Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- US Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. Available online: http://health.gov/dietaryguidelines/2015 (accessed on 20 October 2017).
- US Department of Agriculture Food; Nutrition Service. Healthy Eating Index (HEI). Available online: https://www.fns.usda.gov/resource/healthy-eating-index-hei (accessed on 8 August 2019).
- World Health Organization; United Nations Food; Agriculture Organization. Diet, Nutrition and the Prevention of Chronic Diseases; Technical Report Series No. 916; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- US Public Halth Service Office of the Sugreon General. The Surgeon General’s Report on Nutriton and Health; U.S. Department of Health and Human Services, Public Health Service: Washington, DC, USA, 1988.
- Micha, R.; Peñalvo, J.L.; Cudhea, F.; Imamura, F.; Rehm, C.D.; Mozaffarian, D. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. J. Am. Med. Assoc. 2017, 317, 912–924. [Google Scholar] [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Beaulac, J.; Kristjansson, E.; Cummins, S. A systematic review of food deserts, 1996–2007. Prev. Chronic Dis. 2009, 6, A105. Available online: http://www.cdc.gov/pcd/issues/2009/jul/08_0163.htm. (accessed on 1 May 2020).
- US Department of Agriculture Economic Research Service. Food Access Research Atlas. Available online: https://www.ers.usda.gov/data-products/food-access-research-atlas/ (accessed on 5 August 2019).
- Rose, D.; Bodor, J.N.; Swalm, C.M.; Rice, J.C.; Farley, T.A.; Hutchinson, P.L. Deserts in New Orleans? Illustrations of Urban Food Access and Implications for Policy. Available online: https://pdfs.semanticscholar.org/abc8/b418aa0783c8f3b0a0c4fca8f137ad806e0a.pdf (accessed on 6 April 2020).
- Block, J.P.; Scribner, R.A.; Desalvo, K.B. Fast food, race/ethnicity, and income: A geographic analysis. Am. J. Prev. Med. 2004, 27, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Hager, E.R.; Cockerham, A.; O’Reilly, N.; Harrington, D.; Harding, J.; Hurley, K.M.; Black, M.M. Food swamps and food deserts in Baltimore City, MD, USA: Associations with dietary behaviours among urban adolescent girls. Public Health Nutr. 2017, 20, 2598–2607. [Google Scholar] [CrossRef] [PubMed]
- Thomson, J.L.; Tussing-Humphreys, L.M.; Goodman, M.H. Delta Healthy Sprouts: A randomized comparative effectiveness trial to promote maternal weight control and reduce childhood obesity in the Mississippi Delta. Contemp. Clin. Trials 2014, 38. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief 2017, 219, 1–8. [Google Scholar]
- Robert Wood Johnson Foundation. County Health Rankings & Roadmaps. Available online: https://www.countyhealthrankings.org/ (accessed on 5 August 2019).
- Trust for America’s Health; Robert Wood Johnson Foundation. The State of Childhood Obesity. Available online: https://stateofobesity.org/childhood (accessed on 9 January 2018).
- Tussing-Humphreys, L.M.; Thomson, J.L.; Goodman, M.H.; Olender, S. Maternal diet quality and nutrient intake in the gestational period: Results from the Delta Healthy Sprouts comparative impact trial. Matern. Health Neonatol. Perinatol. 2016, 2, 8. [Google Scholar] [CrossRef][Green Version]
- Thomson, J.L.; Tussing-Humphreys, L.M.; Landry, A.S.; Goodman, M.H. No improvements in postnatal dietary outcomes were observed in a two-arm, randomized, controlled, comparative impact trial among rural, Southern, African-American women. J. Acad. Nutr. Diet. 2018, 118, 1196–1207. [Google Scholar] [CrossRef]
- Thomson, J.L.; Goodman, M.H.; Landry, A.S. Measurement of nutrition environments in grocery stores, convenience stores, and restaurants in the Lower Mississippi Delta. Prev. Chronic Dis. 2020, 17, 190293. [Google Scholar] [CrossRef]
- US Department of Agriculture Economic Research Service. Food Environment Atlas. Available online: https://www.ers.usda.gov/data-products/food-environment-atlas/ (accessed on 8 August 2019).
- US Department of Agriculture Food and Nutrition Service. Where can I Use SNAP EBT? Available online: https://www.fns.usda.gov/snap/retailerlocator (accessed on 15 March 2016).
- Mississippi State Department of Health. Restaurant and Food Facility Inspections. Available online: https://msdh.ms.gov/msdhsite/_static/43,1911,231,203.html (accessed on 15 March 2016).
- B2bBiz.com. B2BYellowpages.com. Available online: https://www.b2byellowpages.com/ (accessed on 15 March 2016).
- National Space and Aeronautics Administration. Latitude/Longitude Finder. Available online: https://mynasadata.larc.nasa.gov/latitudelongitude-finder/ (accessed on 15 March 2016).
- University of Minnesota Nutrition Coordinating Center. Nutrition Data System for Research (NDSR). Available online: http://www.ncc.umn.edu/products/ (accessed on 9 April 2019).
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.B.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture; U.S. Department of Health and Human Services. 2010–2015 Dietary Guidelines for Americans. Available online: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2010 (accessed on 8 May 2019).
- Charreire, H.; Casey, R.; Salze, P.; Simon, C.; Chaix, B.; Banos, A.; Badariotti, D.; Weber, C.; Oppert, J.M. Measuring the food environment using geographical information systems: A methodological review. Public Health Nutr. 2010, 13, 1773–1785. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A. The ESRI Guide to GIS Analysis -Volume 2: Spatial Measurements and Statistics; ESRI Press: Redlands, CA, USA, 2009. [Google Scholar]
- ESRI. How Hot Spot Analysis (Getis-Ord Gi*) Works. Available online: https://pro.arcgis.com/en/pro-app/tool-reference/spatial-statistics/h-how-hot-spot-analysis-getis-ord-gi-spatial-stati.htm (accessed on 8 May 2019).
- Mississippi Department of Transportation. 2019 Official State Highway Map Mississippi. Available online: https://mdot.ms.gov/portal/maps (accessed on 5 August 2019).
- US Census Bureau. American Community Survey. Available online: https://www.census.gov/acs/www/data/data-tables-and-tools/data-profiles/2016/ (accessed on 5 August 2019).
- US Census Bureau Geography Program. Urban and Rural. Available online: https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural.html (accessed on 5 August 2019).
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments. Disparities in access to healthy foods in the U.S. Am. J. Prev. Med. 2009, 36. [Google Scholar] [CrossRef]
- Rahkovsky, I.; Snyder, S. Food Choices and Store Proximity; Economic Research Service Report Number 195; Economic Research Service: Washington, DC, USA, 2015.
- Ver Ploeg, M.; Rahkovsky, I. Recent Evidence on the Effects of Food Store Access on Food Choice and Diet Quality. Available online: https://www.ers.usda.gov/amber-waves/2016/may/recent-evidence-on-the-effects-of-food-store-access-on-food-choice-and-diet-quality/ (accessed on 1 May 2020).
- Lo, B.K.; Megiel, S.; Liu, E.; Folta, S.C.; Graham, M.L.; Seguin, R.A. Associations between frequency of food shopping at different food sources and fruit and vegetable intake among rural residents in upstate New York, USA. Public Health Nutr. 2019, 22, 2472–2478. [Google Scholar] [CrossRef]
- Ver Ploeg, M.; Mancino, L.; Todd, J.E.; Clay, D.M.; Scharadin, B. Where Do Americans Usually Shop for Food and How Do They Travel to Get There? Initial Findings from the National Household Food Acquisition and Purchase Survey; Ecomomic Information Bulletin No. 138; Economic Research Service: Washington, DC, USA, 2015.
- Stern, D.; Poti, J.M.; Ng, S.W.; Robinson, W.R.; Gordon-Larsen, P.; Popkin, B.M. Where people shop is not associated with the nutrient quality of packaged foods for any racial-ethnic group in the United States. Am. J. Clin. Nutr. 2016, 103, 1125–1134. [Google Scholar] [CrossRef]
- Vaughan, C.A.; Cohen, D.A.; Ghosh-Dastidar, M.; Hunter, G.P.; Dubowitz, T. Where do food desert residents buy most of their junk food? Supermarkets. Public Health Nutr. 2017, 20, 2608–2616. [Google Scholar] [CrossRef]
- Richardson, A.S.; Ghosh-Dastidar, M.; Beckman, R.; Flórez, K.R.; DeSantis, A.; Collins, R.L.; Dubowitz, T. Can the introduction of a full-service supermarket in a food desert improve residents’ economic status and health? Ann. Epidemiol. 2017, 27, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Allcott, H.; Diamond, R.; Dubé, J.-P.; Handbury, J.; Rahkovsky, I.; Schnell, M. Food deserts and the causes of nutritional inequality. Q. J. Econ. 2019, 134, 1793–1844. [Google Scholar] [CrossRef]
- Rhone, A.; Ver Ploeg, M.; Williiams, R.; Breneman, V. Understanding Low-Income and Low-Access Census Tracts Across the Nation: Subnational and Subpopulation Estimates of Access to Healthy Food; Economic Information Bulletin No. 2019; Economic Research Service: Washington, DC, USA, 2019.
- Moore, L.V.; Roux, A.V.D.; Nettleton, J.A.; Jacobs, D.R.; Franco, M. Fast-food consumption, diet quality, and neighborhood exposure to fast food: The Multi-Ethnic Study of Atherosclerosis. Am. J. Epidemiol. 2009, 170, 29–36. [Google Scholar] [CrossRef]
- Vaughan, C.A.; Collins, R.; Ghosh-Dastidar, M.; Beckman, R.; Dubowitz, T. Does where you shop or who you are predict what you eat? The role of stores and individual characteristics in dietary intake. Prev. Med. (Baltim.) 2017, 100, 10–16. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic 1 | United States | Town 1 | Town 2 | Town 3 | Town 4 | Town 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Population (n) | 32,612 | 12,346 | 4254 | 2484 | 1750 | |||||||
| Black (%) | 13.8 | 80.0 | 49.4 | 68.9 | 86.0 | 90.7 | ||||||
| Below poverty level (%) | 15.1 | 36.0 | 28.5 | 32.1 | 41.4 | 50.6 | ||||||
| Overall | Town 1 | Town 2 | Town 3 | Town 4 | Town 5 | |||||||
| Food outlet class | n | % | n | % | n | % | n | % | n | % | n | % |
| Grocery store | 11 | 4.1 | 5 | 45.5 | 4 | 36.4 | 1 | 9.1 | 1 | 9.1 | 0 | 0.0 |
| Convenience store | 86 | 32.3 | 48 | 55.8 | 18 | 20.9 | 10 | 11.6 | 6 | 7.0 | 4 | 4.7 |
| Full-service restaurant | 50 | 18.8 | 28 | 56.0 | 16 | 32.0 | 5 | 10.0 | 1 | 2.0 | 0 | 0.0 |
| Fast food restaurant | 119 | 44.7 | 60 | 50.4 | 40 | 33.6 | 8 | 6.7 | 7 | 5.9 | 4 | 3.4 |
| Convenience store subclass | ||||||||||||
| Corner store | 21 | 24.4 | ||||||||||
| Gas station | 40 | 46.5 | ||||||||||
| Chain dollar store | 21 | 24.4 | ||||||||||
| Chain pharmacy | 4 | 4.7 | ||||||||||
| Fast food restaurant subclass | ||||||||||||
| Corner store | 5 | 4.2 | ||||||||||
| Gas station | 25 | 21.0 | ||||||||||
| Grocery store delicatessen | 8 | 6.7 | ||||||||||
| Restaurant stand-alone | 81 | 68.1 | ||||||||||
| Distance between Residence and Food Outlet | ||||||
|---|---|---|---|---|---|---|
| Miles | % Living Within | |||||
| Food Outlet Class | Range | Mean | SD | 1/4 Mile | 1/2 Mile | 1 Mile |
| Grocery store | ||||||
| Closest | 0.4–11.1 | 1.6 | 2.13 | 0.0 | 5.9 | 44.1 |
| Most food purchased 1 | 0.4–22.9 | 4.2 | 5.15 | 0.0 | 1.6 | 14.5 |
| Convenience store | <0.1–1.1 | 0.4 | 0.23 | 29.4 | 76.5 | 98.5 |
| Full-service restaurant | 0.1–10.0 | 1.1 | 1.97 | 11.8 | 30.9 | 79.4 |
| Fast food restaurant | 0.1–1.5 | 0.5 | 0.25 | 19.1 | 66.2 | 95.6 |
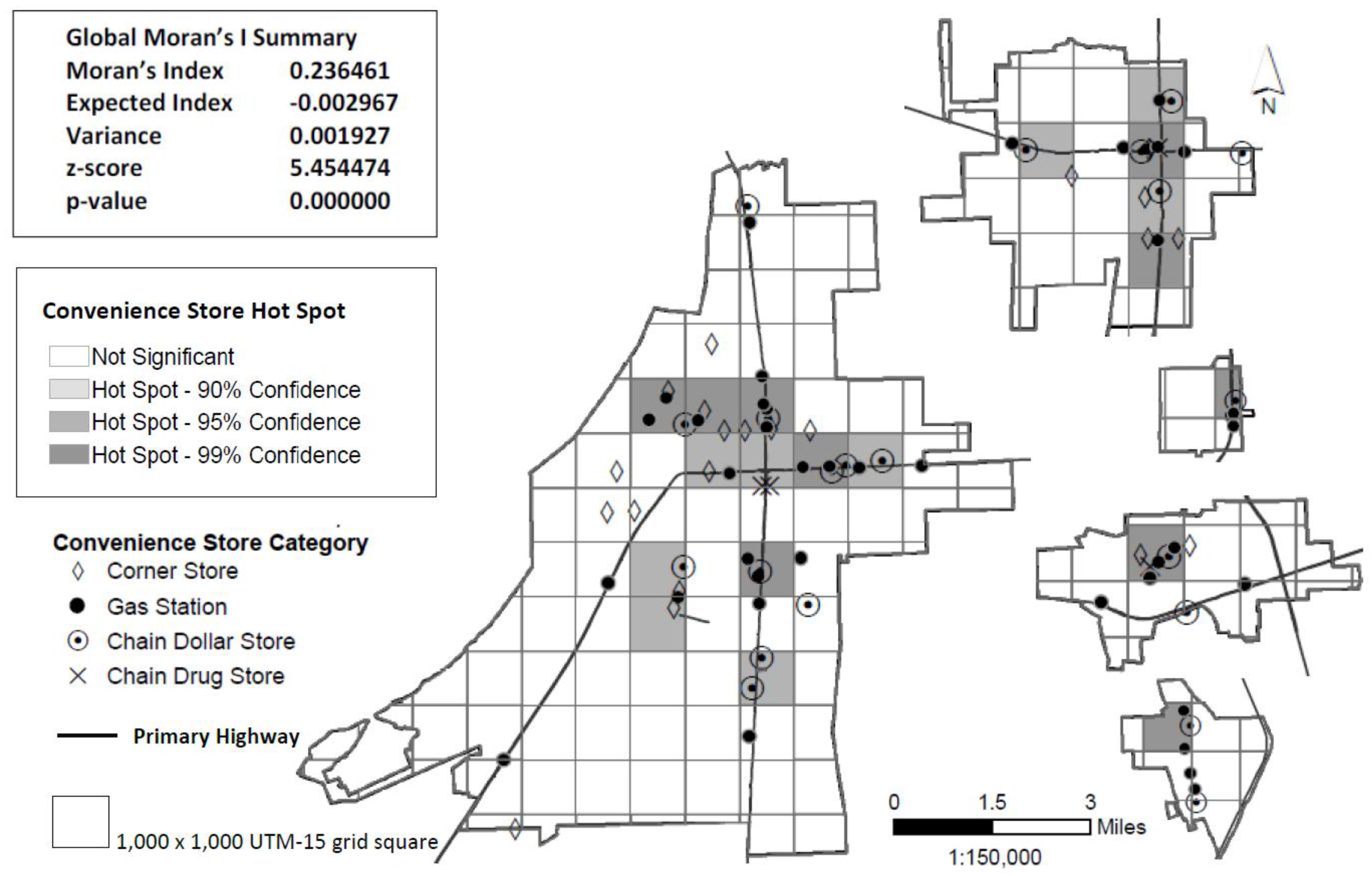
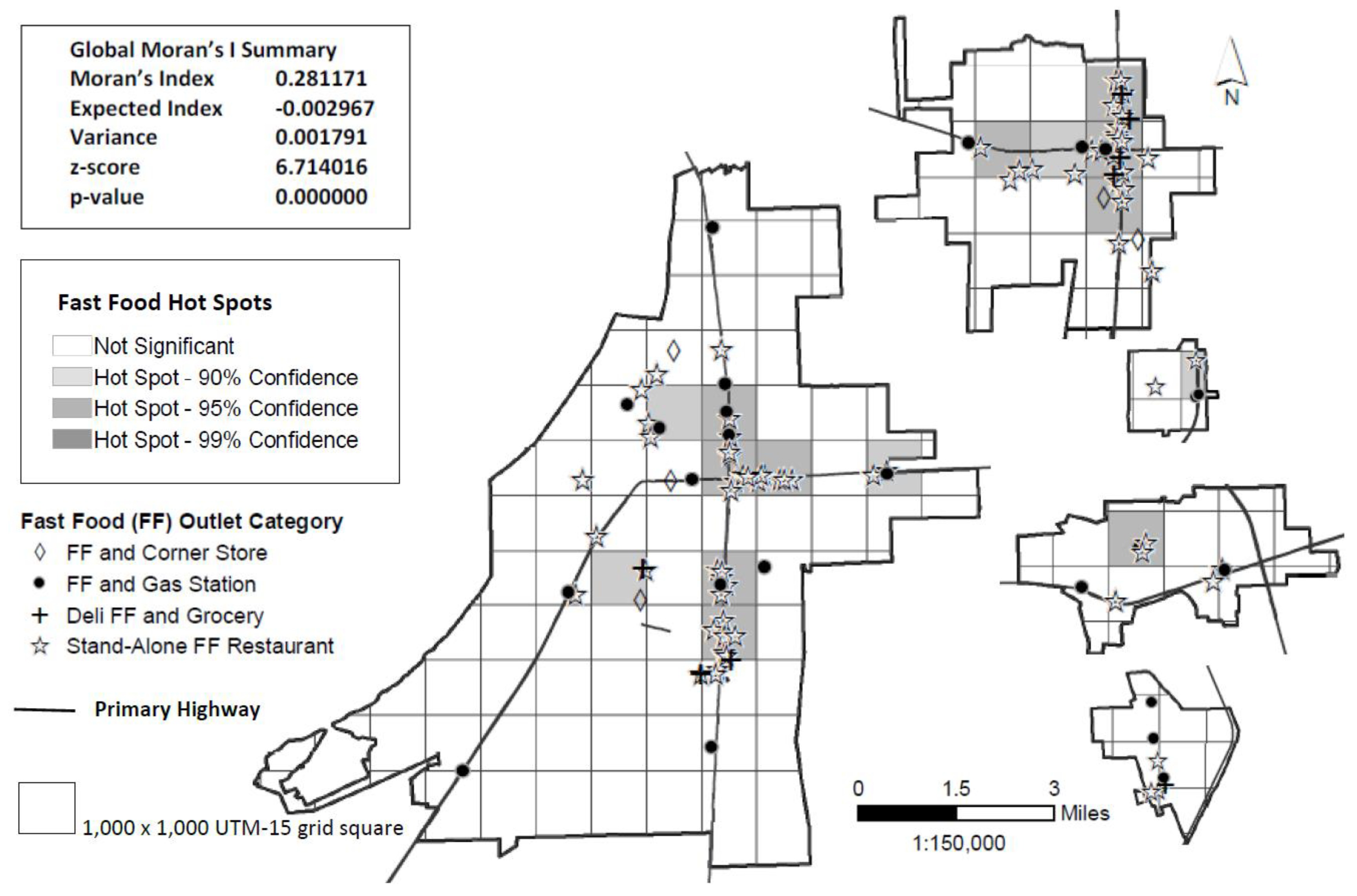
| Frequency of residences within hot spot | ||||||
| In | Adjacent 2 | Not in/adjacent | ||||
| Hot spot type | n | % | n | % | n | % |
| Convenience store | 22 | 32.4 | 29 | 42.6 | 17 | 25.0 |
| Fast food restaurant | 15 | 22.1 | 22 | 32.3 | 31 | 45.6 |
| Census Tract Class | ||||||||
|---|---|---|---|---|---|---|---|---|
| NLILA | LINLA | LIMA | LILA | |||||
| Census Tract | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| African American (%) | 34.0 | 15.56 | 64.1 | 6.64 | 91.3 | 12.01 | 82.3 | 10.38 |
| Below poverty level (%) | 13.3 | 0.05 | 26.3 | 7.00 | 51.3 | 12.84 | 36.4 | 8.05 |
| Participant Residence | ||||||||
| Distance (miles) to closest | ||||||||
| Grocery store | 1.3 | 0.27 | 2.0 | 1.18 | 0.9 | 0.34 | 2.2 | 3.00 |
| Convenience store | 0.5 | 0.28 | 0.6 | 0.25 | 0.3 | 0.13 | 0.5 | 0.24 |
| Full-service restaurant | 0.7 | 0.27 | 1.1 | 0.72 | 0.6 | 0.30 | 1.7 | 2.80 |
| Fast food restaurant | 0.6 | 0.31 | 0.8 | 0.42 | 0.3 | 0.13 | 0.5 | 0.22 |
| n | % | n | % | n | % | n | % | |
| Overall | 3 | 4.4 | 5 | 7.4 | 30 | 44.1 | 30 | 44.1 |
| Convenience store hot spot | 0 | 0.0 | 0 | 0.0 | 13 | 43.3 | 9 | 30.0 |
| Fast food restaurant hot spot | 0 | 0.0 | 0 | 0.0 | 9 | 30.0 | 6 | 20.0 |
| Convenience Store Hot Spot | |||||
|---|---|---|---|---|---|
| Component | No (n = 46) | Yes (n = 22) | |||
| (score range) | Mean | SD | Mean | SD | p1 |
| Total vegetable (0–5) | 1.9 | 1.37 | 2.2 | 1.44 | 0.790 |
| Empty calories (0–20) | 11.8 | 5.78 | 9.2 | 5.44 | 0.044 |
| Total (0–100) | 42.8 | 14.10 | 42.8 | 9.75 | 0.500 |
| Median | IQR | Median | IQR | p2 | |
| Greens and beans (0–5) | 0.0 | 0.00 | 0.0 | 0.00 | 0.487 |
| Total fruit (0–5) | 0.0 | 2.49 | 0.1 | 3.01 | 0.254 |
| Whole fruit (0–5) | 0.0 | 2.47 | 0.0 | 4.67 | 0.273 |
| Whole grains (0–10) | 0.0 | 3.40 | 0.0 | 4.27 | 0.402 |
| Dairy (0–10) | 3.4 | 6.04 | 3.5 | 2.90 | 0.435 |
| Total protein foods (0–5) | 5.0 | 0.78 | 5.0 | 1.23 | 0.357 |
| S&P protein foods (0–5) | 0.0 | 0.89 | 0.0 | 0.00 | 0.023 |
| Fatty acids (0–10) | 6.3 | 7.32 | 5.0 | 7.21 | 0.310 |
| Sodium (0–10) | 1.8 | 4.79 | 2.9 | 5.21 | 0.155 |
| Refined grains (0–10) | 5.8 | 5.36 | 6.9 | 4.82 | 0.097 |
| Fast food hot spot | |||||
| No (n = 53) | Yes (n = 15) | ||||
| Mean | SD | Mean | SD | p1 | |
| Total vegetable (0–5) | 1.9 | 1.39 | 2.3 | 1.41 | 0.839 |
| Empty calories (0–20) | 11.3 | 6.13 | 9.5 | 4.01 | 0.141 |
| Total (0–100) | 42.9 | 13.63 | 42.4 | 9.57 | 0.447 |
| Median | IQR | Median | IQR | p2 | |
| Greens and beans (0–5) | 0.0 | 0.00 | 0.0 | 0.00 | 0.205 |
| Total fruit (0–5) | 0.0 | 2.30 | 2.3 | 5.00 | 0.059 |
| Whole fruit (0–5) | 0.0 | 1.90 | 0.0 | 4.94 | 0.181 |
| Whole grains (0–10) | 0.0 | 4.46 | 0.0 | 4.02 | 0.465 |
| Dairy (0–10) | 3.3 | 5.55 | 3.7 | 2.64 | 0.500 |
| Total protein foods (0–5) | 5.0 | 0.78 | 5.0 | 4.61 | 0.278 |
| S&P protein foods (0–5) | 0.0 | 0.89 | 0.0 | 0.00 | 0.015 |
| Fatty acids (0–10) | 6.4 | 7.24 | 4.5 | 8.28 | 0.137 |
| Sodium (0–10) | 2.1 | 4.79 | 1.9 | 5.21 | 0.388 |
| Refined grains (0–10) | 6.1 | 6.58 | 6.9 | 4.34 | 0.196 |
| Census tract | |||||
| LIMA (n = 30) | LILA (n = 30) | ||||
| Component | Mean | SD | Mean | SD | p3 |
| Total vegetable (0–5) | 1.7 | 1.25 | 2.3 | 1.54 | 0.132 |
| Empty calories (0–20) | 9.6 | 6.46 | 12.8 | 4.57 | 0.028 |
| Total (0–100) | 41.3 | 13.57 | 45.0 | 10.98 | 0.243 |
| Median | IQR | Median | IQR | p4 | |
| Greens and beans (0–5) | 0.0 | 0.00 | 0.0 | 0.00 | 0.278 |
| Total fruit (0–5) | 0.0 | 2.30 | 0.1 | 4.40 | 0.072 |
| Whole fruit (0–5) | 0.0 | 0.00 | 0.0 | 3.03 | 0.029 |
| Whole grains (0–10) | 1.3 | 5.09 | 0.0 | 3.67 | 0.356 |
| Dairy (0–10) | 2.9 | 4.35 | 3.7 | 4.96 | 0.830 |
| Total protein foods (0–5) | 5.0 | 1.61 | 5.0 | 0.78 | 0.583 |
| S&P protein foods (0–5) | 0.0 | 0.00 | 0.0 | 0.89 | 0.243 |
| Fatty acids (0–10) | 5.7 | 7.90 | 6.5 | 6.38 | 0.396 |
| Sodium (0–10) | 3.5 | 4.10 | 0.0 | 3.62 | 0.015 |
| Refined grains (0–10) | 7.0 | 4.91 | 5.7 | 6.74 | 0.598 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodman, M.; Thomson, J.; Landry, A. Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots. Int. J. Environ. Res. Public Health 2020, 17, 3354. https://doi.org/10.3390/ijerph17103354
Goodman M, Thomson J, Landry A. Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots. International Journal of Environmental Research and Public Health. 2020; 17(10):3354. https://doi.org/10.3390/ijerph17103354
Chicago/Turabian StyleGoodman, Melissa, Jessica Thomson, and Alicia Landry. 2020. "Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots" International Journal of Environmental Research and Public Health 17, no. 10: 3354. https://doi.org/10.3390/ijerph17103354
APA StyleGoodman, M., Thomson, J., & Landry, A. (2020). Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots. International Journal of Environmental Research and Public Health, 17(10), 3354. https://doi.org/10.3390/ijerph17103354