Occupational Class and Cancer Survival in Korean Men: Follow-Up Study of Nation-Wide Working Population


Abstract
1. Introduction
2. Materials and Methods
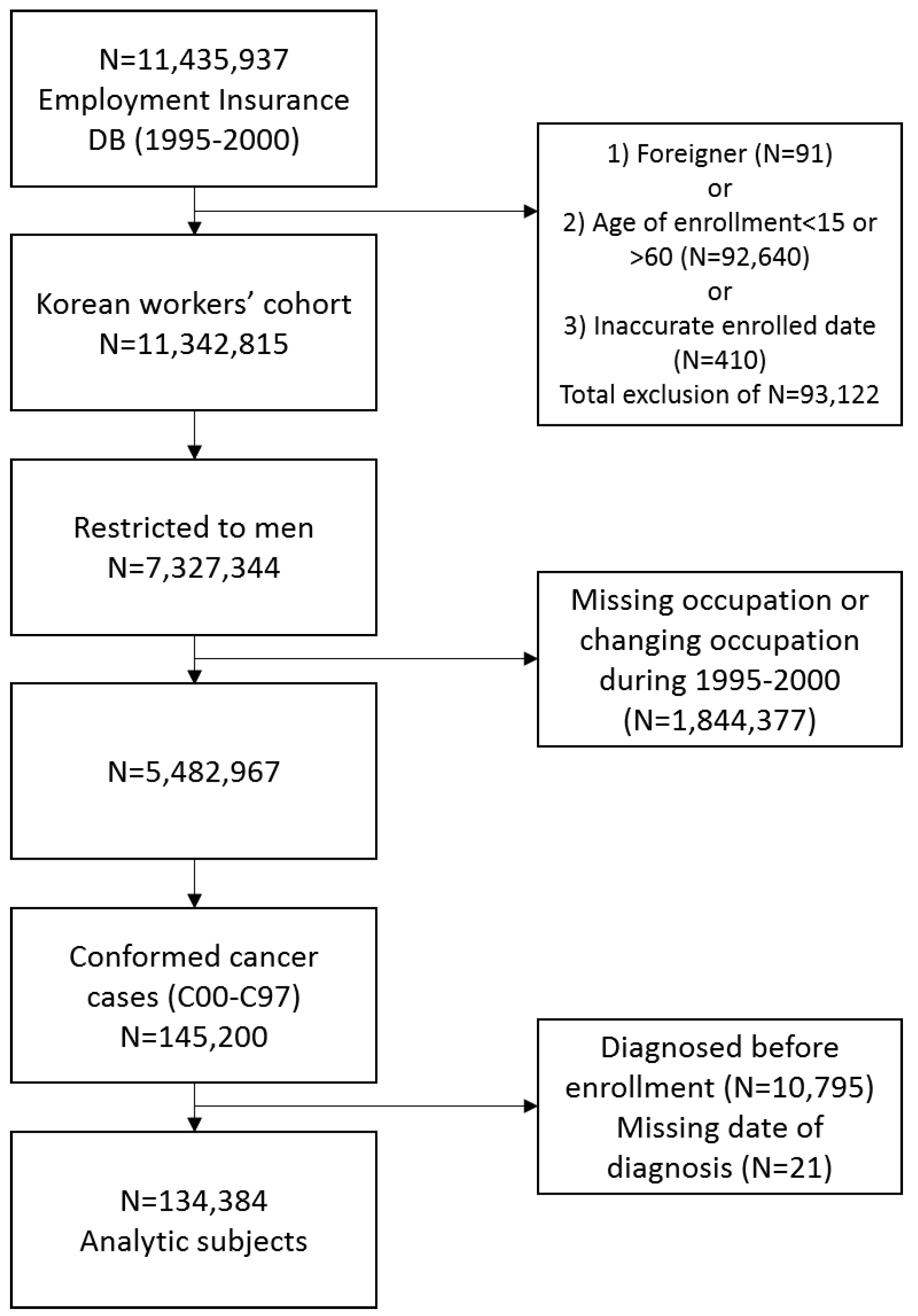
2.1. Data Source and Study Population
2.2. Calculation of Survival
2.3. Occupational Class
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rachet, B.; Woods, L.M.; Mitry, E.; Riga, M.; Cooper, N.; Quinn, M.J.; Steward, J.; Brenner, H.; Estève, J.; Sullivan, R.; et al. Cancer survival in England and Wales at the end of the 20th century. Br. J. Cancer 2008, 99 (Suppl. S1), S2–S10. [Google Scholar] [CrossRef]
- Booth, C.M.; Li, G.; Zhang-Salomons, J.; Mackillop, W.J. The impact of socioeconomic status on stage of cancer at diagnosis and survival: A population-based study in Ontario, Canada. Cancer 2010, 116, 4160–4167. [Google Scholar] [CrossRef] [PubMed]
- Kogevinas, M.; Porta, M. Socioeconomic differences in cancer survival: A review of the evidence. IARC Sci. Publ. 1997, 138, 177–206. [Google Scholar]
- Jansen, L.; Eberle, A.; Emrich, K.; Gondos, A.; Holleczek, B.; Kajüter, H.; Maier, W.; Nennecke, A.; Pritzkuleit, R.; Brenner, H.; et al. Socioeconomic deprivation and cancer survival in Germany: An ecological analysis in 200 districts in Germany. Int. J. Cancer 2014, 134, 2951–2960. [Google Scholar] [CrossRef] [PubMed]
- Chien, L.-H.; Tseng, T.-J.; Tsai, F.-Y.; Wang, J.-H.; Hsiung, C.A.; Liu, T.-W.; Chang, I.-S. Patterns of age-specific socioeconomic inequalities in net survival for common cancers in Taiwan, a country with universal health coverage. Cancer Epidemiol. 2018, 53, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Zaitsu, M.; Kim, Y.; Lee, H.-E.; Takeuchi, T.; Kobayashi, Y.; Kawachi, I. Occupational class differences in pancreatic cancer survival: A population-based cancer registry-based study in Japan. Cancer Med. 2019, 8, 3261–3268. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.K.; Hyun, J.J.; Kim, S.Y.; Jung, S.W.; Koo, J.S.; Kim, J.H.; Yim, H.J.; Lee, S.W. Influence of socioeconomic status on survival and clinical outcomes in patients with advanced gastric cancer after chemotherapy. Oncol. Res. Treat. 2014, 37, 310–314. [Google Scholar] [CrossRef]
- Jang, J.S.; Shin, D.G.; Cho, H.M.; Kwon, Y.; Cho, D.H.; Lee, K.B.; Park, S.S.; Yoon, J.; Jang, Y.S.; Kim, I.M. Differences in the Survival of Gastric Cancer Patients after Gastrectomy according to the Medical Insurance Status. J. Gastric Cancer 2013, 13, 247–254. [Google Scholar] [CrossRef]
- Jang, B.-S.; Chang, J.H. Socioeconomic status and survival outcomes in elderly cancer patients: A national health insurance service-elderly sample cohort study. Cancer Med. 2019, 8, 3604–3613. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Hwang, S.-S.; Yoo, K.-Y.; Kim, C.-Y. Contribution of income-related inequality and healthcare utilisation to survival in cancers of the lung, liver, stomach and colon. J. Epidemiol. Community Health 2012, 66, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Fujishiro, K.; Xu, J.; Gong, F. What does “occupation” represent as an indicator of socioeconomic status?: Exploring occupational prestige and health. Soc. Sci. Med. 2010, 71, 2100–2107. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.-W.; Park, S.; Kong, H.-J.; Won, Y.-J.; Lee, J.Y.; Seo, H.G.; Lee, J.-S. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2009. Cancer Res. Treat. 2012, 44, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-E.; Kim, H.-R.; Chung, Y.K.; Kang, S.-K.; Kim, E.-A. Mortality rates by occupation in Korea: A nationwide, 13-year follow-up study. Occup. Environ. Med. 2016, 73, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.-W.; Won, Y.-J.; Oh, C.-M.; Kong, H.-J.; Lee, D.H.; Lee, K.H. Community of Population-Based Regional Cancer Registries Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2014. Cancer Res. Treat. 2017, 49, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.M.; Rachet, B.; Coleman, M.P. Origins of socio-economic inequalities in cancer survival: A review. Ann. Oncol. 2006, 17, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Suh, M.; Song, S.; Cho, H.N.; Park, B.; Jun, J.K.; Choi, E.; Kim, Y.; Choi, K.S. Trends in Participation Rates for the National Cancer Screening Program in Korea, 2002–2012. Cancer Res. Treat. 2017, 49, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.-S.; Kim, M.-G.; Kang, M.-R.; Shin, M.-H.; Choi, J.-S. Difference of stage at cancer diagnosis by socioeconomic status for four target cancers of the National Cancer Screening Program in Korea: Results from the Gwangju and Jeonnam cancer registries. J. Epidemiol. 2017, 27, 299–304. [Google Scholar] [CrossRef]
- Kim, J.-Y.; Kang, H.-T. Association between Socioeconomic Status and Cancer Screening in Koreans over 40 Years in Age Based on the 2010-2012 Korean National Health and Nutrition Examination Survey. Korean J. Fam. Med. 2016, 37, 287–292. [Google Scholar] [CrossRef]
- Jung, M. Breast, prostate, and thyroid cancer screening tests and overdiagnosis. Curr. Probl. Cancer 2017, 41, 71–79. [Google Scholar] [CrossRef]
- Lee, H.-E.; Zaitsu, M.; Kim, E.-A.; Kawachi, I. Cancer incidence by occupation in Korea: Longitudinal analysis of a nationwide cohort. Saf. Health Work. (accepted). [CrossRef]
- Quaglia, A.; Lillini, R.; Mamo, C.; Ivaldi, E.; Vercelli, M. Socio-economic inequalities: A review of methodological issues and the relationships with cancer survival. Crit. Rev. Oncol. Hematol. 2013, 85, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Lyratzopoulos, G.; Barbiere, J.M.; Rachet, B.; Baum, M.; Thompson, M.R.; Coleman, M.P. Changes over time in socioeconomic inequalities in breast and rectal cancer survival in England and Wales during a 32-year period (1973-2004): The potential role of health care. Ann. Oncol. 2011, 22, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, D.; de Mestral, C.; Bochud, M.; Bartley, M.; Kivimäki, M.; Vineis, P.; Mackenbach, J.; Stringhini, S. The contribution of health behaviors to socioeconomic inequalities in health: A systematic review. Prev. Med. 2018, 113, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Avci, N.; Hayar, M.; Altmisdortoglu, O.; Tanriverdi, O.; Deligonul, A.; Ordu, C.; Evrensel, T. Smoking habits are an independent prognostic factor in patients with lung cancer. Clin. Respir. J. 2017, 11, 579–584. [Google Scholar] [CrossRef]
- Parsons, A.; Daley, A.; Begh, R.; Aveyard, P. Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis: Systematic review of observational studies with meta-analysis. BMJ 2010, 340, b5569. [Google Scholar] [CrossRef]
- Abe, H.; Aida, Y.; Ishiguro, H.; Yoshizawa, K.; Miyazaki, T.; Itagaki, M.; Sutoh, S.; Aizawa, Y. Alcohol, postprandial plasma glucose, and prognosis of hepatocellular carcinoma. World J. Gastroenterol. 2013, 19, 78–85. [Google Scholar] [CrossRef]
- Dasgupta, P.; Turrell, G.; Aitken, J.F.; Baade, P.D. Partner status and survival after cancer: A competing risks analysis. Cancer Epidemiol. 2016, 41, 16–23. [Google Scholar] [CrossRef]
- Simpson, M.C.; Challapalli, S.D.; Cass, L.M.; Zahirsha, Z.S.; Adjei Boakye, E.; Massa, S.T.; Osazuwa-Peters, N. Impact of gender on the association between marital status and head and neck cancer outcomes. Oral Oncol. 2019, 89, 48–55. [Google Scholar] [CrossRef]
- Choi, K.-H.; Park, J.-H.; Park, J.-H.; Park, J.-S. Psychosocial needs of cancer patients and related factors: A multi-center, cross-sectional study in Korea. Psychooncology 2013, 22, 1073–1080. [Google Scholar] [CrossRef]
- Jung, K.-W.; Won, Y.-J.; Kong, H.-J.; Lee, E.S. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2016. Cancer Res. Treat. 2019, 51, 417–430. [Google Scholar] [CrossRef]
- Lee, E.-Y.; Xuan Mai, T.T.; Chang, Y.; Ki, M. Trends of liver cancer and its major risk factors in Korea. Epidemiol. Health 2015, 37, e2015016. [Google Scholar] [CrossRef] [PubMed][Green Version]




{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Age of Diagnosis | ||
| <20 | 42 | 0.0 |
| 20–29 | 2,156 | 1.6 |
| 30–39 | 13,590 | 10.1 |
| 40–49 | 31,780 | 23.7 |
| 50–59 | 46,729 | 34.8 |
| 60– | 40,087 | 29.8 |
| Year of diagnosis | ||
| 1995–1999 | 19,804 | 14.7 |
| 2000–2004 | 49,771 | 37.0 |
| 2005–2008 | 64,820 | 48.2 |
| Occupational group | ||
| Group 1 (Professionals and managers) | 28,198 | 21.0 |
| Group 2 (Clerks) | 23,937 | 17.8 |
| Group 3 (Service and sales workers) | 8,152 | 6.1 |
| Group 4 (blue-collar workers) | 74,097 | 55.1 |
| Vital status | ||
| Alive | 70,117 | 52.2 |
| Dead | 64,267 | 47.8 |
| cause of death: cancer | 58,332 | (90.8) |
| cause of death: non-cancer | 3,037 | (4.7) |
| cause of death: undefined | 2,898 | (4.5) |
| Total | 134,384 | 100.0 |
| Site of Cancer | N | % |
|---|---|---|
| All cancer (C00–C97) | 134,384 | 100.0 |
| Lip, oral cavity and pharynx (C00–C14) | 3142 | 2.3 |
| Esophagus (C15) | 2192 | 1.6 |
| Stomach (C16) | 32,524 | 24.2 |
| Colon, rectosigmoid junction, rectum (C18–C20) | 18,361 | 13.7 |
| Liver and intrahepatic bile ducts (C22) | 23,170 | 17.2 |
| Gallbladder, other and unspecified parts of biliary tract (C23–C24) | 2632 | 2.0 |
| Pancreas (C25) | 3068 | 2.3 |
| Larynx (C32) | 1496 | 1.1 |
| Trachea, bronchus and lung (C33–C34) | 14,423 | 10.7 |
| Mesothelioma (C45) | 92 | 0.1 |
| Breast (C50) | 102 | 0.1 |
| Prostate (C61) | 3403 | 2.5 |
| Testis (C62) | 443 | 0.3 |
| Kidney (C64) | 3746 | 2.8 |
| Bladder (C67) | 3329 | 2.5 |
| Brain and other parts of central nervous system (C70–C72) | 1775 | 1.3 |
| Thyroid gland (C73) | 6059 | 4.5 |
| Hodgkin lymphoma (C81) | 264 | 0.2 |
| Non-Hodgkin lymphoma (C82–C85, C96) | 3706 | 2.8 |
| Multiple myeloma (C90) | 701 | 0.5 |
| Leukemia (C91–C95) | 2748 | 2.0 |
| Adjusted HR | 95% CI | ||
|---|---|---|---|
| All cancer (C00–C97) | Group 1 | Reference | |
| Group 2 | 1.05 | 1.02–1.08 | |
| Group 3 | 1.38 | 1.33–1.43 | |
| Group 4 | 1.45 | 1.42–1.48 | |
| Lip, oral cavity and pharynx (C00-C14) | Group 1 | Reference | |
| Group 2 | 1.20 | 0.97–1.49 | |
| Group 3 | 1.89 | 1.47–2.42 | |
| Group 4 | 1.78 | 1.51–2.10 | |
| Esophagus (C15) | Group 1 | Reference | |
| Group 2 | 1.14 | 0.91–1.41 | |
| Group 3 | 1.24 | 0.94–1.61 | |
| Group 4 | 1.29 | 1.11–1.51 | |
| Stomach (C16) | Group 1 | Reference | |
| Group 2 | 1.01 | 0.95–1.09 | |
| Group 3 | 1.35 | 1.23–1.47 | |
| Group 4 | 1.31 | 1.24–1.38 | |
| Colon, rectosigmoid junction, rectum (C18–C20) | Group 1 | Reference | |
| Group 2 | 1.15 | 1.05–1.27 | |
| Group 3 | 1.39 | 1.22–1.57 | |
| Group 4 | 1.37 | 1.27–1.47 | |
| Liver and intrahepatic bile ducts (C22) | Group 1 | Reference | |
| Group 2 | 1.06 | 1.01–1.12 | |
| Group 3 | 1.36 | 1.26–1.46 | |
| Group 4 | 1.44 | 1.38–1.50 | |
| Gallbladder, other and unspecified parts of biliary tract (C23–C24) | Group 1 | Reference | |
| Group 2 | 1.14 | 0.96–1.36 | |
| Group 3 | 1.18 | 0.93–1.47 | |
| Group 4 | 1.26 | 1.11–1.44 | |
| Pancreas (C25) | Group 1 | Reference | |
| Group 2 | 1.04 | 0.91–1.19 | |
| Group 3 | 1.23 | 1.03–1.46 | |
| Group 4 | 1.18 | 1.06–1.30 | |
| Larynx (C32) | Group 1 | Reference | |
| Group 2 | 0.94 | 0.57–1.55 | |
| Group 3 | 1.66 | 0.96–2.78 | |
| Group 4 | 1.84 | 1.33–2.60 | |
| Trachea, bronchus and lung (C33–C34) | Group 1 | Reference | |
| Group 2 | 1.10 | 1.02–1.19 | |
| Group 3 | 1.21 | 1.10–1.33 | |
| Group 4 | 1.26 | 1.19–1.33 | |
| Prostate (C61) | Group 1 | Reference | |
| Group 2 | 1.25 | 0.89–1.74 | |
| Group 3 | 2.26 | 1.39–3.52 | |
| Group 4 | 2.35 | 1.85–3.02 | |
| Kidney (C64) | Group 1 | Reference | |
| Group 2 | 0.98 | 0.77–1.24 | |
| Group 3 | 1.19 | 0.84–1.65 | |
| Group 4 | 1.53 | 1.28–1.85 | |
| Bladder (C67) | Group 1 | Reference | |
| Group 2 | 1.04 | 0.76–1.42 | |
| Group 3 | 1.18 | 0.75–1.81 | |
| Group 4 | 1.26 | 1.01–1.60 | |
| Brain and other parts of central nervous system (C70–C72) | Group 1 | Reference | |
| Group 2 | 1.04 | 0.85–1.27 | |
| Group 3 | 1.11 | 0.84–1.45 | |
| Group 4 | 1.22 | 1.04–1.45 | |
| Thyroid gland (C73) | Group 1 | Reference | |
| Group 2 | 1.07 | 0.63–1.79 | |
| Group 3 | 2.59 | 1.25–4.98 | |
| Group 4 | 1.43 | 0.94–2.20 | |
| Non-Hodgkin lymphoma (C82–C85,C96) | Group 1 | Reference | |
| Group 2 | 1.08 | 0.90–1.29 | |
| Group 3 | 1.46 | 1.15–1.84 | |
| Group 4 | 1.46 | 1.27–1.68 | |
| Leukemia (C91–C95) | Group 1 | Reference | |
| Group 2 | 1.04 | 0.89–1.23 | |
| Group 3 | 1.03 | 0.82–1.27 | |
| Group 4 | 1.32 | 1.16–1.50 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-E.; Zaitsu, M.; Kim, E.-A.; Kawachi, I. Occupational Class and Cancer Survival in Korean Men: Follow-Up Study of Nation-Wide Working Population. Int. J. Environ. Res. Public Health 2020, 17, 303. https://doi.org/10.3390/ijerph17010303
Lee H-E, Zaitsu M, Kim E-A, Kawachi I. Occupational Class and Cancer Survival in Korean Men: Follow-Up Study of Nation-Wide Working Population. International Journal of Environmental Research and Public Health. 2020; 17(1):303. https://doi.org/10.3390/ijerph17010303
Chicago/Turabian StyleLee, Hye-Eun, Masayoshi Zaitsu, Eun-A Kim, and Ichiro Kawachi. 2020. "Occupational Class and Cancer Survival in Korean Men: Follow-Up Study of Nation-Wide Working Population" International Journal of Environmental Research and Public Health 17, no. 1: 303. https://doi.org/10.3390/ijerph17010303
APA StyleLee, H.-E., Zaitsu, M., Kim, E.-A., & Kawachi, I. (2020). Occupational Class and Cancer Survival in Korean Men: Follow-Up Study of Nation-Wide Working Population. International Journal of Environmental Research and Public Health, 17(1), 303. https://doi.org/10.3390/ijerph17010303