Complexity and Community Context: Learning from the Evaluation Design of a National Community Empowerment Programme

 , and
, and 
Abstract
1. Introduction
Conceptually, it (the assertion) frames health matters embedded in a community ecology that includes local conditions, community history, relations among subgroups in the community, relations between community groups and groups external to the community (including relationships with community intervention researchers), local resources, networks and their social capital, and effects of macrosystem policies on community life [24].
2. Background
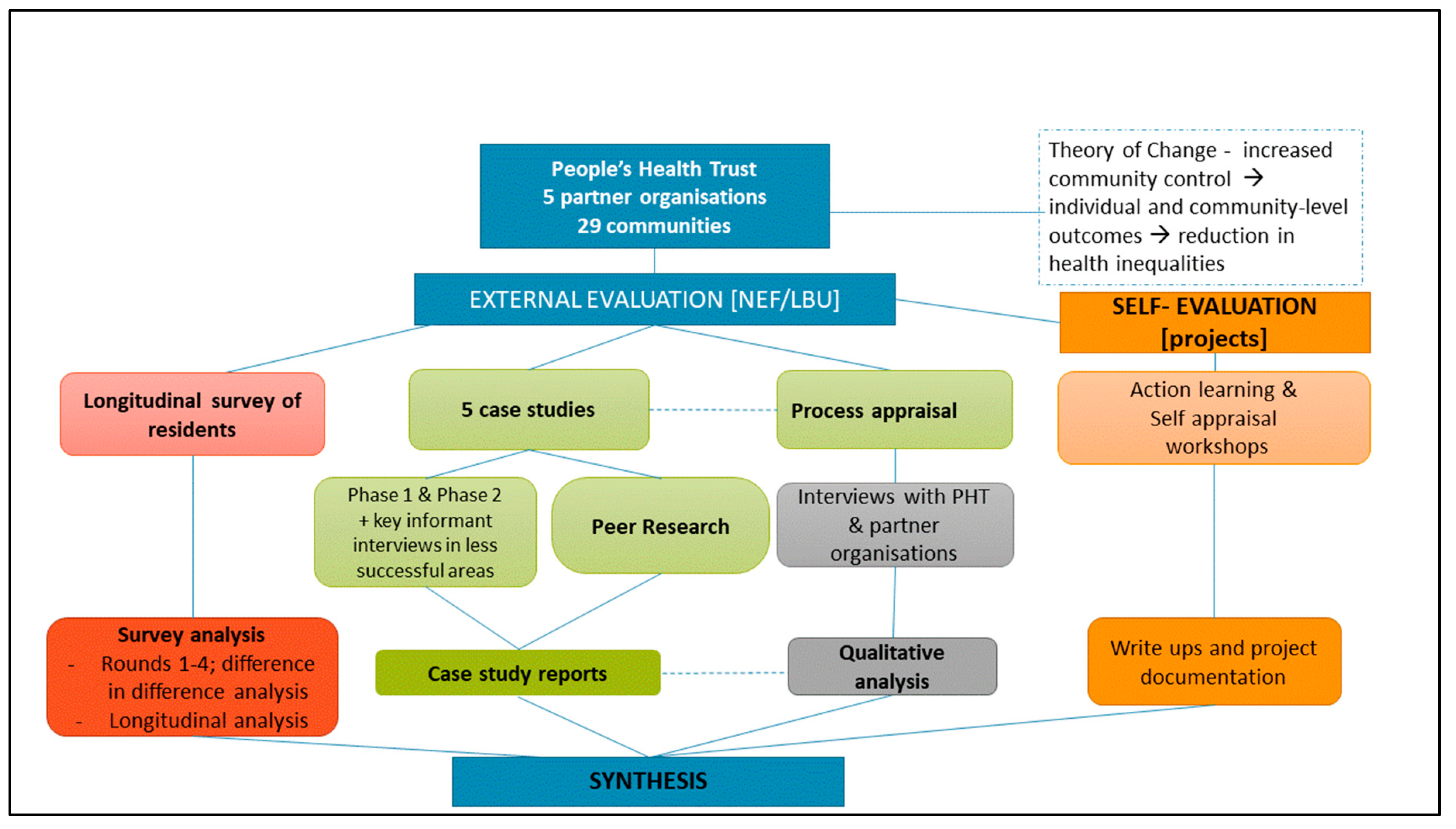
3. Evaluation Design & Methods
- (a)
- Case studies of Local People intervention communities: The case studies formed a major part of the qualitative fieldwork within the overall evaluation with the aim of providing an in-depth analysis of how the initiative worked in and for communities experiencing disadvantage (neighbourhoods and communities of interest). Using a multiple case study design [37], five case studies were undertaken in communities receiving Local People funding. The sampling strategy aimed to select a varied sample of areas, taking into account geographical spread, type of area (urban, rural and coastal) and the supporting national partner organisation. Sites were excluded where there had been major delays with activities, although key informant interviews were later undertaken with a sample of projects in this category. Drawing on traditions of qualitative, naturalistic enquiry [38], the primary research methods were semi-structured individual interviews and group interviews with project staff, local partner representatives and community members, including those involved and not involved in Local People activities. Data collection took place in two phases, with the research team undertaking a number of visits to each community over the course of the project. In the first phase, researchers attended meetings, community events or went on resident-led walks to familiarise themselves with the area [39]. The sample for each case study was selected through discussion with the project leads and following this orientation period. Individuals were invited to participate in the study and with consent, all interviews and focus groups were digitally recorded. Researchers also took field notes of their observation and reflexive memos.
- (b)
- Peer research: Each case study site also undertook some peer (participatory) research [40] supported by the research team. The peer research element aligned to the empowerment goals of the Local People programme [30]. The aims were to build local evaluation skills and capacity and to work collaboratively with residents who wished to collect data on the reach and impact of the case study projects. In each area, a preparatory workshop was held and between four and ten local people were recruited who later undertook peer research. These peer researchers decided the focus of the data collection, in most instances the reach of the initiative and barriers to involvement, and then did a small number of informal interviews in the community. Peer researchers discussed their findings at a final workshop run by the research team. In one case study site, an external exhibition was held.
- (c)
- A longitudinal survey: A questionnaire-based survey of project participants and residents was undertaken across all 29 neighbourhoods (or projects with communities of interest) receiving funding. Projects used a self-completion questionnaire that was administered at four points in the programme. Questions covered demographic variables, type of participation in the local project, views of the neighbourhood and questions about the shorter-term individual outcomes, including confidence, social connectedness, knowledge and skills. The questionnaire drew on verified questions from existing national surveys, mostly the Community Life survey [41]. All project leads were contacted and encouraged to distribute the questionnaire to residents who had some involvement in the programme or programme activities. Questionnaires were administered through paper copies or online if preferred.
- (d)
- Process appraisal: A further strand of the evaluation was the process appraisal. This focused on understanding how Local People worked through the different levels of the programme: funder, national organisation, local project support and communities. In addition to data gathered through case studies, key informant interviews were conducted with national and local leads working in the five national partner organisations.
Analysis and Synthesis
4. Results—Understanding Study Contexts
There’s lot to link in with on a good day. The bad side of it I think is it depends on how much money you’ve got or how ill you are or what the nature of the particular illness is—it can be really hard to access those things. It kind of changes from being an amazing place to a place that’s a bit shit. (Case study E)
When schools broke up for holiday this year the following week the number of people in food banks almost doubled. It’s because the kids are having breakfast club and lunch [in school]. People are really living in poverty and can’t afford to even feed their children. It is so expensive to live these days; you have nurses using food banks. People have got a good salary but by the time you run your house, you pay your bills and everything, you’ve got nothing left over to buy bloody food. (Case study C)
Both areas don’t have a community centre, as such. They have a library and they have lots of churches, but they don’t have a thriving community hub where people can go to meet and go to groups and catch up with the people. (Case study B)
We can be on one estate and say, ‘oh, you know just over the road…’ ‘No, no, I’m not crossing the road, we’re not crossing that bridge”. (Case study A)
Respondent 1: “The people are friendly. Everyone knows everyone. ”Respondent 2: “You find that with the poorer communities though. In essence they are closer and more connected.” (Case study C)
“Community spirit is probably at an all time low”. (Case study A)
“…the communities here, they’re ex-mining communities, I think people have grown up and moved on and people have found themselves lonely and, you know, within their own community lonely and I think there’s something lacking in terms of how do we bring those people together.” (Case study D)
I think we do tend to be very defensive of the area because we are so used to our reputation. Wherever you go, people say things like ‘don’t go up there the wheels will be stolen off your car’. (Case study C)
We have got […] just down the road, big city, beautiful city, a lot of the resources go to that and since we became an authority … we all feel very strongly but […] takes all the money and we are left with the crumbs and anything that’s rubbish. (Case study A)
So there’s this great sense of connected and belonging, I think, despite all the pressures and despite all the, whatever poverty means, despite all those, sort of, economic pressures, there is a sense of community. (Case study D)
“I think there’s a barrier in-between our older generation and our younger generation, if I’m honest. I think the older generation see these younger ones as trouble makers, some of them, but when they get to know them they’re lovely, and that’s how it is.” (Case study D)“So in a way we had a strong community and people will get involved if there is an issue. If there is issues they’ll come and get involved but if there is no issue they’re just quite happy to go along you know.“ (Case study A)
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smith, R.D.; Petticrew, M. Public health evaluation in the twenty-first century: Time to see the wood as well as the trees. J. Public Health 2010, 32, 2–7. [Google Scholar] [CrossRef]
- Rutter, H.; Savona, N.; Glonti, K.; Bibby, J.; Cummins, S.; Finegood, D.T.; Greaves, F.; Harper, L.; Hawe, P.; Moore, L.; et al. The need for a complex systems model of evidence for public health. Lancet 2017, 390, 2602–2604. [Google Scholar] [CrossRef]
- Local Government Association. Health in All Policies: A Manual for Local Government; Local Government Association: London, UK, 2016. [Google Scholar]
- Sims, J.; Aboelata, M.J. A System of Prevention: Applying a Systems Approach to Public Health. Health Promot. Pract. 2019, 20, 476–482. [Google Scholar] [CrossRef]
- World Health Organization. Health in All Policies. Helsinki Statement. Framework for Country Action; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization Regional Office for Europe. Health 2020: A European Policy Framework Supporting Action Across Government and Society for Health and Well-Being; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Carey, G.; Malbon, E.; Carey, N.; Joyce, A.; Crammond, B.; Carey, A. Systems science and systems thinking for public health: A systematic review of the fiel. BMJ Open 2015, 5, e009002. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P. Lessons from compLex interventions to improve health. Am. Rev. Public Health 2015, 36, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P.; Sheill, A.; Riley, T. Theorising interventions as events in systems. Am. J. Community Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, N.K. One step back toward the future of health promotion: Complexity-informed health promotion. Health Promot. Int. 2019, 34, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef]
- South, J.; Phillips, G. Evaluating community engagement as part of the public health system. J. Epidemiol. Community Health 2014, 68, 692–696. [Google Scholar] [CrossRef]
- Rifkin, S.B. Examining the links between community participation and health outcomes: A review of the literature. Health Policy Plan. 2014, 29, ii98–ii108. [Google Scholar] [CrossRef]
- South, J.; Bagnall, A.M.; Stansfield, J.A.; Southby, K.J.; Mehta, P. An evidence-based framework on community centred approaches for health: England, UK. Health Promot. Int. 2019, 34, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Wallerstein, N. Empowerment to reduce health disparities. Scand. J. Public Health 2002, 30, 72–77. [Google Scholar] [CrossRef]
- Laverack, G. Improving health outcomes through community empowerment: A review of the literature. J. Health Popul. Nutr. 2006, 24, 113–120. [Google Scholar] [PubMed]
- Laverack, G.; Pratley, P. Quantitative and qualitative methods to measure community empowerment at a national level. In Health Evidence Network (HEN) Synthesis Report 59; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Whitehead, M.; Pennington, A.; Orton, L.; Nayak, S.; Petticrew, M.; Sowden, A.; White, M. How could differences in ‘control over destiny’ lead to socio-economic inequalities in health? A synthesis of theories and pathways in the living environment. Health Place 2016, 39, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Mead, E.L.; Gittelsohn, J.; Roache, C.; Corriveau, A.; Sharma, S. A Community-Based, Environmental Chronic Disease Prevention Intervention to Improve Healthy Eating Psychosocial Factors and Behaviors in Indigenous Populations in the Canadian Arctic. Health Educ. Behav. 2013, 40, 592–602. [Google Scholar] [CrossRef] [PubMed]
- Rosato, M. A framework and methodology for differentiating community intervention forms in global health. Community Dev. J. 2015, 50, 244–263. [Google Scholar] [CrossRef]
- Cyril, S.; Smith, B.J.; Renzaho, A.M. Systematic review of empowerment measures in health promotion. Health Promot. Int. 2016, 31, 809–826. [Google Scholar] [CrossRef]
- Mason, A.R.; Carr Hill, R.; Myers, L.A.; Street, A.D. Establishing the economics of engaging communities in health promotion: What is desirable, what is feasible? Crit. Public Health 2008, 18, 285–297. [Google Scholar] [CrossRef]
- Draper, A.K.; Hewitt, G.; Rifkin, S. Chasing the dragon: Developing indicators for the assessment of community participation in health programmes. Soc. Sci. Med. 2010, 71, 1102–1109. [Google Scholar] [CrossRef]
- Trickett, E.J.; Beehler, S.; Deutsch, C.; Green, L.W.; Hawe, P.; McLeroy, K.; Miller, R.L.; Rapkin, B.D.; Schensul, J.J.; Schulz, A.J.; et al. Advancing the science of community-level interventions. Am. J. Public Health 2011, 101, 1410–1419. [Google Scholar] [CrossRef]
- Raphael, D.; Bryant, T. The limitations of population health as a model for the new public health. Health Promot. Int. 2002, 17, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Lankelly Chase. Lankelly Chase Foundation: Theory of Change V1.0; Lankelly Chase: London, UK, 2015. [Google Scholar]
- UCL Institute of Equity. Review of Social Determinants and the Health Divide in the WHO European Region: Executive Summary; World Health Organization Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Durie, R.; Wyatt, K. Connecting communities and complexity: A case study in creating the conditions for transformational change. Crit. Public Health 2013, 23, 174–187. [Google Scholar] [CrossRef]
- Orton, L.; Halliday, E.; Collins, M.; Egan, M.; Lewis, S.; Ponsford, R.; Powell, K.; Salway, S.; Townsend, A.; Whitehead, M.; et al. Putting context centre stage: Evidence from a systems evaluation of an area based empowerment initiative in England. Crit. Public Health 2016, 27, 477–489. [Google Scholar] [CrossRef]
- People’s Health Trust, What We Do. Available online: https://www.peopleshealthtrust.org.uk/about-us/what-we-do (accessed on 25 October 2019).
- O’Mara-Eves, A.; Brunton, G.; Oliver, S.; Kavanagh, J.; Jamal, F.; Thomas, J. The effectiveness of community engagement in public health interventionsfor disadvantaged groups: A meta-analysis. BMC Public Health 2015, 15, 129. [Google Scholar] [CrossRef] [PubMed]
- Brunton, G.; Caird, J.; Kneale, D.; Thomas, J.; Richardson, M. Review 2: Community Engagement for Health via Coalitions, Collaborations and Partnerships. A Systematic Review and Meta-Analysis; EPPI-Centre; University of London: London, UK, 2015. [Google Scholar]
- The Marmot Review. Fair Society, Healthy Lives. The Marmot Review. In Strategic Review of Health Inequalities in England Post-2010; The Marmot Review: London, UK, 2010. [Google Scholar]
- Social Research Association. Ethical Guidelines. 2003. Available online: https://the-sra.org.uk/common/Uploaded%20files/ethical%20guidelines%202003.pdf (accessed on 22 November 2019).
- Leech, N.L.; Onwuegbuzie, A.J. A typology of mixed methods research designs. Qual. Quant. 2009, 43, 265–275. [Google Scholar] [CrossRef]
- Judge, K.; Bauld, L. Strong theory, flexible methods: Evaluating complex community-based initiatives. Crit. Public Health 2001, 11, 19–38. [Google Scholar] [CrossRef]
- Yin, Y.K. Case Study Research: Design and Methods, 4th ed.; Sage: London, UK, 2009. [Google Scholar]
- Silverman, D. Intrepreting Qualitative Data. Methods for Analyzing Talk, Text and Interaction, 3rd ed.; Sage: London, UK, 2006. [Google Scholar]
- Sharpe, P.A.; Greaney, M.L.; Lee, P.R.; Royce, S.W. Assets-oriented community assessment. Public Health Rep. 2000, 115, 205–211. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. Using community-based participatory research to address health disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef]
- Department for Digital, Culture, Media & Sport, and Office for Civil Society. Community Life Survey. Available online: https://www.gov.uk/government/collections/community-life-survey--2 (accessed on 26 October 2019).
- Clarke, C.L.; Braun, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage: London, UK, 2013. [Google Scholar]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis. A Methods Sourcebook, 3rd ed.; Sage: Los Angeles, CA, USA, 2014. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Button, D.; Woodward, J.; Quick, A.; Coan, S.; Heisse, C.; Trigwell, J.; Southby, K.; Bagnall, A.-M.; South, J. An Evaluation of People’s Health Trust’s Local People Programme; New Economics Foundation Leeds Beckett University: London, UK, in press.
- Egan, M.; Penney, T.; Anderson de Cuevas, R.; Er, V.; Orton, L.; White, M.; Lock, K.; Cummins, S.; Savona, N.; Whitehead, M.; et al. NIHR SPHR Guidance on Systems Approaches to Local Public Health Evaluation; National Institute for Health Research School of Public Health Research: London, UK, 2019. [Google Scholar]
- Connell, J.P.; Kubisch, A.C. Applying a Theory of Change Approach to the Evaluation of Comprehensive Community Initiatives: Progress, Prospects and Problems, in New Approaches to Evaluating Community Initiatives; Fulbright-Anderson, K., Kubisch, A., Connell, J., Eds.; The Aspen Institute: Washington, DC, USA, 1988. [Google Scholar]
- Orton, L.; Ponsford, R.; Egan, M.; Halliday, E.; Whitehead, M.; Popay, J. Capturing complexity in the evaluation of a major area-based initiative in community empowerment: What can a multi-site, multi team, ethnographic approach offer? Anthropol. Med. 2019, 26, 48–64. [Google Scholar] [CrossRef]
- Conn, E. Community Engagement in the Social Eco-System Dance, in Third Sector Research Centre Discussion Paper; Third Sector Research Centre Discussion Paper: Birmingham, UK, 2011. [Google Scholar]
- Blamey, A.; Mackenzie, M. Theories of change and realistic evaluation: Peas in a pod or apples and oranges? Evaluation 2007, 13, 439–455. [Google Scholar] [CrossRef]
- Halliday, E.; Popay, J.; Anderson de Cuevas, R.; Wheeler, P. The elephant in the room? Why spatial stigma does not receive the attention it deserves. J. Public Health 2018. [Google Scholar] [CrossRef]
- Cornwall, A. Unpacking ‘Participation’: Models, meanings and practices. Community Dev. J. 2008, 43, 269–283. [Google Scholar] [CrossRef]
- Whitesell, N.R.; Mousseau, A.; Parker, M.; Rasmus, S.; Allen, J. Promising Practices for Promoting Health Equity through Rigorous Intervention Science with Indigenous Communities. Prev. Sci. 2018, 1–8. [Google Scholar] [CrossRef]
- South, J.; Jones, R.; Stansfield, J.; Bagnall, A.-M. What quantitative and qualitative methods have been developed to measure health-related community resilience at a national and local level? In Health Evidence Network (HEN) Synthesis Report 60; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]


{kind=link}
| Case Study Sites | Local Project Aims | |
|---|---|---|
| A | Two neighbourhoods in the North West of England form the project area. It is an industrial area in decline, with high unemployment and low skilled jobs. Previously based around the docks, the focus of the area is now an out of town shopping centre. There are green spaces and good access to the countryside but a railway and a motorway divide the area. New people are arriving, but their stay is often short-term. | To improve the physical infrastructure of the area, enhance social spaces, make it more attractive and a better place to walk and cycle. Aimed at all residents living in the neighbourhoods. Supported by Sustrans. |
| B | On the outskirts of a large town in Scotland, two neighbourhoods form the project area. These are surrounded by green space and overlook the sea. Historically separate, the two neighbourhoods are linked by an area of woodland. Much of the current housing is former council owned, often terraced and a large new housing estate is being built. Wage stagnation and austerity has affected residents with many ‘just getting by’. | To get people involved in their community to help make it a better place ‘where they’re happier and more connected and where they feel they have a say’. Aimed at all residents living in the neighbourhoods. Supported by The Conservation Volunteers. |
| C | Two neighbourhoods form the project area. Set atop a hill in a city in Wales, the area has attractive views and convenient access to the city. Poverty rates are high with many residents having insufficient income. Food poverty is an issue and there are concerns for the future. | To support local residents to design and lead activities to improve the area for living and working in. Aimed at all residents living in the neighbourhoods. Supported by The Youth Sport Trust. |
| D | The project area is part of a small town in the West Midlands. The area is semi-rural. Housing is good quality and includes a former mining estate. Industries have shut and unemployment is high. There are limited opportunities for young people and reported low aspirations. The population is largely White British and with a high proportion of older people. | To improve health and wellbeing by connecting people back into community life, to be part of a society and to have a voice. The original target audience was 50 years plus, but this was broadened slightly to more inter-generational work. Supported by Royal Voluntary Service. |
| E | The project area is a busy, vibrant town on the South coast. Most of the town is not economically disadvantaged but there are pockets of deprivation. While there are liberal attitudes to diversity, there is some reported intolerance towards disability and accessibility to some areas is poor. | To create change, improve quality of life, to take control and make decisions. People with disabilities and unpaid carers are the communities of interest. The project is covers the town. Supported by Scope. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
South, J.; Button, D.; Quick, A.; Bagnall, A.-M.; Trigwell, J.; Woodward, J.; Coan, S.; Southby, K. Complexity and Community Context: Learning from the Evaluation Design of a National Community Empowerment Programme. Int. J. Environ. Res. Public Health 2020, 17, 91. https://doi.org/10.3390/ijerph17010091
South J, Button D, Quick A, Bagnall A-M, Trigwell J, Woodward J, Coan S, Southby K. Complexity and Community Context: Learning from the Evaluation Design of a National Community Empowerment Programme. International Journal of Environmental Research and Public Health. 2020; 17(1):91. https://doi.org/10.3390/ijerph17010091
Chicago/Turabian StyleSouth, Jane, Daniel Button, Annie Quick, Anne-Marie Bagnall, Joanne Trigwell, Jenny Woodward, Susan Coan, and Kris Southby. 2020. "Complexity and Community Context: Learning from the Evaluation Design of a National Community Empowerment Programme" International Journal of Environmental Research and Public Health 17, no. 1: 91. https://doi.org/10.3390/ijerph17010091
APA StyleSouth, J., Button, D., Quick, A., Bagnall, A.-M., Trigwell, J., Woodward, J., Coan, S., & Southby, K. (2020). Complexity and Community Context: Learning from the Evaluation Design of a National Community Empowerment Programme. International Journal of Environmental Research and Public Health, 17(1), 91. https://doi.org/10.3390/ijerph17010091