted the attending surgeon for the next surgery and told them to prepare. |
| Scene 6: The OR manager received a phone call from Anesthesiologist P4 at 4:20 PM and was informed that the last surgery in OR 6 had been completed. The OR manager then asked Anesthesiologist P4 to close the OR and he updated the room assignment on his paper by marking an “X” on OR 6 the note that the room is closed for the day. | |
| Scheduling conflict | Scene 7: When the OR manager visited each OR before the morning session, Surgeon S2 approached him to extend the OR time. Surgeon S2 requested additional time, stated reasons for the request and argued that it was necessary. However, the OR manager declined his request because of the vast number of surgeries that day. He asked Surgeon S2 to manage their time and proceed with the surgery as according to the reserved schedule. |
| Scene 8: At 4:40 PM, the OR manager received a phone call from Anesthesiologist P5, who informed him that the remaining two surgeries could not be performed that day. Anesthesiologist P5 explained that the unstable condition of each of the patients proved unfavorable conditions for surgery but the surgeons continued to insist on performing the surgery. Consequently, the OR manager confirmed to Anesthesiologist P5 that the two surgeries in question would be postponed until the next day. This means that the OR manager canceled the surgeries despite the insistence of the attending surgeon. |
References
- Jang, J.; Lim, H.H.; Bae, G.; Choi, S.U.; Lim, C.H. Operation room management in Korea: Results of a survey. Korean J. Anesthesiol. 2016, 69, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-Z.; Lee, S.I.; Lee, H.W.; Lim, H.J.; Yoon, S.M.; Chang, S.H. The effect of increasing operating room capacity on day-of-surgery cancellation. Anaesth. Intensive Care 2009, 37, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Trentman, T.L.; Mueller, J.T.; Fassett, S.L.; Dormer, C.L.; Weinmeister, K.P. Day of surgery cancellations in a tertiary care hospital: A one year review. J. Anesth. Clin. Res. 2010, 1, 109. [Google Scholar] [CrossRef]
- Kumar, R.; Gandhi, R. Reasons for cancellation of operation on the day of intended surgery in a multidisciplinary 500 bedded hospital. J. Anaesthesiol. Clin. Pharmacol. 2012, 28, 66. [Google Scholar] [CrossRef]
- Dimitriadis, P.A.; Iyer, S.; Evgeniou, E. The challenge of cancellations on the day of surgery. Int. J. Surg. 2013, 11, 1126–1130. [Google Scholar] [CrossRef]
- Kaddoum, R.; Fadlallah, R.; Hitti, E.; EL-Jardali, F.; Eid, G.E. Causes of cancellations on the day of surgery at a Tertiary Teaching Hospital. BMC Health Serv. Res. 2016, 16, 259. [Google Scholar] [CrossRef]
- Kim, K.O.; Lee, J. Reasons for cancellation of elective surgery in a 500-bed teaching hospital: A prospective study. Korean J. Anesthesiol. 2014, 67, 66–67. [Google Scholar] [CrossRef]
- Fayed, A.; Elkouny, A.; Zoughaibi, N.; Wahabi, H.A. Elective surgery cancelation on day of surgery: An endless dilemma. Saudi J. Anaesth. 2016, 10, 68–73. [Google Scholar] [CrossRef]
- Cho, H.S.; Lee, Y.S.; Lee, S.G.; Kim, J.M.; Kim, T.H. Reasons for Surgery Cancellation in a General Hospital: A 10-year Study. Int. J. Environ. Res. Public Health 2019, 16, 7. [Google Scholar] [CrossRef]
- Cardoen, B.; Demeulemeester, E.; Beliën, J. Operating room planning and scheduling: A literature review. Eur. J. Oper. Res. 2010, 201, 921–932. [Google Scholar] [CrossRef]
- Batun, S.; Denton, B.T.; Huschka, T.R.; Schaefer, A.J. Operating room pooling and parallel surgery processing under uncertainty. INFORMS J. Comput. 2011, 23, 220–237. [Google Scholar] [CrossRef]
- Bruni, M.E.; Beraldi, P.; Conforti, D. A stochastic programming approach for operating theatre scheduling under uncertainty. IMA J. Manag. Math. 2015, 26, 99–119. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, T.; Luo, S.; Xu, D. Operating room scheduling and surgeon assignment problem under surgery durations uncertainty. Technol. Health Care 2018, 26, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Pang, B.; Xie, X.; Song, Y.; Luo, L. Surgery Scheduling Under Case Cancellation and Surgery Duration Uncertainty. IEEE T Autom. Sci. Eng. 2018, 16, 74–86. [Google Scholar] [CrossRef]
- Spratt, B.; Kozan, E.; Sinnott, M. Analysis of uncertainty in the surgical department: Durations, requests and cancellations. Aust. Health Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.A.O.; deSouza, M.C. Surgical scheduling under uncertainty by approximate dynamic programming. Omega 2019. [Google Scholar] [CrossRef]
- Perroca, M.G.; Jericó, M.D.C.; Facundin, S.D. Surgery cancelling at a teaching hospital: Implications for cost management. Rev. Latino-Am. Enferm. 2007, 15, 1018–1024. [Google Scholar] [CrossRef]
- Maimaiti, N.; Rahimi, A.; Aghaie, L.A. Economic impact of surgery cancellation in a general hospital, Iran. Ethiop. J. Health Dev. 2016, 30, 94–98. [Google Scholar]
- Hoehn, R.S.; Wima, K.; Vestal, M.A.; Weilage, D.J.; Hanseman, D.J.; Abbott, D.E.; Shah, S.A. Effect of Hospital Safety-Net Burden on Cost and Outcomes After Surgery. JAMA Surg. 2016, 151, 120–128. [Google Scholar] [CrossRef]
- Vali-Siar, M.M.; Gholami, S.; Ramezanian, R. Multi-period and multi-resource operating room scheduling under uncertainty: A case study. Comput. Ind. Eng. 2018, 126, 549–568. [Google Scholar] [CrossRef]
- Huang, W.T.; Chen, P.S.; Liu, J.J.; Chen, Y.R.; Chen, Y.H. Dynamic configuration scheduling problem for stochastic medical resources. J. Biomed. Inform. 2018, 80, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Pasupathy, K.S.; Sir, M.Y. Pattern-based strategic surgical capacity allocation. J. Biomed. Inform. 2019, 94, 103170. [Google Scholar] [CrossRef] [PubMed]
- Franke, S.; Meixensberger, J.; Neumuth, T. Intervention time prediction from surgical low-level tasks. J. Biomed. Inform. 2013, 46, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Wiyartanti, L.; Park, M.W.; Chung, D.; Kim, J.K.; Sohn, Y.T.; Kwon, G.H. Managing Uncertainties in the Surgical Scheduling. Stud. Health Technol. Inform. 2015, 210, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Meskens, N.; Duvivier, D.; Hanset, A. Multi-objective operating room scheduling considering desiderata of the surgical team. Decis. Support. Syst. 2013, 55, 650–659. [Google Scholar] [CrossRef]
- Fereday, E. Post-anaesthetic care unit bed escalation plan. ACORN J. Perioper. Nurs. Aust. 2015, 28, 20–21. [Google Scholar]
- Marques, I.; Captivo, M.E.; Barros, N. Optimizing the master surgery schedule in a private hospital. Oper. Res. Health Care 2019, 20, 11–24. [Google Scholar] [CrossRef]
- Affare, S.C.; Tolk, J.; Cantu, J. Analyzing Healthcare Tools Practitioners Use to Implement HRO Theory. In Proceedings of the 2015 Industrial and Systems Engineering Research Conference (ISERC), Nashville, TN, USA, 30 May–2 June 2015; pp. 493–498. [Google Scholar]
- Tsao, K.; Browne, M. Culture of safety: A foundation for patient care. In Seminars in pediatric surgery. Semin. Pediatr. Surg. 2015, 24, 283–287. [Google Scholar] [CrossRef]
- Høyland, S.A.; Skotnes, R.Ø.; Holte, K.A. An empirical exploration of the presence of HRO safety principles across the health care sector and construction industry in Norway. Saf. Sci. 2018, 107, 161–172. [Google Scholar] [CrossRef]
- Fairbanks, R.J.; Wears, R.L.; Woods, D.D.; Hollnagel, E.; Plsek, P.; Cook, R.I. Resilience and resilience engineering in health care. Jt. Comm. J. Qual. Saf. 2014, 40, 376–383. [Google Scholar] [CrossRef]
- Braithwaite, J.; Wears, R.L.; Hollnagel, E. Resilient health care: Turning patient safety on its head. Int. J. Qual. Health Care 2015, 27, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Ammar, W.; Kdouh, O.; Hammoud, R.; Hamadeh, R.; Harb, H.; Ammar, Z.; Atun, R.; Christiani, D.; Zalloua, P.A. Health system resilience: Lebanon and the Syrian refugee crisis. J. Glob. Health 2016, 6, 020704. [Google Scholar] [CrossRef] [PubMed]
- Borsci, S.; Uchegbu, I.; Buckle, P.; Ni, Z.; Walne, S.; Hanna, G.B. Designing medical technology for resilience: Integrating health economics and human factors approaches. Expert Rev. Med. Devices 2018, 15, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Beresford, E.B. Uncertainty and the shaping of medical decisions. Hastings Cent. Rep. 1991, 21, 6–11. [Google Scholar] [CrossRef]
- Courtney, H.; Kirkland, J.; Viguerie, P. Strategy under uncertainty. Harv. Bus. Rev. 1997, 75, 67–79. [Google Scholar] [PubMed]
- Wiyartanti, L.; Park, M.W.; Kwon, G.H. Personalized Activity Tracking System: Improving Situation Awareness for Anesthesiologist’s Task within the Surgical Team. In Proceedings of the 1st Asian Conference on Ergonomics and Design (ACED), Jeju, Korea, 21–24 May 2014; pp. 554–559. [Google Scholar]
- Wiyartanti, L.; Park, M.W.; Lim, C.H.; Kwon, G.H. Surgery Scheduling in the Perioperative Planning: A Preliminary Study of a Surgical Readiness in a General Hospital in South Korea. In Proceedings of the 13th International Conference on Control, Automation and Systems (ICCAS), Gwangju, Korea, 20–23 October 2013; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2013; pp. 807–811. [Google Scholar] [CrossRef]
- Farnan, J.M.; Johnson, J.K.; Meltzer, D.O.; Humphrey, H.J.; Arora, V.M. Resident uncertainty in clinical decision making and impact on patient care: A qualitative study. Qual. Saf. Health Care 2008, 17, 122–126. [Google Scholar] [CrossRef]
- Kazandjian, V.A.; Lipitz-Snyderman, A. HIT or miss: The application of health care information technology to managing uncertainty in clinical decision making. J. Eval. Clin. Pract. 2011, 17, 1108–1113. [Google Scholar] [CrossRef]
- Hamui-Sutton, A.; Vives-Varela, T.; Gutiérrez-Barreto, S.; Leenen, I.; Sánchez-Mendiola, M. A typology of uncertainty derived from an analysis of critical incidents in medical residents: A mixed methods study. BMC Med. Educ. 2015, 15, 198. [Google Scholar] [CrossRef]
- Pomare, C.; Churruca, K.; Ellis, L.A.; Long, J.C.; Braithwaite, J. A revised model of uncertainty in complex healthcare settings: A scoping review. J. Eval. Clin. Pract. 2019, 25, 176–182. [Google Scholar] [CrossRef]
- Braaf, S.; Riley, R.; Manias, E. Failures in communication through documents and documentation across the perioperative pathway. J. Clin. Nurs. 2015, 24, 1874–1884. [Google Scholar] [CrossRef]
- Dios, M.; Molina-Pariente, J.M.; Fernandez-Viagas, V.; Andrade-Pineda, J.L.; Framinan, J.M. A decision support system for operating room scheduling. Comput. Ind. Eng. 2015, 88, 430–443. [Google Scholar] [CrossRef]
- Wahlström, M.; Seppänen, L.; Norros, L.; Aaltonen, I.; Riikonen, J. Resilience through interpretive practice–A study of robotic surgery. Saf. Sci. 2018, 108, 113–128. [Google Scholar] [CrossRef]
- Weick, K.E.; Sutcliffe, K.M. Managing the Unexpected: Resilient Performance in an Age of Uncertainty, 2nd ed.; Jossey-Bass: San Fransisco, CA, USA, 2007; pp. 71–73. [Google Scholar]
- Courtney, H. Decision-driven scenarios for assessing four levels of uncertainty. Strategy Leadersh. 2003, 31, 14–22. [Google Scholar] [CrossRef]
- Gaubinger, K.; Rabl, M.; Swan, S.; Werani, T. (Eds.) Corporate Success Through Market Driven Innovation. In Innovation and Product Management; Springer Texts in Business and Economics; Springer: Berlin, Germany, 2015; pp. 3–25. [Google Scholar] [CrossRef]
- Garcia, E.F.; Zúñiga, E.R.; Bruch, J.; Moris, M.U.; Syberfeldt, A. Simulation-based Optimization for Facility Layout Design in Conditions of High Uncertainty. Procedia CIRP 2018, 72, 334–339. [Google Scholar] [CrossRef]
- ASA Physical Status Classification System | American Society of Anesthesiologists (ASA). Available online: http://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system (accessed on 25 March 2020).
- Bogdanovic, J.; Perry, J.; Guggenheim, M.; Manser, T. Adaptive coordination in surgical teams: An interview study. BMC Health Serv. Res. 2015, 15, 128. [Google Scholar] [CrossRef]
- Conn, L.G.; Haas, B.; Cuthbertson, B.H.; Amaral, A.C.; Coburn, N.; Nathens, A.B. Communication and culture in the surgical intensive care unit: Boundary production and the improvement of patient care. Qual. Health Res. 2016, 26, 895–906. [Google Scholar] [CrossRef]
- Yanes, A.F.; McElroy, L.M.; Abecassis, Z.A.; Holl, J.; Woods, D.; Ladner, D.P. Observation for assessment of clinician performance: A narrative review. BMJ Qual. Saf. 2016, 25, 46–55. [Google Scholar] [CrossRef]
- Cumin, D.; Skilton, C.; Weller, J. Information transfer in multidisciplinary operating room teams: A simulation-based observational study. BMJ Qual. Saf. 2017, 26, 209–216. [Google Scholar] [CrossRef]
- Rankin, A.; Lundberg, J.; Woltjer, R.; Rollenhagen, C.; Hollnagel, E. Resilience in Everyday Operations: A Framework for Analyzing Adaptations in High-Risk Work. J. Cogn. Eng. Decis. Mak. 2014, 8, 78–97. [Google Scholar] [CrossRef]
- Anderson, J.E.; Ross, A.J.; Jaye, P. Modelling Resilience and Researching the Gap between Work-as-Imagined and Work-as-done. In Resilient Health Care: Reconciling Work-as-Imagined and Work-as-Done, 1st ed.; Braithwaite, J., Wears, R.L., Hollnagel, E., Eds.; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2017; Volume 3, pp. 133–141. [Google Scholar]
- Cooke, F.L.; Cooper, B.; Bartram, T.; Wang, J.; Mei, H. Mapping the relationships between high-performance work systems, employee resilience and engagement: A study of the banking industry in China. Int. J. Hum. Resour. Man. 2019, 30, 1239–1260. [Google Scholar] [CrossRef]
- Molino, M.; Cortese, C.G.; Ghislieri, C. The Promotion of Technology Acceptance and Work Engagement in Industry 4.0: From Personal Resources to Information and Training. Int. J. Environ. Res. Public Health 2020, 17, 2438. [Google Scholar] [CrossRef] [PubMed]
- Lalys, F.; Jannin, P. Surgical process modelling: A review. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 495–511. [Google Scholar] [CrossRef] [PubMed]
- Dergachyova, O.; Bouget, D.; Huaulmé, A.; Morandi, X.; Jannin, P. Automatic data-driven real-time segmentation and recognition of surgical workflow. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Franke, S.; Neumuth, T. Rule-Based Medical Device Adaptation for the Digital Operating Room. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2015; pp. 1733–1736. [Google Scholar] [CrossRef]
- Wright, M.C.; Endsley, M.R. Building Shared Situation Awareness in Healthcare Settings. In Improving Healthcare Team Communication; Nemeth, C.P., Ed.; CRC Press: London, UK, 2017; pp. 97–114. [Google Scholar] [CrossRef]
- van Essen, J.T.; Hurink, J.L.; Hartholt, W.; van den Akker, B.J. Decision support system for the operating room rescheduling problem. Health Care Manag. Sci. 2012, 15, 355–372. [Google Scholar] [CrossRef]
- Spangenberg, N.; Wilke, M.; Augenstein, C.; Franczyk, B. Online Surgery Rescheduling-A Data-driven Approach for Real-time Decision Support. In Proceedings of the 20th International Conference on Enterprise Information Systems (ICEIS 2018), Funchal, Portugal, 21–24 March 2018; pp. 336–343. [Google Scholar] [CrossRef]
- Hasvold, P.E.; Scholl, J. Flexibility in interaction: Sociotechnical design of an operating room scheduler. Int. J. Med. Inform. 2011, 80, 631–645. [Google Scholar] [CrossRef]
- Bonzo, S.M.; McLain, D.; Avnet, M.S. Process Modeling in the Operating Room: A Socio-Technical Systems Perspective. Syst. Eng. 2016, 19, 267–277. [Google Scholar] [CrossRef]
- Martinez-Millana, A.; Lizondo, A.; Gatta, R.; Vera, S.; Salcedo, V.T.; Fernandez-Llatas, C. Process mining dashboard in operating rooms: Analysis of staff expectations with analytic hierarchy process. Int. J. Environ. Res. Public Health 2019, 16, 199. [Google Scholar] [CrossRef]
- Chen, A.T.; Wu, S.; Tomasino, K.N.; Lattie, E.G.; Mohr, D.C. A multi-faceted approach to characterizing user behavior and experience in a digital mental health intervention. J. Biomed. Inform. 2019, 94, 103187. [Google Scholar] [CrossRef]







| Measurement | Pre-Surgical | Post-Surgical |
|---|---|---|
| Data Collection | ||
| Data collection start date | 26 October 2015 | 26 October 2015 |
| Data collection end date | 4 December 2015 | 4 December 2015 |
| Number of days | 20 days | 20 days |
| Number of surgeries | 1016 | 1391 |
| Average surgeries per day | 50.80 | 69.55 |
| Standard Deviation | 7.46 | 13.14 |
| Time of Surgeries | ||
| Morning Session (08:30–12:00) | 613 | 808 |
| Mid-Daytime Session (12:00–13:00) | 157 | 222 |
| Afternoon Session (13:00–16:30) | 246 | 361 |
| Overtime Surgeries | ||
| Surgeries during office hours * | 933 | 1305 |
| Surgeries possibly out of office hours | 83 | 86 |
| Surgeries not during office hours | 32 | 45 |
| Surgery Changes | ||
| Surgery schedule changes | 141 | |
| Operating room changes | 326 | |
| Additional cases (average **/std. deviation) | 437 (21.85/8.07) | |
| Emergency cases (average **/std. deviation) | 10 | 268 (13.40/4.21) |
| Cancellation (average **/std. deviation) | 63 (3.15/1.93) | |
| Surgery Duration | ||
| Maximum surgery duration (minutes) | 750 | 750 |
| Minimum surgery duration (minutes) | 12 | 12 |
| Average/std. deviation (minutes) | 79.44 (67.95) | 80.78 (69.38) |
| Surgery Department | Operating Room |
|---|---|
| Otorhinolaryngology-Head and Neck Surgery | OR 1(R *), OR 9 |
| Neurosurgery | OR 2, OR 3 |
| Orthopedic Surgery | OR 4, OR 19, OR 20 |
| Plastic and Reconstructive Surgery | OR 5, OR 13 |
| Thoracic & Cardiovascular Surgery | OR 7, OR 16 |
| Genito-Urology | OR 8 |
| Transplantation Vascular Surgery/Colorectal Surgery | OR 10 |
| Breast and Endocrine Surgery | OR 11 |
| Ophthalmology | OR 14 |
| Obstetrics and Gynecology | OR 15 |
| Hepatobiliary Pancreas Surgery | OR 17 |
| Transplantation Vascular Surgery | OR 18 |
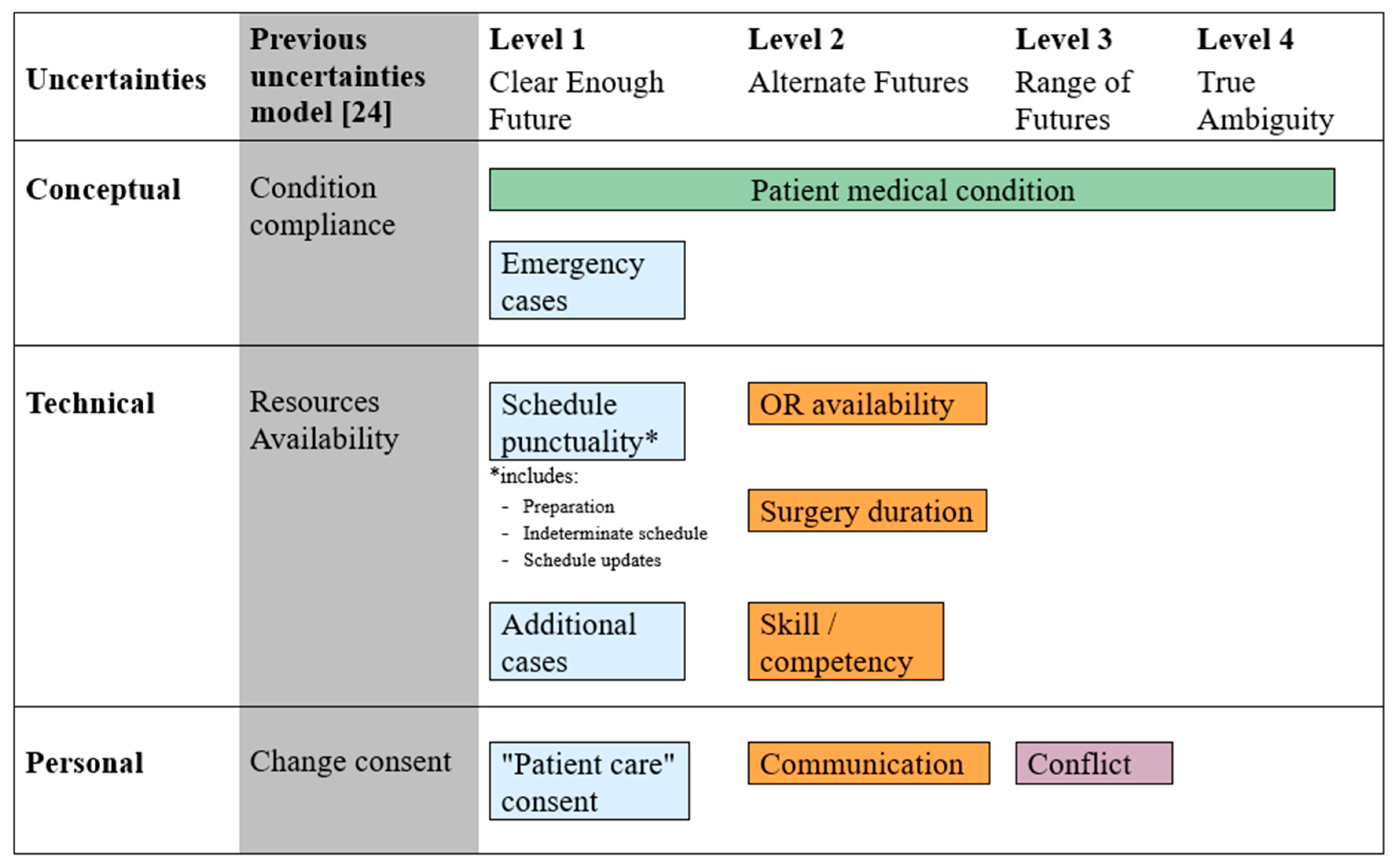
| Beresford Model Domain | Previous Uncertainties Model [24] | Observed Factors | Evidence (Scenes are from Table A1) | |
|---|---|---|---|---|
| (From Schedule Sheets) | (From Observation) | |||
| Conceptual uncertainty | Condition compliance | Patient medical condition1 | Scene 3, Scene 8 | |
| Emergency cases | Table 1 | |||
| Technical uncertainty | Resource availability | Schedule punctuality | Preparation, Indeterminate schedule | Scene 1, Scene 2, Scene 6, Scene 7 |
| OR availability | Communication, schedule updates | Scene 2, Scene 3, Scene 5 | ||
| Surgery duration, skill/competency1 | Scene 2, Scene 7 | |||
| Additional cases | Table 1 | |||
| Personal uncertainty | Change consent | “Patient care” consent1 | Scene 8 | |
| Communication | Scene 3, Scene 4 | |||
| Scheduling conflict | Scene 7, Scene 8 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiyartanti, L.; Lim, C.H.; Park, M.W.; Kim, J.K.; Kwon, G.H.; Kim, L. Resilience in the Surgical Scheduling to Support Adaptive Scheduling System. Int. J. Environ. Res. Public Health 2020, 17, 3511. https://doi.org/10.3390/ijerph17103511
Wiyartanti L, Lim CH, Park MW, Kim JK, Kwon GH, Kim L. Resilience in the Surgical Scheduling to Support Adaptive Scheduling System. International Journal of Environmental Research and Public Health. 2020; 17(10):3511. https://doi.org/10.3390/ijerph17103511
Chicago/Turabian StyleWiyartanti, Lisa, Choon Hak Lim, Myon Woong Park, Jae Kwan Kim, Gyu Hyun Kwon, and Laehyun Kim. 2020. "Resilience in the Surgical Scheduling to Support Adaptive Scheduling System" International Journal of Environmental Research and Public Health 17, no. 10: 3511. https://doi.org/10.3390/ijerph17103511
APA StyleWiyartanti, L., Lim, C. H., Park, M. W., Kim, J. K., Kwon, G. H., & Kim, L. (2020). Resilience in the Surgical Scheduling to Support Adaptive Scheduling System. International Journal of Environmental Research and Public Health, 17(10), 3511. https://doi.org/10.3390/ijerph17103511